

Abstract
Objectives
The aim of this study was to compare the diagnostic quality of a new wireless handheld unit (ADX4000; Dexcowin Co. Ltd, Korea) on conventional bitewings and its LCD screen for the detection of approximal caries in primary teeth.
Methods
In total, 108 approximal surfaces of primary teeth were examined in vitro by 3 observers. Conventional films were viewed under subdued lighting conditions on a conventional view box. Digital 3.5 inch images were displayed on the built-in monitor of the ADX4000 and digital 17 inch images were viewed on a 17 inch monitor. The true caries diagnosis was based on histological assessment of the approximal surfaces after sectioning the primary teeth. Receiver operating characteristic (ROC) curve (Az) analysis was used to assess the diagnostic quality of imaging modalities.
Results
The areas under the ROC curves ranged from 0.786 (digital 17 inch) to 0.813 (digital 3.5 inch). No statistically significant differences were found between the three modalities for detecting approximal caries.
Conclusions
It was concluded that the diagnostic quality of conventional film and digital images, which were exposed and viewed by a new wireless handheld unit, was comparable.
Keywords: approximal caries, bitewing radiographs, handheld unit, receiver operating characteristic curve, primary teeth
Introduction
Since the introduction of the first direct digital system in 1987, a variety of these systems have become available in dentistry in recent years. Digital radiography is now possible with either a charge-coupled device (CCD) or phosphor imaging plates. With the rapid technological progression in dentistry, digital radiographic machines have become smaller and portable. As a result of these properties, this system has become especially advantageous in paediatric dentistry. Using these portable digital radiographic machines children can be diagnosed radiographically and clinically in their dental units, and these machines can also be used while children are treated under general anaesthesia or sedation. The portable units are also suitable for use in nursing homes, humanitarian missions and with disabled patients.
The ADX4000 (Dexcowin Co. Ltd, Korea) is a three in one machine combining an X-ray source, digital radiography sensor and computer processor in a portable and wireless handheld unit. It weighs 2.2 kg and uses a charging battery-pack of the loading/unloading type. The ADX4000 operates at a fixed tube potential of 60 kV, at 1.0 mA and with a 0.8 mm focal spot with a 10 cm source-to-skin distance. The built-in monitor of the ADX4000 is a TFT LCD 3.5 inch monitor with 320 × 240 resolution. It has an image storage facility of 300 images.
The aim of this study was to compare the diagnostic quality of a new wireless handheld unit (ADX4000) on conventional bitewings and its LCD screen for the detection of approximal caries in primary teeth.
Materials and methods
54 human first and second primary molar teeth extracted because of physiological root resorption or for orthodontic reasons were used in this study. The selection of teeth was based on visual inspection with a 1.5× magnifying lens. Thus, the observer could select equal proportions of carious and non-carious approximal surfaces. The approximal surfaces of the teeth were visually without cavitations. Teeth with restorations and large approximal cavitations or with facial or lingual caries were excluded. The teeth were positioned with approximal contacts to simulate clinical conditions. The roots of the teeth were then immersed in die stone to a depth corresponding to a healthy bone level.
The conventional and digital images of the teeth were acquired by using bitewing projection geometry. The radiographic films (Ektaspeed plus; Kodak, Rochester, NY) and the CCD sensor (CCD38-20; Marconi Applied Technologies Ltd, Chelmsford, UK) were held by Kwik-bite® and Kwik-bite® Senso (Kwik-bite; Hawe Neos Dental, Bioggio, Switzerland) film holders. An ADX4000 portable radiographic machine was used at 60 kVp to make the exposures (Figure 1). The films were exposed for 0.32 s, whereas the CCD sensor was exposed for 0.06 s. The films were developed in an automatic film processor with fresh solution (Velopex, Extra-X; Medivance Instruments Ltd, London, UK). To simulate soft tissue, 14 mm dental wax was placed in front of the teeth.1
Figure 1.

A convenient three-in-one machine, ADX4000 (Dexcowin Co. Ltd, Korea)
Three faculty members, each with approximately 10 years of clinical experience, served as observers. The observers were asked to score the approximal caries according to a five-point confidence scale: 1, definitely present; 2, probably present; 3, unsure; 4, probably not present; and 5, definitely not present. Observers viewed three types of images in four different viewing sessions. Images were randomized for both radiographic methods. At least 1 week was allowed to elapse between consecutive sessions. Before the observation sessions, written and verbal instructions were given to the observers.
Conventional films were viewed under subdued lighting conditions on a conventional view box. Digital 3.5 inch images were displayed on the built-in monitor of the ADX4000 (TFT LCD 3.5 inch monitor with 320 × 240 resolution), whereas digital 17 inch images were viewed on a 17 inch monitor with 1024 × 768 resolution. No adjustment of contrast or brightness was performed by the observers.
Following acquisition of the radiographs, teeth were sectioned mesiodistally in approximately 400-μm-thick sections (Mecatome T201, Presi, France). Sections were examined under a 16× magnifying microscope by 2 observers. Tooth sections were evaluated for the absence of approximal carious lesions and the penetration depth of a caries lesion. 108 approximal surfaces were selected for the study: 42 surfaces were caries free; 25 had carious lesions limited to the outer half of the enamel; 28 had carious lesions into the inner half of the enamel; and 13 had carious lesions into the inner half of the dentine.
Receiver operating characteristic (ROC) curve (Az) analysis was used to assess the diagnostic accuracy of the three imaging modalities. MedCalc statistical software (version 9.4.2.0) was used for ROC analysis. The Az values were calculated for each observer for each diagnostic method. ANOVA was performed to compare variances. The level of statistical significance was set as α _ 0.05. The Pearson correlation coefficient was used to measure intrarater reliability, and Kendall's coefficient of concordance was used to measure interrater reliability.
Results
The Pearson correlation coefficient was 0.53 for intrarater reliability and the coefficient of concordance was 0.34 for interrater reliability.
There was no statistically significant difference in the performance of the dental films and the digital imaging systems exposed and viewed by the ADX4000 when Az values were calculated from all three observers in the 95% confidence interval. Table 1 shows individual Az scores for each observer and each modality. Figure 2 shows the ROC curves for each radiographic method. No statistically significant differences were found between the three modalities for detecting approximal caries (P > 0.05).
Table 1. Receiver operating characteristic (ROC) curve areas for approximal caries detection for observers 1–3 with conventional bitewings and digital bitewings viewed on 17 and 3.5 inch monitors.
| Observer | Area under the ROC curve |
||
| Conventional | Digital 3.5 inch | Digital 17 inch | |
| 1 | 0.820 | 0.827 | 0.796 |
| 2 | 0.803 | 0.802 | 0.774 |
| 3 | 0.813 | 0.810 | 0.788 |
| Mean | 0.812 | 0.813 | 0.786 |
Figure 2.
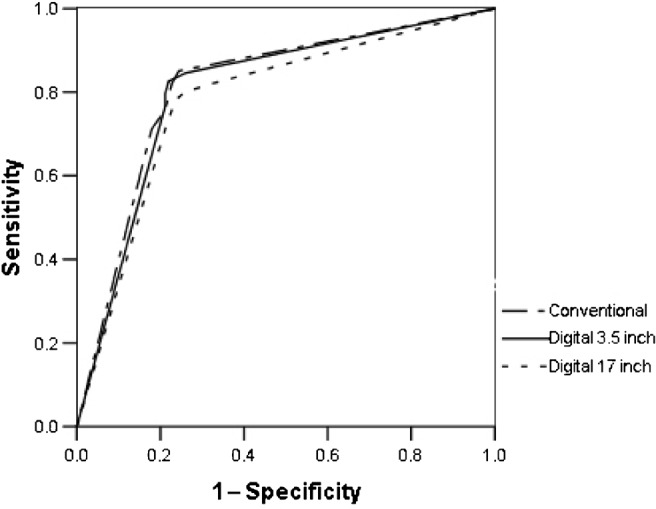
Receiver operating characteristic curves for three observers' averaged assessment of approximal caries with three modalities
Discussion
In the present study, a portable radiographic machine (ADX4000) was used at 60 kVp to make the exposures, and this system combines an X-ray source, digital radiography sensor and computer processor in one completely portable and wireless handheld unit. The built-in monitor of the ADX4000 is a TFT LCD 3.5 inch monitor with 320 × 240 resolution. According to Li et al,2 the mean values of the desired and minimum acceptable spatial resolution of the sensor are 17 lp mm−1 and 10 lp mm−1, respectively. Syriopoulos et al3 reported that low resolution (e.g. 4 lp mm−1) made the diagnosis of approximal caries more difficult. In the current study, the sensor of the handheld unit was 10 lp mm−1.
There was no statistical difference between the bitewing systems for the detection of approximal caries exposed and viewed by a wireless handheld unit. Although the difference was not significant, it must be taken into consideration that the results of statistical comparisons might be biased because of the small number of observers.4 When comparing the intra- and interrater reliability of this present study with the other studies, Castro et al5 reported higher values than the present findings. Naitoh et al6 also found higher interrater reliability values than determined in the current study. This may be due to differences in the gold standard criteria between authors. Naitoh et al6 used radiological images, which are reported to yield a better agreement than the histological validation utilized by Hintze and Wenzel.7
Syriopoulos et al3 reported that the performance of the observers affected the performance of the imaging modalities. They suggested that the relative inexperience of general practitioners in digital imaging could have influenced their performance. In their study, although the general practitioners and radiologists overestimated the number of sound surfaces to a similar degree, radiologists assessed the severity of the lesion more accurately. In the current study, all observers were specialists, each with approximately 10 years of experience.
The condition under which a radiograph is examined affects caries detection.8 In this study, conventional films were viewed under subdued lighting conditions on a conventional view box. To standardize the images, film holders were used (Kwik-bite® and Kwik-bite® Senso). The use of a film holder is very important not only to minimize dose but also to avoid changes in exposure geometry leading to misleading changes in the subsequent images of an individual lesion.9
The small size of the monitor might have affected the observers' decision to evaluate carious lesions. Moystad et al10 found that detecting artificial bone lesions on digital images was similar to that with film images when using 5 inch, non-manipulated digital images. Interestingly, the current study's results showed that there was no significant difference between the 3.5 inch monitor with 320 × 240 resolution and the 17 inch monitor with 1024 × 768 resolution for detecting approximal caries. Although Hellén-Halme11 suggested that the ability to diagnose carious lesions is significantly better with a monitor with well-adjusted brightness and contrast values, observers were not allowed to manipulate the digital images. The results of such manipulation have been variable. Ohki et al12 showed a significant decrease in diagnostic accuracy when observers were allowed to manipulate the images.
ROC analysis is well established as a method of comparing the diagnostic accuracies of imaging systems. The ROC curve areas calculated in the present study, for assessment of diagnostic accuracy of approximal caries in conventional bitewings, demonstrated no significant differences in Az values compared with digital bitewings. ROC analyses have usually failed to show statistically significant differences, with respect to caries diagnosis, between film and digital imaging systems.4, 5, 13–15 On the other hand, Moystad et al10 evaluated the storage phosphor system for detecting approximal caries and they reported that enhanced storage phosphor images had significantly higher Az values than dental radiographic film. Price and Ergül16 also showed significant differences between the ROC areas for film and a digital imaging system with respect to natural caries and artificial cavities. Dagenais and Clark17 found that holes drilled in proximal surfaces of teeth to simulate caries were better detected on film than on digital images. White and Yoon15 also suggested that the sharp edges associated with the simulated lesions were better detected on higher resolution film than on lower resolution sensors.
In conclusion, it was found that the diagnostic quality of conventional film and digital images, which were exposed and viewed by a new wireless handheld unit, was comparable. The ADX4000 has become especially advantageous in paediatric dentistry and it also has potential for use in nursing homes, humanitarian missions and forensic dentistry and also with disabled patients.
Acknowledgments
This study was supported by the University of Gazi, Committee of Scientific Research Projects (no. 03/2006-18).
References
- 1.Haak R, Wicht MJ, Noack MJ. Conventional, digital and contrast-enhanced bitewing radiographs in the decision to restore approximal carious lesions. Caries Res 2001;35:193–199 [DOI] [PubMed] [Google Scholar]
- 2.Li G, van derStelt PF, Verheij JG, Speller R, Galbiati A, Psomadellis F, et al. End-user survey for digital sensor characteristics: a pilot questionnaire study. Dentomaxillofac Radiol 2006;35:147–151 [DOI] [PubMed] [Google Scholar]
- 3.Syriopoulos K, Sanderink GC, Velders XL, van derStelt PF. Radiographic detection of approximal caries: a comparison of dental films and digital imaging systems. Dentomaxillofac Radiol 2000;29:312–318 [DOI] [PubMed] [Google Scholar]
- 4.Hintze H, Frydenberg M, Wenzel A. Influence of number of surfaces and observers on statistical power in a multiobserver ROC radiographic caries detection study. Caries Res 2003;37:200–205 [DOI] [PubMed] [Google Scholar]
- 5.Castro VM, Katz JO, Hardman PK, Glaros AG, Spencer P. In vitro comparison of conventional film and direct digital imaging in the detection of approximal caries. Dentomaxillofac Radiol 2007;36:138–142 [DOI] [PubMed] [Google Scholar]
- 6.Naitoh M, Yuasa H, Toyama M, Shiojima M, Nakamura M, Ushida M, et al. Observer agreement in the detection of proximal caries with direct digital intraoral radiography. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998;85:107–112 [DOI] [PubMed] [Google Scholar]
- 7.Hintze H, Wenzel A. Influence of the validation method on diagnostic accuracy for caries. A comparison of six digital and two conventional radiographic systems. Dentomaxillofac Radiol 2002;31:44–49 [DOI] [PubMed] [Google Scholar]
- 8.Chadwick BL, Dummer PH. Factors affecting the diagnostic quality of bitewing radiographs: a review. Br Dent J 1998;184:80–84 [DOI] [PubMed] [Google Scholar]
- 9.Pitts NB. The use of film holding, beam collimating and aiming devices in bitewing radiography. A suggested design for routine and research use. Dentomaxillofac Radiol 1983;12:77–82 [DOI] [PubMed] [Google Scholar]
- 10.Moystad A, Svanaes DB, Larheim TA, Grondahl HG. The effect of cathode ray tube display format on observer performance in dental digitized radiography: comparison with plain films. Dentomaxillofac Radiol 1994;23:206–210 [DOI] [PubMed] [Google Scholar]
- 11.Hellén-Halme K. Quality aspects of digital radiography in general dental practice. Swed Dent J Suppl 2007:9–60 [PubMed] [Google Scholar]
- 12.Ohki M, Okano T, Nakamura T. Factors determining the diagnostic accuracy of digitized conventional intraoral radiographs. Dentomaxillofac Radiol 1994;23:77–82 [DOI] [PubMed] [Google Scholar]
- 13.Abreu M, Jr, Mol A, Ludlow JB. Performance of RVGui sensor and Kodak Ektaspeed Plus film for proximal caries detection. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2001;91:381–385 [DOI] [PubMed] [Google Scholar]
- 14.Wenzel A, Hintze H, Mikkelsen L, Mouyen F. Radiographic detection of occlusal caries in noncavitated teeth. A comparison of conventional film radiographs, digitized film radiographs, and RadioVisioGraphy. Oral Surg Oral Med Oral Pathol 1991;72:621–626 [DOI] [PubMed] [Google Scholar]
- 15.White SC, Yoon DC. Comparative performance of digital and conventional images for detecting proximal surface caries. Dentomaxillofac Radiol 1997;26:32–38 [DOI] [PubMed] [Google Scholar]
- 16.Price C, Ergül N. A comparison of a film-based and a direct digital dental radiographic system using a proximal caries model. Dentomaxillofac Radiol 1997;26:45–52 [DOI] [PubMed] [Google Scholar]
- 17.Dagenais ME, Clark BG. Receiver operating characteristics of RadioVisioGraphy. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1995;79:238–245 [DOI] [PubMed] [Google Scholar]