

Abstract
Supratentorial anaplastic ependymoma is an uncommon tumor which can rarely present as a cyst with mural nodule on imaging. Authors present this unusual radiological appearance of supratentorial extraventricular anaplastic ependymoma in a 9-year-old boy.
Keywords: Anaplastic ependymoma, MRI, supratentorial
A 9-year-old boy presented to our outpatient services with complaints of headache in the left frontal region associated with on- and off-vomiting for the last 6 months. Neurological examination was normal except for mild left hemiparesis (4+/5 power, Medical Research Council grading). Magnetic resonance imaging (MRI) of the brain revealed a space occupying lesion in the right posterior frontal region. It was cystic with a small mural nodule on the lateral aspect. It was hypointense on T1W, hyperintense on T2W with mild homogenous contrast enhancement of the mural nodule. The mural nodule was hyperintense on fluid attenuation inversion recovery (FLAIR) images. The tumor was intra-axial, extraventricular [Figure 1]. The possibility of pilocytic astrocytoma was entertained and the patient was operated through a fronto-parietal quadrangular flap craniotomy and gross total excision of the tumor was carried out. The tumor had a large cystic component containing xanthochromic fluid and a solid nodule of 2 × 1 cm. The tumor was well demarcated from the surrounding brain parenchyma and heterogenous in consistency. There was no communication to the ventricular system. Microsurgical gross total excision of the tumor was carried out. Histo-pathological examination revealed a malignant neoplasm with dense cellularity and formation of perivascular pseudorosettes along with microvascular proliferation and necrosis. Immunohistochemistry revealed epithelial membrane antigen (EMA). The tumor cells were negative for glial fibrillary acid protein (GFAP). The Ki-67/MIB-1 index was 25%. Overall, histological features were suggestive of anaplastic ependymoma with clear cell change [Figures 2–f]. The patient was discharged on 7th postoperative day and referred for radiotherapy.
Figure 1.
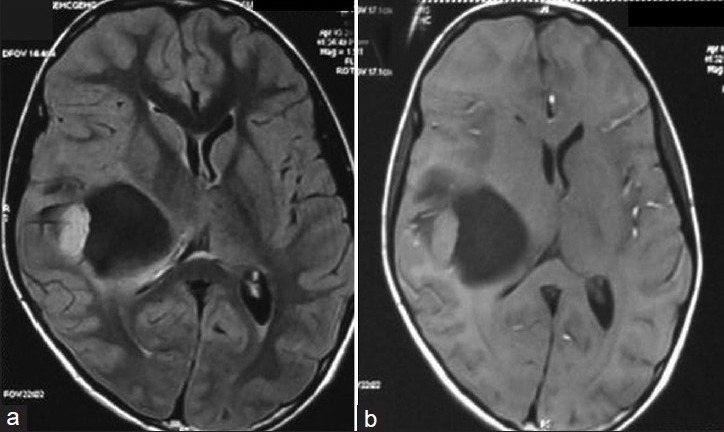
(a and b) FLAIR and T1 contrast MR images of the patient showing a cyst with enhancing mural nodule in the right posterior frontal region. Note that there is no communication to the ventricle
Figure 2.
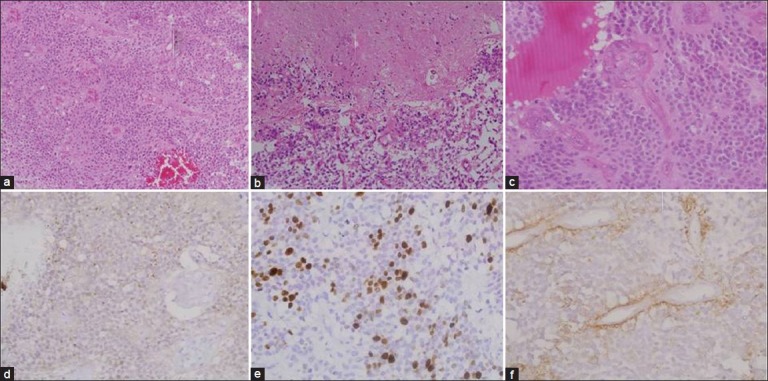
(a—f) Photomicrograph showing a highly cellular tumor with perivascular arrangement (a) (H and E ×40). The tumor cells have clear cytoplasm and irregularly clumped chromatin with areas of necrosis (b) and endothelial proliferation (c) (H and E ×200). Immunohistochemistry for EMA showing dot positivity (d), MIB-1 indices of 25% (e), and GFAP negativity (f). Overall histological features are suggestive of anaplastic ependymoma with clear cell change
Ependymomas comprise around 10% of pediatric intracranial tumors. They are usually located in the infratentorial compartment. However, approximately 30% of intracranial ependymomas are supratentorial.[1] As per the published literature, supratentorial ependymomas differ from infratentorial ependymomas in various ways. A higher proportion of supratentorial ependymomas are high grade tumors (50–60%) compared to infratentorial ependymomas (10–40%).[2] Also, supratentorial ependymomas are mostly extraventricular compared to infratentorial ependymomas which are intraventricular in more than 80% cases.[3]
The classical radiological feature of a cyst with mural nodule is usually observed with low grade pathologies such as pilocytic astrocytoma. The other differential diagnoses include a ganglioglioma, hemangioblastoma and pleomorphic xanthoastrocytoma.[4] It is very unusual for a supratentorial anaplastic ependymoma to present in such a manner. Furie and Provenzale[5] analyzed the MRI appearance of supratentorial ependymomas and concluded that MR contrast enhancement pattern in supratentorial ependymoma can be heterogenous enhancement of a solid lesion, heterogenous enhancement of a cystic/solid lesion and although rare, an enhancing nodule in the wall of a cyst.
To conclude, supratentorial extraventricular anaplastic ependymoma is an uncommon tumor which can rarely present as a cyst with mural nodule on imaging. In any case of a supratentorial cyst with mural nodule, the possibility of supratentorial ependymoma should be considered.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
References
- 1.Van Tassel P, Lee YY, Bruner JM. Supratentorial ependymomas: computed tomographic and pathologic correlations. J Comput Assist Tomogr. 1986;10:157–65. doi: 10.1016/0149-936x(86)90069-x. [DOI] [PubMed] [Google Scholar]
- 2.Silverman CL, Thomas PR, Cox W. Ependymomas. In: Deutsch M, editor. Management of childhood brain tumours. Boston: Kluwer Academic; 1990. pp. 369–82. [Google Scholar]
- 3.Palma L, Paolo C, Cantore G. Supratentorial ependymomas of the forst two decades of life. Long-term follow-up of 20 cases (including two subependymomas) Neurosurgery. 1993;32:169–75. doi: 10.1227/00006123-199302000-00003. [DOI] [PubMed] [Google Scholar]
- 4.Lin E, Escott E, Garg K, Bleicher A. Practical differential diagnosis for CT and MRI. New York: Thieme Inc; 2008. Tumor and tumor-like lesions; pp. 17–20. [Google Scholar]
- 5.Furie DM, Provenzale JM. Supratentorial ependymomas and subependymomas: CT and MR appearance. J Comput Assist Tomogr. 1995;19:518–26. doi: 10.1097/00004728-199507000-00002. [DOI] [PubMed] [Google Scholar]