

Abstract
Context:
Carcinoma in an early stage of development is hard to detect clinically because the lesion may not be palpable and color of the lesional tissue is not necessarily different from the color of the surrounding mucosa. In order to improve the efficacy of the diagnosis, techniques are being developed to complement clinical examination and to facilitate the identification of initial carcinomas.
Aims:
To find out the efficacy of chemiluminescent illumination (ViziLite™) for the diagnosis in precancer and cancer patients and compare this result to toluidine blue staining and oral exfoliative cytology.
Materials and Methods:
This study was done in 3 groups. Each group consists of 10 cases. Group I consists of normal appearing mucosa. Group II and III consist of clinically diagnosed pre-cancer and clinically suggestive of cancer respectively. Chemiluminescent illumination, toluidine blue supravital staining, oral exfoliative cytology and biopsy were performed in all cases.
Statistical analysis used:
SPSS version 10.05 was used to calculate positive and negative predictive values.
Results:
In Group I, all 10 patients showed negative result to ViziLite™. 8 patients showed positivity and 2 patients showed negativity to ViziLite™ test in Group II. 9 patients were positive and one patient was negative for ViziLite™.
Conclusions:
Chemiluminescent illumination test was sensitive for precancerous and cancerous lesions, which presented as keratotic lesions and red-white lesions. It showed negative result to erosive lesions. Toluidine blue staining test was reliable in precancerous and cancerous lesions, which present as erosive and red-white lesions. It showed negative result to keratotic lesions. Oral exfoliative cytology has diagnostic value in cancer patients than in precancer patients. These Results indicate that chemiluminescent illumination test is relatively reliable and accurate than toluidine blue staining test and useful chair side diagnostic test.
Keywords: Chemiluminescent illumination, Oral exfoliative cytology, Toluidine blue
INTRODUCTION
Oral cancer is usually first diagnosed when it becomes symptomatic and approximately two thirds of the patients present with advanced disease, regional metastasis and consequently poor prognosis.[1] Oral precancers associated with habits which occur in the oral cavity include leukoplakia and oral submucous fibrosis. 8-10% of these eventually progress to malignancy. The risk of development of carcinoma within an area of leukoplakia is 5 times higher than in those without leukoplakia. Malignant transformation has been reported in 43% of dysplastic leukoplakia cases.[2] It is therefore important to identify these lesions early to enable management.
Conventional visual inspection and palpation of oral soft tissues for the early detection of premalignant or malignant changes have their limitations. The adjunctive application of technology to highlight such lesions may increase the diagnostic yield.[3]
A number of techniques have been developed to supplement clinical examination and improve the diagnosis of early oral malignancy.[1] They include (a) chemiluminescent illumination (ViziLite™, a trademark of Zila, Inc., Phoenix, USA), (b) toluidine blue supravital staining test and (c) oral exfoliative cytology.
ViziLite™ is an oral examination device that is claimed to improve identification, evaluation and monitoring of oral mucosal abnormalities in those with increased risk of oral cancer. The specific ViziLite™ wavelength is absorbed by normal cells and reflected by abnormal cells due to their higher nuclear-cytoplasmic ratio. As a result, atypical mucosal abnormalities appear bright white.[4]
The topical application of toluidine blue, an acidophilic, metachromatic nuclear stain has been used in the in vivo evaluation of neoplastic changes of the cervix (Richart, 1963) and the oral cavity (Shedd et al., 1967, Myers, 1970). Areas of carcinoma have a strong affinity for the dye, whereas the normal mucosa does not. This response permits detection of small and early lesions and also permits their surface delineation.[5]
Oral exfoliative cytology examines the morphological characteristics of exfoliated (or) scraped off superficial cells of the oral mucosa. The exfoliated cells are stained by Papanicolaou stain.[6] Exfoliative cytology is of diagnostic references in ulcerated oral carcinomas and erosive leukoplakias and is of importance in mass screening programme (or) where biopsy is not feasible.
As with all cancers, early detection is the key to successful treatment and reduction in morbidity. Use of exfoliative cytology and toluidine blue in vivo for selection of biopsy sites are widely reported in the literature. There is paucity of information regarding the use of ViziLite™ as an aid in early detection of mucosal abnormalities particularly in identifying potential malignant lesions. The present study was done to compare the usefulness and validity of ViziLite™, toluidine blue in vivo application and oral exfoliative cytology with gold standard of biopsy.
MATERIALS AND METHODS
This study was done in 3 groups. Each group consists of 10 cases. Group I consists of normal appearing mucosa. Group II and III consist of clinically diagnosed pre-cancer and clinically suggestive of cancer respectively. Chemiluminescent illumination [Figure 1], toluidine blue supravital staining, oral exfoliative cytology and biopsy were performed in all cases. A detailed case history was recorded. The patient consent was obtained.
Figure 1.
Chemiluminescent illumination kit
Chemiluminescent illumination (ViziLite™)
The patients were instructed to rinse their mouth with the ViziLite™ rinse recommended (1% acetic acid solution). They were asked to swish the rinse all over the mouth for one minute and expectorate the contents. The examination room was dimmed to minimize ambient light. The ViziLite™ capsule was activated and assembled with the ViziLite™ retractor. The oral cavity was re-examined using the illumination from the ViziLite™ assembly. The observations were recorded accordingly and duly photographed. The ViziLite™ device was discarded. The presence of “acetowhite” lesion after one minute rinse with 1% acetic acid solution was considered as a “positive” test [Figure 2]. The absence of such findings was considered as a “negative” test.
Figure 2.
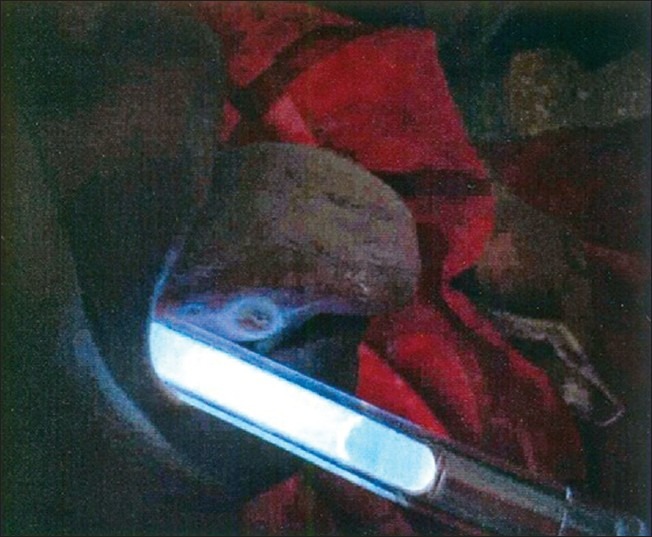
Chemiluminescent illumination positivity
Toluidine blue
The toluidine blue technique was performed after the ViziLite™ procedure. The intraoral lesion was cleaned with 1% acetic acid. A cotton applicator tip was soaked with toluidine blue and applied over the lesion for 30 seconds. 1% acetic acid on a cotton applicator tip was used for 30 seconds to remove excess stain from the lesion. The observations were recorded in detail and lesion was photographed. Lesions that exhibited dark blue (or) stippled staining were considered as a “positive” test [Figure 3], while those that stained faintly (or) not at all were considered as “negative” test.
Figure 3.

Toluidine blue positivity
Oral exfoliative cytology
The patients were asked to rinse their mouth thoroughly with water. A wet wooden spatula was used to firmly scrape the lesion. The scrapings were smeared onto a glass slide, which was fixed in 95% alcohol for 30 minutes. The slides were stained with Papanicolaou's stain and viewed under a microscope. Interpretation was done based on cytological diagnostic criteria.[7]
All the patients were subjected to subsequent biopsy. The areas as indicated by the positivity of ViziLite™ and toluidine blue were the preferable sites chosen for the biopsy. If the areas indicated by ViziLite™ and toluidine blue were not same, biopsy was performed from each site indicated by their positivity.
RESULTS
Data analysis and data base management was done using SPSS version 10.05. Descriptive analysis, sensitivity and specificity were calculated. Positive and negative predictive values were also calculated.
Group I
All 10 patients showed negative result to ViziLite™ and toluidine blue staining test. All 10 cases exhibit Class I cytology and normal epithelium in histopathology [Table 1].
Table 1.
Comparison of ViziLite™ and toluidine blue positivity in normal epithelium

Group II
8 patients showed positivity and 2 patients showed negativity to ViziLite™ test. These 2 patients exhibited mild dysplasia in histopathology. Of the 8 ViziLite™ positive patients, 4 exhibit Class II cytology. The remaining 4 patients exhibit Class I and Class III cytology equally. Of the 2 ViziLite™ negative patients, one had Class I and other had Class II cytology.
6 patients showed positivity and 4 patients showed negativity to toluidine blue staining test. Of the 4 patients, 3 had mild dysplasia and one case showed moderate dysplasia in histopathology. Of the 6 toluidine blue staining positive patients, 3 had Class II cytology, 2 had Class III cytology and one had Class I cytology. Of the 4 toluidine blue staining negative patients, each two had Class I and Class II cytology [Table 2].
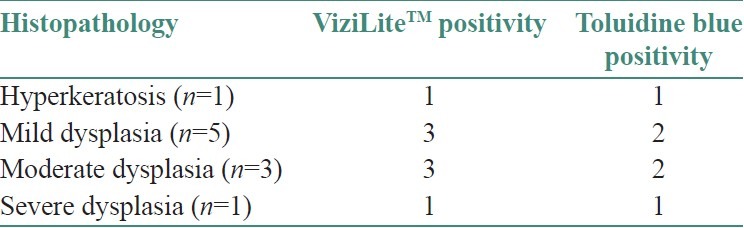
Table 2.
Comparison of ViziLite™ and toluidine blue positivity in precancer
Group III
9 patients were positive for ViziLite™ test and one patient was negative for ViziLite™ test. The negative case was diagnosed as moderately differentiated squamous cell carcinoma. Of these 9 ViziLite™ positive cases, 7 patients had Class III cytology, 2 patients (one patient each) had Class I cytology and Class IV cytology. Cytological findings revealed that the negative case had Class II cytology.
All 10 cases showed positive result when subjected to toluidine blue staining. Of these 10 cases, 7 had Class III cytology, 2 had Class II cytology and one had Class IV cytology [Table 3].
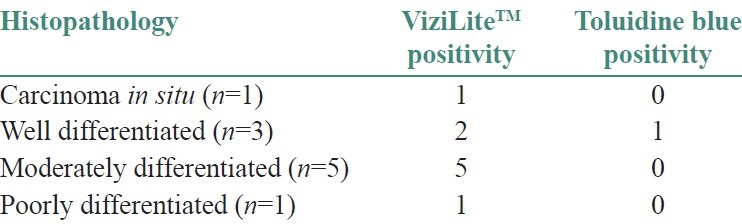
Table 3.
Comparison of ViziLite™ and toluidine blue positivity in oral cancer
DISCUSSION
The early diagnosis and management of carcinoma of the oral cavity is essential and it continues to present a great challenge. Carcinoma in an early stage of development is hard to detect clinically because the lesion may not be palpable and color of the lesional tissue is not necessarily different from the color of the surrounding mucosa.[8] In order to improve the efficacy of the diagnosis, techniques are being developed to complement clinical examination and to facilitate the identification of initial carcinomas.[9]
A non-toxic chemiluminescent light source has been recently used to supplement clinical examination of precancer and cancer lesions. Chemiluminescent (ViziLite™) was first used by Huber et al.[3] to study mucosal abnormalities in populations at increased risk for oral cancer.
One of the procedures in chemiluminescent illumination is acetic acid application. It causes dehydration of the cells and some surface coagulation of cellular proteins, thereby reducing the transparency of the epithelium. These changes are more pronounced in abnormal epithelium due to higher nuclear density and consequently high concentration of proteins.[10]
Thus before subjecting a clinically suspected lesional area suggestive of precancer (or) cancer in the oral mucosa to chemiluminescent light, the patient is asked to rinse the oral cavity with acetic acid. Epithelium with an altered nuclear cytoplasmic ratio will reflect the diffuse, low-level, blue-white chemiluminescent light and will appear sharply demarcated from the adjacent normal epithelium.
In 10 precancer patients, 4 patients had keratotic lesions, 4 had red-white lesions and 2 had erosive lesions clinically. Chemiluminescent light positivity observed in 8 patients, which presented clinically as keratotic and red-white lesions. On histopathological examination, 3 patients showed mild dysplasia, 3 patients showed moderate dysplasia and one showed severe dysplasia. But, one patient, who had a positive chemiluminescence showed hyperkeratosis without dysplastic changes on histopathology and this case was considered as false positive.
Two patients showed negativity to chemiluminescent light, which presented clinically as erosive lesions. On histopathological examination, they exhibited epithelial dysplasia.
In 10 cancer patients, 6 patients presented with non-healing ulcerative lesions clinically surrounded by white keratotic borders, 3 had red-white lesions and one patient had erosive lesions. When these patients were subjected to chemiluminescent light, 9 showed positive result. Of these 9 cases, 3 patients had well differentiated OSCC, 4 patients had moderately differentiated OSCC and one patient had poorly differentiated OSCC. But, one patient showed carcinoma in situ histopathologically.
We considered the result of this case as a false positive. Most probably the site subjected to biopsy in this lesion may not have the representative area to exhibit features of well differentiated OSCC histopathologically. To confirm this, we wanted to repeat the biopsy but the patient was not available for a follow-up. This may be extended to state that chemiluminescent light may be unable to distinguish epithelial dysplasia confined to the basement membrane from that of a well differentiated infiltrating carcinoma.
One patient with a clinically erosive lesion showed negative result to chemiluminescent light. Histopathologically, this patient showed well differentiated OSCC. This case was considered as “negative”. From this, we observed that an erosive lesion when subjected to chemiluminescent light will elicit a false negative result.
Vahidy et al.,[5] Epstein et al.,[11] Warnakulasuriya et al.[12] and Martin[1] have evaluated the efficiency of in vivo staining with toluidine blue in the detection of dysplasias and malignant lesions. Toluidine blue is an acidophilic dye of the thiazine group that selectively stains acetic tissue components such as DNA and RNA. Its use in vivo is based on the fact that dysplastic and anaplastic cells contain quantitatively more nucleic acids than normal tissues. In addition, malignant epithelium may contain intracellular canals that are wider than in normal epithelium and this factor that could enhance the penetration of the dye.[1] Shedd et al.[13] stated that non- dysplastic epithelium fails to retain toluidine blue.
Of the 8 precancer patients who were positive to chemiluminescent light, 4 patients showed positive result to toluidine blue staining test. These patients had red-white lesions clinically. On histopathology, 2 patients showed moderate dysplasia and one patient showed severe dysplasia. But, one patient showed hyperkeratosis without dysplastic changes and this case was considered as “false positive”.
The four patients who were positive to chemiluminescent light showed negative result to toluidine blue staining test. These 4 patients had keratotic lesions clinically and on histopathology, 3 patients showed mild dysplasia and one patient showed moderate dysplasia. The keratotic lesions did not retain toluidine blue stain after rinsing with acetic acid. The false negative result obtained by toluidine blue may limit its use as a diagnostic procedure, which can complement clinical diagnosis.[14]
The two precancer patients in whom the lesional tissue was negative to chemiluminescent light, both showed positive Results to toluidine blue staining. Both patients had erosive lesions clinically.
Warnakulasuriya et al.[12] stated that ulcerative (or) erosive cases of carcinomas and carcinoma in situ retain a dark blue stain obtained following rinsing with toluidine blue. It is strongly indicative of neoplastic disease and warrants further investigations.
Of the 9 cancer patients, all showed positive result when subjected to toluidine blue staining. Of these 9 patients, 5 patients showed moderately differentiated OSCC, 2 patients showed well differentiated OSCC and one patient showed poorly differentiated OSCC on histopathology. But, one cancer patient showed carcinoma in situ histopathologically and this result was considered as false positive.
One patient with clinical diagnosis of oral cancer showed negative result to chemiluminescent light but positive result when subjected to toluidine blue staining. This patient had erosive lesion clinically and showed well differentiated OSCC histopathologically.
The use of exfoliative cytology in diagnosing malignant transformation in oral precancerous lesions, namely in leukoplakias, is still more controversial. False negative cytologic Results in leukoplakia were observed in 62% of the cases.[6]
In this study, of the 8 precancer patients who were positive to chemiluminescent light, 4 patients had Class I cytology and 4 patients had Class II cytology. Clinically, these patients had keratotic lesions and red-white lesions. Of the 2 precancer patients who were negative to chemiluminescent light, both had Class III cytology. These patients had erosive lesions clinically.
Of the 9 cancer patients who were positive to chemiluminescent light, 6 patients had Class III cytology and 3 patients had Class II cytology. These patients had ulcerative lesions with keratotic borders and red-white lesions respectively. One cancer patient who was negative to chemiluminescent light showed Class IV cytology. This patient had erosive lesion clinically.
CONCLUSIONS
Presently, we evaluated 3 diagnostic procedures that have been used as an aid in the diagnosis of oral cancer other than biopsy. Chemiluminescent illumination test was sensitive for precancerous and cancerous lesions, which presented as keratotic lesions and red-white lesions. It showed negative result to erosive lesions. Toluidine blue staining test was reliable in precancerous and cancerous lesions, which present as erosive and red-white lesions. It showed negative result to keratotic lesions. Oral exfoliative cytology has diagnostic value in cancer patients than in precancers patients.
Sensitivity of chemiluminescent light (83.3%) was greater than that of toluidine blue (77.8%) and its positive predictive value (88.2%) and negative predictive value (76.9%) were also high compared to toluidine blue.
These Results indicate that chemiluminescent illumination test is relatively reliable and accurate than toluidine blue staining test and useful chair side diagnostic test.
ACKNOWLEDGEMENT
We sincerely thank Dr. T. Rooban, Dr. S. Nalinkumar and Dr. B. Saravanan for extending their kind support during the study.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Martin IC, Kerawala CJ, Reed M. The application of toluidine blue as a diagnostic adjunct in the detection of epithelial dysplasia. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1998;85:444–6. doi: 10.1016/s1079-2104(98)90071-3. [DOI] [PubMed] [Google Scholar]
- 2.Allen CM. Toluidine blue: Proceed with caution? Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1998;86:255. doi: 10.1016/s1079-2104(98)90168-8. [DOI] [PubMed] [Google Scholar]
- 3.Bánóczy J. Exfoliativecytologic examinations in the early diagnosis of oral cancer. Int Dent J. 1976;26:398–404. [PubMed] [Google Scholar]
- 4.Epstein JB, Oakley C, Millner A, Emerton S, van der Meij E, Le N. The utility of toluidine blue application as a diagnostic aid in patients previously treated for upper oropharyngeal carcinoma. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997;83:537–47. doi: 10.1016/s1079-2104(97)90117-7. [DOI] [PubMed] [Google Scholar]
- 5.Epstein JB, Scully C, Spinelli J. Toluidine blue and Lugol's iodine application in the assessment of oral malignant disease and lesions at risk of malignancy. J Oral Pathol Med. 1992;21:160–3. doi: 10.1111/j.1600-0714.1992.tb00094.x. [DOI] [PubMed] [Google Scholar]
- 6.Huber MA, Bsoul SA, Terezhalmy GT. Acetic acid wash and chemiluminescent illumination as an adjunct to conventional oral soft tissue examination for the detection of dysplasia: A pilot study. Quintessence Int. 2004;35:378–84. [PubMed] [Google Scholar]
- 7.Onofre MA, Sposto MR, Navarro CM. Reliability of toluidine blue application in the detection of oral epithelial dysplasia and in situ and invasive squamous cell carcinomas. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001;91:535–40. doi: 10.1067/moe.2001.112949. [DOI] [PubMed] [Google Scholar]
- 8.Sankaranarayanan R, Wesley R, Somanathan T, Dhakad N, Shyamalakumary B, Amma NS, et al. Visual inspection of the uterine cervix after the application of acetic acid in the detection of cervical carcinoma and its precursors. Cancer. 1998;83:2150–6. [PubMed] [Google Scholar]
- 9.Shafer WG, Hine MK, Levy BM, editors. 4th ed. New Delhi: Saunders; 2003. A Textbook of Oral Pathology. [Google Scholar]
- 10.Shedd DP, Hukill PB, Bahn S, Farraro RH. Further appraisal of in vivo staining properties of oral cancer. Arch Surg. 1967;95:16–22. doi: 10.1001/archsurg.1967.01330130018004. [DOI] [PubMed] [Google Scholar]
- 11.Vahidy NA, Zaidi SH, Jafarey NA. Toludine blue test for detection of carcinoma of the oral cavity: An evaluation. J Surg Oncol. 1972;4:434–8. doi: 10.1002/jso.2930040505. [DOI] [PubMed] [Google Scholar]
- 12.Warnakulasuriya KA, Johnson NW. Sensitivity and specificity of OraScan (R) toluidine blue mouthrinse in the detection of oral cancer and precancer. J Oral Pathol Med. 1996;25:97–103. doi: 10.1111/j.1600-0714.1996.tb00201.x. [DOI] [PubMed] [Google Scholar]
- 13. [Last accessed on 23 December 2007]. Available from: www.zila.com/products/ViziLite .
- 14.Strong MS, Vaughan CW, Incze JS. Toluidine blue in the management of carcinoma of the oral cavity. Arch Otolaryngol Head Neck Surg. 1968;87:527–31. doi: 10.1001/archotol.1968.00760060529017. [DOI] [PubMed] [Google Scholar]