

Abstract
Objectives
The aims of the study were to compare subjective image quality of clinical images obtained with a storage phosphor plate (SPP)-based digital and conventional film-based panoramic system for the visualization of various anatomical structures and to evaluate the effect of various processing algorithms on image interpretation.
Methods
Panoramic radiographs were taken in 42 patients both with film and with a SPP system. SPP images were treated with shadow, sharpen, negative, greyscale sigma and greyscale exponential filters. Four observers subjectively evaluated films and unfiltered and filtered SPP images for the visibility of anatomical structures with various radiodensities as well as for overall image quality on a three-point rating scale. The statistical methods used were Kruskal–Wallis, odds ratio analysis and Cohen's kappa.
Results
No statistically significant difference was found between film and unfiltered digital images except for low-contrast structures (P > 0.05). Film images were preferred for the visibility of low-contrast structures (P < 0.05). Best overall image quality was obtained with sharpened images (P < 0.05) followed by films and unfiltered digital images. Among all filtered images, sharpened ones received the highest ratings for the visibility of all anatomical structures (P < 0.05). The intra- and interobserver agreement ranged between moderate and substantial and between fair and moderate, respectively.
Conclusions
Film and unfiltered SPP-based panoramic images performed equally well in terms of overall quality; however, films were best for the perception of low-contrast structures. The sharpening filter may be recommended for enhancing SPP panoramic images to improve the visual perception of most of the anatomical structures as well as overall quality.
Keywords: radiography, panoramic; radiography, dental, digital; image processing
Introduction
Digital radiography has been a common technique in medicine for many years, but digital systems for dental panoramic radiography have not been available until recently.1,2 Since the introduction of digital extra-oral imaging, scientific research on this topic has been rather limited.3,4 Studies using panoramic images have compared the quality of unfiltered digital images with films, evaluated the effect of dose reduction on the detection of anatomical structures and/or dental pathologies or compared the performance of different panoramic receptors.4–7
It is well known that radiographic recognition of disease requires superior radiographic appearance of normal anatomy. For this purpose, the processing of digital images with the aid of various filters is recommended to produce a “conventional look” while overcoming the limitations of conventional film radiography.8 However, so far, only a few studies have compared the effect of image filters that may enhance the quality of the panoramic image.4,6,9 Although panoramic radiography is not the primary diagnostic yield for approximal caries diagnosis; a recent study focused on the evaluation of filters to maximize the diagnosis of approximal caries.10 The filters enhanced the overall quality of the image but visualization of important structures that may aid in the distinction of pathology from anatomy were not considered. For this purpose, Gijbels et al4 tested the effect of different filters on the overall image quality using a charged-coupled device (CCD)-based panoramic system and reported a significant effect of contrast enhancement. An evaluation of various image filters on visibility of anatomical structures, as well as on overall image quality, using a storage phosphor plate (SPP)-based panoramic system was done in only one study. However, the authors used individually designed algorithms, rather than standard and commonly used filters, for image processing, which makes their results impractical.9
The present study was designed, therefore, to compare subjective image quality of clinical images obtained with SPP-based digital and conventional film-based panoramic systems for the visualization of various anatomical structures; and to evaluate the effect of various processing algorithms on image interpretation.
Materials and methods
Clinical radiographs
Panoramic radiographs of 42 patients (22 female and 20 male) with natural dentition in all quadrants were obtained using both conventional (film) and digital panoramic systems. A minimum of six natural teeth in each quadrant was required as the inclusion criterion. All patients were informed in writing, as well as verbally, about the study and asked to sign a written consent regarding their acceptance to participate. This study was approved by the ethics committee of Ege University (approval date and number: 4 February 2008 – 393/365).
Panoramic films were obtained using Kodak T-MAT G film (Carestream Health Inc., Rochester, NY) while digital panoramic images were taken using the SPP of the Digora PCT system (Soredex Corporation, Helsinki, Finland). Two receptors were placed in the same cassette equipped with a Kodak Lanex medium intensifying screen (Carestream Health Inc., Rochester, NY) and exposed using the OP 100 (GE Healthcare, Tuusula, Finland) panoramic X-ray unit at 70 kV, 16 mA and 17.6 s. All exposures were made by the same radiographic operator.
The technique of placing an imaging plate behind a screen–film combination in a conventional cassette is called the dual-image recording technique. Opaque paper was placed in front of the imaging plate to avoid light exposure to the film from the spontaneous luminescence emitted from the imaging plate during X-ray exposure. The technique is frequently used in medical radiology to evaluate diagnostic image quality and provides two radiographs simultaneously with a single exposure.11,12 It has been proved that the technique offers single-exposure imaging with only nominal degradation in film and SPP image quality, relative to the two standard image counterparts and, therefore, has been adopted as the method of choice in the present study to avoid the added radiation exposure to patients.13,14
After exposure, films were processed in an automatic processor (XR 24; Dürr, Bietigheim, Germany) while phosphor plates were read on a Digora PCT laser scanner. The scanning spatial resolution, which is selectable, was set at high resolution, as recommended by the manufacturer, and the acquired images were saved by means of Digora for Windows software (Soredex Corporation, Helsinki, Finland) and named “original”. Thereafter, the images were enhanced using Digora for Windows software. Five different display modality options were, provided by the software, including shadow, enhancement (hereafter named sharpen), negative, greyscale sigmoidal (hereafter named sigmoidal) and greyscale exponential (hereafter named exponential) modes, as defined by the manufacturer, were used as enhancement filters.
It has been shown that the high-pass filters are preferable for enhancement of bone structures, while contrast enhancement via grey level modifications help to improve local contrast and increase the sensitivity of the human eye to fine details.15,16 Accordingly, shadow and sharpen filters were chosen as the high-pass filters while sigmoidal and exponential type of grey value modifications were chosen to see the effect of contrast change. Negative modification of the images, also known as the inversion or invert algorithm, was also done to test the effect of brightness changes in the dark regions of the image. The negative filter provides a different perception of densities by reversing the greyness of the image, so that what was black becomes white and what was white becomes black (Figure 1).
Figure 1.

Unfiltered and digitally filtered panoramic images of the same patient obtained using a storage phosphor plate (SPP)-based system
The manufacturer of the Digora PCT system claims that the enhancement algorithm makes an image appear sharper.17 It was not possible to obtain detailed information on the nature of this filter; however, images treated with the enhancement filter visually appear sharper and coarse-grained and are, therefore, named sharpen in this study in order to describe the function and the standard name of the filter (Figure 1).
The shadow filter is a high-pass filtering procedure and can be used to visualize the complete course of structures that pass through dark and light regions in a radiograph, for example endodontic files or root fractures and similar pathology. The shadow filter displays the image with an embossed greyscale. The difference between shadow and three-dimensional (3D) emboss filtering is that a residual portion of greyscale remains when using shadow filter. This gives the image an appearance of depth based on the relative densities or greyscale values. The resultant image shows the borderlines of structures regardless of the intensity or regional density differences (Figure 1).
Grey levels of the image can be modified to change the contrast of the image and are used to outline different anatomical structures or properties. In practice, re-mapping of the grey values is generally calculated by the operator using a look-up table (LUT). The LUT represents the transformation that is performed on each pixel on the basis of that intensity value. These grey value transformations may be linear or non-linear.18 The use of a non-linear LUT allows high displayed contrast in some areas of the image while other areas have low displayed contrast.19 Generally, six mathematical functions are used to generate various LUT response curves, two of which are exponential and sigmoidal.20 According to the manufacturer, use of the exponential filter of the Digora PCT system automatically enhances displayed contrast in the high-density (dark) areas of the image, whereas the sigmoidal function enhances both brighter and darker areas of the image, mimicking the general shape of the film–screen Hurter-Driffield curve and produces results that are similar in appearance to film–screen images (Figure 1).21
After the modification of the original digital images with the above-mentioned filters, the total number of original and enhanced images to be assessed by 1 observer was 294 (252 digital (42 unfiltered, 210 filtered) and 42 film).
Image evaluation
Four radiologists with a mean age of 35 ±&<?ENTCHAR hairsp?>6.3 years <?ENTCHAR lpar?>range 30<?ENTCHAR ndash?>43<?ENTCHAR rpar?> and mean clinical experience of 11.25<?ENTCHAR hairsp?><?ENTCHAR plusmn?><?ENTCHAR hairsp?>6.3 years <?ENTCHAR lpar?>range 6<?ENTCHAR ndash?>19<?ENTCHAR rpar?> acted as evaluators.</p><p id="para18">Films were mounted in non<?ENTCHAR hyphen?>transparent frames, placed on a masked light box and examined in a room where the light was dimmed. SPP images were exported as uncompressed tagged image file format <?ENTCHAR lpar?>TIFF<?ENTCHAR rpar?> files and imported into image presentation software <?ENTCHAR lpar?>PowerPoint 2000<?ENTCHAR semi?> Microsoft Corporation, Redmond, WA<?ENTCHAR rpar?> to show each panoramic image centred against a black background. This procedure ensured the standard presentation of images and that images with different filters were blinded to observers. Digital images were viewed on a 19 inch high<?ENTCHAR hyphen?>resolution <?ENTCHAR lpar?>super video graphics array<?ENTCHAR rpar?> colour liquid crystal monitor with a resolution of 1280<?ENTCHAR hairsp?><?ENTCHAR times?><?ENTCHAR hairsp?>1024 pixels and 256 grey levels <?ENTCHAR lpar?>Philips, 190S8FB<?ENTCHAR sol?>27, New York, NY<?ENTCHAR rpar?>. Images were displayed in a pre<?ENTCHAR hyphen?>set randomized order. Observation conditions were optimized through the use of the same computer monitor for display of the images. Viewing distance was kept constant to about 50<?ENTCHAR emsp14?>cm for all observers and the lights were subdued during observations. A total of 1176 digital and film radiographs were evaluated by 4 observers.</p><p id="para19">To assess the subjective image quality of panoramic images, the observers were asked to score the visibility of relevant anatomical structures as well as the overall quality of the image. Written and verbal instructions for image evaluation were given to each observer. Five anatomical structures and the overall image quality were chosen for evaluation<?ENTCHAR colon?> floor of maxillary sinus <?ENTCHAR lpar?>FMS<?ENTCHAR rpar?><?ENTCHAR semi?> periodontal ligament space <?ENTCHAR lpar?>PDL<?ENTCHAR rpar?> of the mandibular right first molar<?ENTCHAR semi?> inferior border of mandible <?ENTCHAR lpar?>IMB<?ENTCHAR rpar?><?ENTCHAR semi?> dentino<?ENTCHAR hyphen?>enamel junction <?ENTCHAR lpar?>DEJ<?ENTCHAR rpar?> of the maxillary right first molar; and root canal space (RCS) of the mandibular left first molar. If the molar tooth to be evaluated was missing, the second molar of the same quadrant was evaluated instead. Anatomical structures were chosen on the basis of their image characteristics providing both low-(PDL and RCS) and high-contrast (FMS and IMB) details.
DEJ appears radiopaque on radiographs and is generally regarded as a high-contrast anatomical structure.22 However, the perception of the apparently simple black and white shadow of a particular anatomical structure can be affected considerably by the density of surrounding shadows.23 As stated by Whaites23, the contrast between adjacent structures can alter the perceived density of one or both of them. Accordingly, as the contrast between enamel and dentine is lower than the contrast between root canal and dentine, the former is perceived as harder than the latter. Therefore, DEJ was not classified as either a high- or low-contrast structure and was evaluated individually in the present study.
Observers were asked to independently score all images using a 3-point rating scale:
0 = important structures are not diagnostic (not visualized) (poor)
1 = important structures are diagnostic but could be improved (moderate)
2 = important structures are optimally visualized (excellent).
The evaluation process was repeated a week later by the same four observers to test the intra-observer agreement.
Statistical analysis
The mean of the subjective image quality scores by the four observers was calculated for each anatomical structure as well for each image type. Scores of 1 and 2 were considered to be diagnostically acceptable, as all the important anatomical structures described above were, by definition, visualized.
The differences between the original, filtered and film images were assessed using the Kruskal–Wallis test. Pair-wise comparisons were made by odds ratio analysis. A 95% confidence interval was applied to determine statistical significance. Intrarater and interrater reliability was tested by Cohen's kappa coefficient.
Results
No statistically significant difference was found between film and unfiltered (original) digital images on depicting anatomical structures, except for PDL and RCS (P < 0.05) (Figures 2–4). Film images received significantly higher scores for the visualization of two low-contrast structures (PDL and RCS) (P < 0.05).
Figure 2.
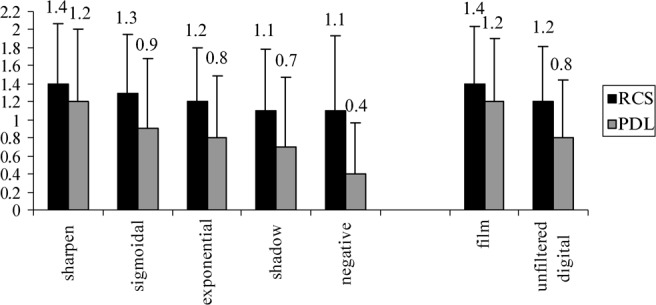
Mean scores of four observers showing the performance of panoramic films and unfiltered and filtered storage phosphor plate (SPP)-based digital panoramic images for the perception of low-contrast anatomical structures; RCS, root canal space; PDL, periodontal ligament space
Figure 4.
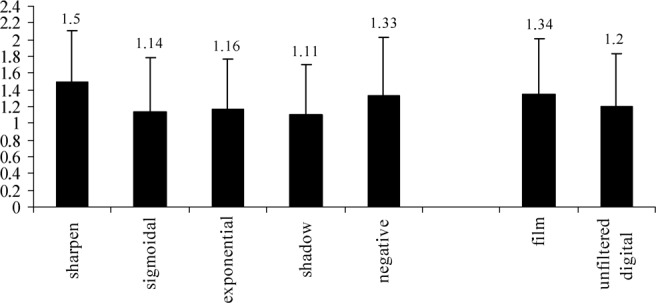
Mean scores of four observers showing the performance of panoramic films and unfiltered and filtered storage phosphor plate (SPP)-based digital panoramic images for the perception of dentino-enamel junction
Best overall image quality was obtained with sharpen filtered images (P < 0.05) followed by films and unfiltered digital images. No significant difference was observed between film and unfiltered images with regard to the overall image quality (P > 0.05). Exponential, sigmoidal and shadow filters received the next best scores for overall image quality (Figure 5). No difference was found between the scores of sigmoidal and exponential filters (P > 0.05). The shadow filter showed significantly lower scores than sigmoidal and exponential filters, whereas the negative filter received the lowest number of scores for overall image quality (P < 0.05) (Figure 5).
Figure 5.
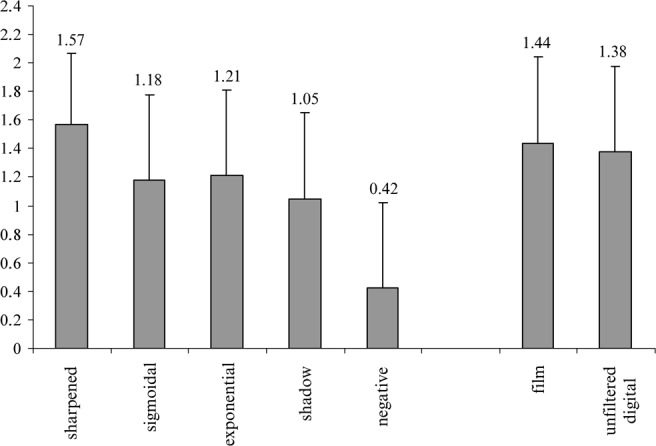
Mean overall image quality scores of four observers showing the performance of panoramic films and unfiltered and filtered storage phosphor plate (SPP)-based digital panoramic images
When sharpened images were compared with films it was observed that sharpened images received the highest ratings for high-contrast structures and DEJ, but received identical scores to film for both low-contrast structures (P > 0.05). The differences between the mean scores of films and sharpened images were significant for high-contrast structures, DEJ and overall image quality (P < 0.05) (Figures 3–5).
Figure 3.
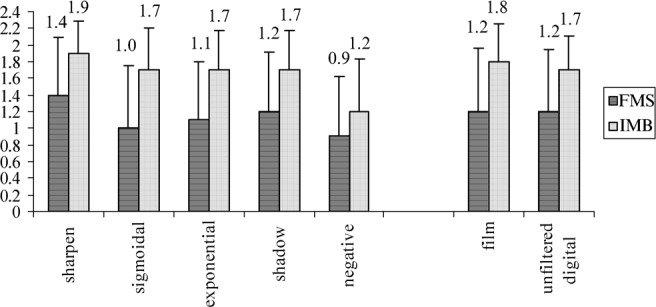
Mean scores of four observers showing the performance of panoramic films, and unfiltered and filtered storage phosphor plate (SPP)-based digital panoramic images for the perception of high-contrast anatomical structures; FMS, Floor of maxillary sinus; IMB, inferior border of mandible
When only the filtered images were compared with each other, the sharpened images received the highest scores for the depiction of high-contrast (FMS and IMB) and low-contrast structures (PDL and RCS) as well as DEJ (P < 0.05) (Figures 2–4). The same order of filters was observed for the visualization of low-contrast structures (Figure 2). Sigmoidal, exponential, shadow and negative filters consecutively followed the sharpen filter for the depiction of PDL and RCS (Figure 2). No significant difference was observed between sigmoidal–exponential and exponential–shadow filters (P > 0.05) whereas a significant difference was found for sigmoidal–shadow and sigmoidal–negative filters for the visualization of PDL and RCS, with the sigmoidal filter showing significantly better scores than the shadow and negative filters (P < 0.05). The difference between exponential and negative filtered images was significant only for PDL (P < 0.05) (Figure 2).
The order of filters obtained for the visualization of high-contrast structures was also identical (Figure 3). When the filters, other than the sharpen filter, were listed with regard to the visualization of FMS, the shadow filtered images received the second best scores, followed by exponential (P > 0.05) and then sigmoidal filtered images (P < 0.05). The mean number of scores obtained for shadow, exponential and sigmoidal filtered images was the same for IMB (P > 0.05). Although not significantly different from exponential and sigmoidal filtered images, negative images received the lowest scores for the depiction of FMS (P > 0.05). On the other hand, negative filtered images showed significantly lower scores than shadow, exponential and sigmoidal filtered images for IMB (P < 0.05) (Figure 3).
When filters were compared for the perception of DEJ, it was observed that negative images received the second best scores after sharpened images, followed by exponential and sigmoidal filtered images, whereas the shadow filtered images received the lowest scores (Figure 2). Although the difference between negative and exponential filtered images was significant (P < 0.05), no significant difference was present among exponential, sigmoidal and shadow filtered images for DEJ (P > 0.05).
The intra-observer agreement ranged from moderate to substantial (range, 0.527–0.756) and the interobserver agreement ranged from fair to moderate (range, 0.282–0.456).
Discussion
The present study evaluated the differences in subjective image quality of film and SPP-based digital panoramic images for the visualization of various anatomical structures, plus the effect of various filters on image interpretation. Overall image quality ratings and visualization of high-contrast details as well as DEJ showed equal performance for unfiltered SPP images and conventional panoramic films. This finding is in line with the general conclusions of many studies reporting equal diagnostic capacity of conventional panoramic films and unfiltered panoramic images.2,3,6 On the other hand, superiority of film images was observed for the visualization of low-contrast structures.
The ability of an imaging system or receptor to reproduce anatomy is limited by the unavoidable degradation of the input information that may manifest as blurring, increase in noise or reduction in contrast.24 In comparing the visibility in low-contrast structures, however, two physical factors are of primary importance: spatial resolution and low-contrast detectability. The resolution of Digora SPP panoramic images (4–6 lp mm−1) has been reported to be lower than that of films (6–9 lp mm−1).25 Conversely, better low-contrast detectability for SPPs, probably as a result of better X-ray detection efficiency, was demonstrated. It was also known that there is more noise in the digital images.6 Since SPPs, were exposed by the wasted radiation exiting from the back of the film–screen combination with the dual-cassette technique used in the present study, reduced percent of entrance dose rendered images with higher noise. Accordingly, the low spatial resolution and high noise level of SPP images may have resulted in lower preference for visualization of low-contrast details as noise is particularly significant when the objects being imaged are small in size and/or have relatively low contrast.26
Enhancing the SPP-based digital images with the sharpen filter revealed an increase in the scores and resulted in equal preference with panoramic films for the perception of low-contrast structures. On the other hand, sharpened images were superior to film and all of the other filters for the evaluation of overall image quality and visualization of high-contrast structures and DEJ. Psychophysical experiments indicate that photographic and radiographic images with enhanced edges are often more pleasing to the human visual system than the original images.27 Wenzel and Hintze showed that the sharpening filter helps to identify anatomical features, periapical bone lesions and caries using intraoral receptors.28 Conversely, Gijbels et al4 and Akarslan et al10 reported that application of the sharpen filter had no significant effect on CCD-based panoramic images. Whether any significance exists for the visualization of anatomical structures on sharpened panoramic images obtained with SPP-based systems has not been reported. In the only study comparing the effect of various digital filters for SPP-based panoramic images on the visibility of various anatomical structures, the authors used specific enhancement algorithms that aimed to decrease high-frequency noise or increase contrast.9 As the authors did not provide any information regarding the nature or universal name of the enhancement functions, it is difficult to interpret their results. Owing to the differences, either in the sensor or in filter type, the present results cannot be directly compared with the above-mentioned studies. Nevertheless, it was demonstrated that sharpened images were advantageous for the enhancement of anatomical structures on chest radiographs obtained with an SPP-based computed radiography (CR) system.29
The current results indicate that sigmoidal and exponential transformation of grey values on SPP-based digital panoramic images showed similar performance for the visibility of all anatomical structures as well as overall image quality. Changing contrast by means of non-linear LUT adjustments resulted in the best scores following sharpen filter for the perception of low-contrast details and overall quality. It is not possible to compare this result as there have been no studies published using the above mentioned filters with digital panoramic systems. However, it was proved that the application of non-linear LUTs resulted in a significant improvement in the contrast enhancement of chest and extremity radiographs.18 Nonetheless, modifications of the overall contrast and/or brightness scale by means of LUT adjustments did not enhance the perception of high-contrast structures and DEJ. This result could be expected for high-contrast structures as overall change in contrast may not have a prominent effect on the perception of structures that can be easily visualized (large amplitudes). On the other hand, DEJ (a high spatial frequency structure) did not benefit from LUT adjustments, probably because this operation is a global process. In a global process, all pixels in the image have the same operation applied equally across the image such that each pixel value in the image is altered without any influence on the neighbouring pixel values. Accordingly, no improvement in visual perception of local area detail could be achieved.19 Structures in the high spatial frequency range on digital images describe small image details, such as trabeculae in the skeleton. High spatial frequencies also contribute to the sharpness of object contours, such as the edge of a fracture line.16 Therefore, it has been advocated that to improve the perception of high spatial frequencies their contours should be sharpened.16 Accordingly, the sharpening filter gave, subjectively, the best results for the depiction of DEJ. In addition, the thin and indiscernible border between enamel and dentine received the second best scores with the use of a negative filter. Inversion of the image depicted the indistinct borderline clearly because the human eye is more sensitive to slight brightness changes in the dark regions of an image than in the light regions.26
Although DEJ received the second best scores for negative filtered images, the lowest ratings were obtained with a negative filter for the evaluation of low-contrast and high-contrast structures, as well as overall quality. This finding confirms that the individual evaluation of DEJ in the present study is acceptable. The perception in negative radiographs might be underestimated owing to the fact that the observers were used to the original view of a particular anatomical structure on black and white radiographs or images. This result was confirmed by previous studies.30,31
The present study was performed on patients in order to interpolate the results to clinical settings and to test the effect of filters on clinical panoramic images, as image quality is greatly affected by anatomical variations.
In conclusion, it was demonstrated that the overall image quality of SPP-based digital panoramic images is equal to that of conventional panoramic films. High-contrast anatomical structures and DEJ are visualized equally well with unfiltered SPP-based and film images; however, conventional panoramic films are still best for the visualization of low-contrast structures. Among the enhancement filters used, sharpening provided subjectively superior images for the visualization of both high- and low-contrast structures, as well as DEJ. It also provided the best overall image quality and, therefore, may be primarily recommended for enhancing SPP-based panoramic images to improve visual perception. However, it should always be kept in mind that the filtering of a digital image introduces noise to the image. Previous studies reported that enhancement using image filters may not necessarily lead to better image interpretation.4,32 Panoramic images include many shadows and soft-tissue contours and, therefore, inappropriately chosen enhancement factors and algorithms may lead to relative enhancement or suppression of the images of these soft tissues, thereby resulting in the misinterpretation of the processed images. However, at present, no studies with panoramic images have been published to test this interaction, and therefore, further studies are needed to test this assumption.
References
- 1.Mastoris M, Li G, Welander U, McDavid WD. Determination of the resolution of a digital system for panoramic radiography based on CCD technology. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2004;97:408–414 [DOI] [PubMed] [Google Scholar]
- 2.Gijbels F, Sanderink G, Bou Serhal C, Pauwels H, Jacobs R. Organ doses and subjective image quality of indirect digital panoramic radiography. Dentomaxillofac Radiol 2001;30:308–313 [DOI] [PubMed] [Google Scholar]
- 3.Makris N, Tsiklakis K, Alexiou KE, Vierrou AM, Stefaniotis T. The subjective image quality of conventional and digital panoramic radiography among 6 to 10 year old children. J Clin Pediatr Dent 2006;31:109–112 [DOI] [PubMed] [Google Scholar]
- 4.Gijbels F, De Meyer AM, Bou Serhal C, Van denBossche C, Declerck J, Persoons M, et al. The subjective image quality of direct digital and conventional panoramic radiography. Clin Oral Investig 2000;4:162–167 [DOI] [PubMed] [Google Scholar]
- 5.Kaeppler G, Dietz K, Reinert S. The effect of dose reduction on the detection of anatomical structures on panoramic radiographs. Dentomaxillofac Radiol 2006;35:271–277 [DOI] [PubMed] [Google Scholar]
- 6.Molander B, Gröndahl H-G , Ekestubbe A. Quality of film-based and digital panoramic radiography. Dentomaxillofac Radiol 2004;33:32–36 [DOI] [PubMed] [Google Scholar]
- 7.Benediktsdottir IS, Hintze H, Petersen JK, Wenzel A. Image quality of two solid-state and three photostimulable phosphor plate digital panoramic systems, and treatment planning of mandibular third molar removal. Dentomaxillofac Radiol 2003;32:39–44 [DOI] [PubMed] [Google Scholar]
- 8.Prokop M, Neitzel U, Schaefer-Prokop C. Principles of image processing in digital chest radiography. J Thoracic Imaging 2003;18:148–164 [DOI] [PubMed] [Google Scholar]
- 9.Yalçınkaya S, Künzel A, Willers R, Thoms M, Becker J. Subjective image quality of filtered radiographs acquired by the Dürr Vistascan system compared with conventional radipgraphs. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006;101:643–651 [DOI] [PubMed] [Google Scholar]
- 10.Akarslan ZZ, Akdevelioğlu M, Güngör K, Erten H. A comparison of the diagnostic accuracy of bitewing, periapical, unfiltered and filtered digital panoramic images for approximal caries detection in posterior teeth. Dentomaxillofac Radiol 2008;37:458–462 [DOI] [PubMed] [Google Scholar]
- 11.Higashida Y, Moribe N, Morita K, Katsuda N, Hatemura M, Takada T, et al. Detection of subtle microcalcifications: comparison of computed radiography and screen-film mammography. Radiology 1992;183:483–486 [DOI] [PubMed] [Google Scholar]
- 12.MacMahon H, Sanada S, Doi K, Giger M, Xu XW, Yin FF, et al. Direct comparison of conventional and computed radiography with a dual-image recording technique. Radiographics 1991;11:259–268 [DOI] [PubMed] [Google Scholar]
- 13.Chotas HG, Dobbins JT, 3rd, Floyd CE, Jr, Ravin CE. Single-exposure conventional and computed radiography image acquisition. Invest Radiol 1991;26:438–445 [DOI] [PubMed] [Google Scholar]
- 14.Sanada S, Doi K, Xu XW, Yin FF, Giger ML, MacMahon H. Comparison of imaging properties of a computed radiography system and screen-film systems. Med Phys 1991;18:414–420 [DOI] [PubMed] [Google Scholar]
- 15.Wenzel A, Hintze H, Mikkelsen L, Mouyen F. Radiographic detection of occlusal caries in noncavitated teeth. Oral Surg Oral Med Oral Pathol 1991;72:621–626 [DOI] [PubMed] [Google Scholar]
- 16.Prokop M, Schafer-Prokop CM. Digital image processing. Eur Radiol 1997;7:73–82 [PubMed] [Google Scholar]
- 17.Digora forWindows2.5 R1, User's manual, Document number 8201017 ver1 (0506),Soredex,Tuusula, Finland,46–48 [Google Scholar]
- 18.Bonciu C, Razaee MR, Edwards W. Enhanced visualization methods for computed radiography images. J Digit Imaging 2006;19:187–196 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Davidson RA. Radiographic contrast-enhancement masks in digital radiography. Current post-processing methods in digital radiography (chapter 5), Thesis,University of Sydney, Australia,72–77,2006. Available at http://ses.library.usyd.edu.au/bitstream/2123/1932/6/06Chapter5a.pdf. Accessed on 20 April 2009 [Google Scholar]
- 20.Sluder G, Wolf DE. Digital microscopy (3rd edn), Methods in cell biology 81 Cardullo RA, Hincliffe EH. Digital manipulation of bright field and fluorescence images: noise reduction, contrast enhancement and feature extraction. Elsevier; Netherlands: 2007:297–303 [DOI] [PubMed] [Google Scholar]
- 21.Powlis WD, Brikman I. Portal radiographs: Digital enhancement of contrast. Radiology 1988;169:839–841 [DOI] [PubMed] [Google Scholar]
- 22.Haring JI, Jensen L. Normal anatomy-Intraoral films. Dental radiology principles and techniques (2nd edn). Philadelphia, W.B.Saunders Company,2000: 433–434 [Google Scholar]
- 23.Whaites E. The radiographic image. Essentials of dental radiography and radiology (3rd edn). London: Churchill Livingstone, 2002:11 [Google Scholar]
- 24.Workman A, Brettle DS. Physical performance measures of radiographic imaging systems: review. Dentomaxillofac Radiol 1997;26:139–146 [DOI] [PubMed] [Google Scholar]
- 25.Langland OE, Langlais RP, Preece J. Panoramic and special imaging techniques. Principles of dental imaging (2nd edn). Philadelphia: Lippincott Williams & Wilkins,2002:288–289 [Google Scholar]
- 26.Angelopoulos C, Bedard A, Katz JO, Karamanis S, Parissis N. Digital panoramic radiography: An overview. Semin Orthod 2004;10:194–203 [Google Scholar]
- 27.Analoui M. Radiographic image enhancement. Part I: spatial domain techniques. Dentomaxillofac Radiol 2001;30:1–9 [DOI] [PubMed] [Google Scholar]
- 28.Wenzel A, Hintze H. Perception of image quality in direct digital radiography after application of various image treatment filters for detectability of dental disease. Dentomaxillofac Radiol 1993;22:131–134 [DOI] [PubMed] [Google Scholar]
- 29.Prokop M, Schafer-Prokop CM. Storage phosphor radiography. Eur Radiol 1997;7:58–65 [PubMed] [Google Scholar]
- 30.Haak R, Wicht MJ. Grey-scale reversed radiographic display in the detection of approximal caries. J Dent 2005;33:65–71 [DOI] [PubMed] [Google Scholar]
- 31.Eickholz P, Riess T, Lenhard M, Hassfeld S, Staehle HJ. Digital radiography of interproximal bone loss; validity of different filters. J Clin Periodontol 1999;26:294–300 [DOI] [PubMed] [Google Scholar]
- 32.Ramesh A, Tyndall DA, Ludlow JB. Evaluation of a new digital panoramic system: a comparison with film. Dentomaxillofac Radiol 2001;30:98–100 [DOI] [PubMed] [Google Scholar]