

Abstract
Objective
The aim was to evaluate the possibility of radiographic prediction of the prognosis of simple bone cysts (SBCs) of the jaws.
Methods
The relationship between the radiographic findings and treatment outcome (healing or recurrence) was investigated in 31 cases treated in the authors' hospital and 108 published cases.
Results
In 17 of our 31 cases, the lesions had radiographic findings of a preserved lamina dura adjacent to the lesion, with a smooth margin, and no or smooth bone expansion, and all of them healed after surgery. In the other 14 cases, there was resorption of the lamina dura, a scalloped margin, nodular bone expansion, root resorption, a sclerotic mass or multiple cavities, and nine cases of recurrence. Although there was incomplete information in the published case studies, similar results were noted.
Conclusions
It was concluded that there was a relationship between the radiographic features of the lesions and prognosis. Radiographic examination should be used not only for discovering and diagnosing the lesions, but also for predicting possible prognosis.
Keywords: bone cyst, diagnosis, radiology, treatment outcome
Introduction
It seems to be a common belief that simple bone cysts (SBCs) of the jaws are cured primarily by simple bone curettage;1–3 however, previous studies have reported various treatments and prognoses. In some cases, radiographic follow-up without surgery demonstrated spontaneous healing.4, 5 Sometimes the lesion resolved after aspiration of the cavity or surgical exploration without curettage.6, 7 Some cases involved extraction of the involved tooth, partial resection of the jawbone, or repeated operations of more than three times for recurrent lesions.8–11 Recurrence occurred even in cases with initial bone formation after surgery.12–14 Because of these variations in prognosis, it is reasonable to modify the follow-up plan in accordance with the possible prognosis of the lesions. However, there is not a common means of forecasting the prognosis of a lesion, although several papers have pointed out the possible relation between some clinical findings and recurrence of the lesions.10, 11
This study was designed to examine the radiographic findings that are useful for predicting the prognosis of SBCs. Radiographic examination was considered to be the most suitable, for a review of its ability to predict prognosis, because it is performed in all cases and the results are frequently reported in the literature.
Materials and methods
This study included 31 patients with SBC treated in the authors' hospital and 108 cases that had been published in English language literature, for which the treatment outcome (healing or recurrence) was stated. All of our cases were diagnosed by the finding of an intrabone cavity without epithelial lining. Soft tissue mass, if present, was histologically examined to exclude the possibility of any other entities. Published cases were initially investigated by a literature survey, which was conducted using PubMed, a database created by the National Center for Biotechnology Information (NCBI: http://www.ncbi.nlm.nih.gov/). The term “simple bone cyst” and several synonyms for SBC (traumatic bone cyst, haemorrhagic/hemorrhagic bone cyst, extravasation cyst, solitary bone cyst, idiopathic bone cyst/cavity and progressive bone cavity) were used as search terms. Including three studies15–17 cited in the literature, obtained through PubMed, a total of 108 cases of SBC in 63 reports, which were followed up until healing or recurrence were identified.
According to patient records and radiographs in our cases and the authors' descriptions in the published cases, age and sex, radiographic findings, histological findings, treatment procedures and prognosis were investigated. For radiographic assessment, we defined 10 findings and 2 oral radiologists, including the first author (YS), examined intraoral and panoramic radiographs of the cases. If the evaluations differed between the two observers, the final determination was reached by consensus after discussion. The definitions of the findings are presented in Table 1 and Figures 1–5. In the survey for treatment procedure, we did not differentiate between curettage of the bone wall and exploration of the cavity because thorough curettage of the bone wall was considered difficult in patients with an exposed tooth root and neurovascular band in the cavities. In these cases, part of the soft tissue wall may remain after curettage and the effect of the procedure is similar to that of exploration. Treatment outcome was assessed as healing or recurrence and was decided radiographically. The criterion for healing was resolution of the radiolucent lesion with newly formed bone trabeculae. The criterion for recurrence was enlargement or reformation of the radiolucency after surgery. In the review of published cases, it was assumed that descriptions such as “complete healing”, “complete bone regeneration” and “normal bone trabeculation” were indicative of healing. Descriptions such as “adequate bone formation” and “good bone formation” were not assumed to indicate healing because recurrence can occur after considerable bone regeneration or formation.13 Patients who underwent a second operation when there was little or no bone regeneration after the primary operation (persistent cyst18) were included in the group of cases with recurrence.
Table 1. Ten radiographic findings and their definitions.
| Radiographic finding | Definition |
| Intact lamina dura | Lamina dura adjacent to the lesion is fairly well preserved (Figure 1) |
| Absent lamina dura | Lamina dura is resorbed by the lesion mostly or completely (Figure 2) |
| Root resorption | The lesion has resorbed the tooth root (Figure 3) |
| Smooth margin | The boundary of the cavity is smooth and circular, and the lesion is round or ovoid, except the area around the tooth root (Figure 1) |
| Scalloped margin | The margin of the lesion is scalloped or a septum-like radiopaque line is observed in the cavity (Figures 3 and 4) |
| No expansion | Bone expansion is not confirmed radiographically |
| Smooth expansion | Slight to moderate bone expansion with a smooth surface smoothly transitioning to the surrounding bone surface (Figure 1) |
| Nodular expansion | Bone expansion is protuberant and/or has an irregular surface. The boundary between the expanded and surrounding bone surface may be crooked (Figure 4) |
| Radiopaque mass | A radiopaque mass is observed in the cavity (Figures 4 and 5) |
| Multiple cavities | Multiple lesions are observed (Figure 4) |
Figure 1.

(a) Simple bone cyst cavity with a smooth margin. (b) Radiographic finding of an intact lamina dura. The lamina dura adjacent to the lesion is fairly well preserved. (c) Occlusal radiograph revealing smooth bone expansion. (d) 4 years and 3 months after surgery, healing of the lesion is confirmed by the formation of new bone trabecula
Figure 5.
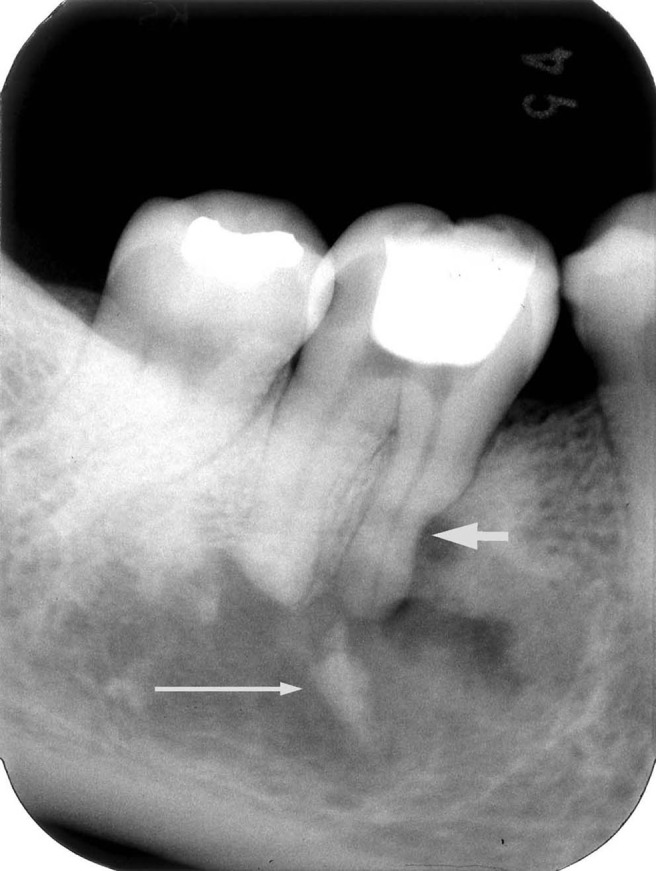
Simple bone cyst with a radiopaque mass in the cavity (long arrow). Root resorption is suspected at the medial root of the first molar (short arrow). The lesion recurred twice after surgery
Figure 2.

Simple bone cyst with an absent lamina dura. Most of the lamina dura has been resorbed
Figure 3.
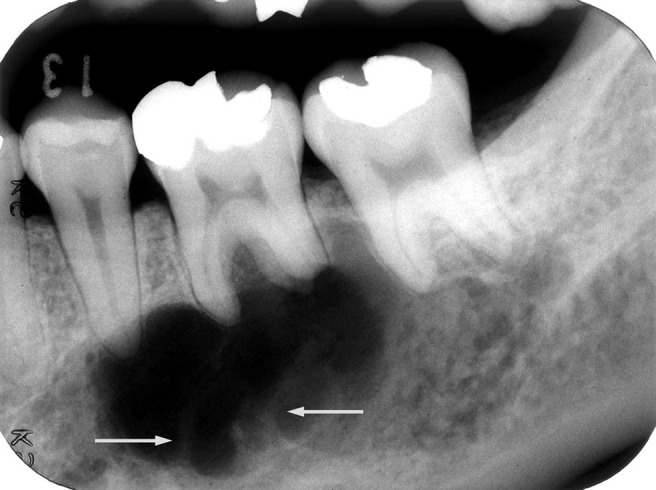
Simple bone cyst with root resorption of the first molar tooth. Septum-like radiopaque lines are also seen (arrows). This lesion recurred after surgery
Figure 4.

(a) Simple bone cyst accompanied by florid cemento-osseous dysplasia (FCOD). Cavities with a scalloped margin are observed in the right molar and anterior teeth regions. No sclerotic mass is apparent, but one was confirmed in periapical radiographs of the incisor region. (b) Characteristic finding of nodular expansion. Protuberant bone expansion with an irregular surface is noted. (c) Seven months after surgery, bone formation is confirmed in the cavity. (d) 4 years and 10 months after surgery; in addition to recurrence of the lesion, formation of a sclerotic mass of FCOD is confirmed (arrow)
Finally, to identify radiographic findings useful for forecasting the prognosis, the numbers of healed and recurrent cases were investigated in each group of cases for each radiographic finding. Furthermore, to assess the possibility of a radiographic classification of the lesions and its relation to prognosis, the cases were divided based on the radiographic findings and the prognoses were compared.
Results
The total number of healing cases and recurrent cases were 102 and 37, respectively (Table 2). The recurrence rate was 26.6%. Patients with recurrence were older than those with healing and more women than men had recurrence. Histological examination was carried out in our 22 patients, including all 9 patients with recurrence, and in 82 published cases, and this confirmed fibroconnective tissue, granulation tissue, blood clot and/or bone tip. In some cases, giant cells and/or dysplastic bone formation were found in the connective tissue. No specific relationship between these histological findings and prognosis was found, but a high rate of recurrence was confirmed in cases with concomitant osseous dysplasia (OD); 9 of 10 cases with OD recurred. Surgical procedures and treatment results are shown in Table 3. The results indicate the possibility that fenestration and packing the cavity with materials are more curative than curettage or exploration of the cavity, although there was no statistically significant difference. The relationship between radiographic features and prognosis is described below in detail.
Table 2. Patient age and sex distribution of healed and recurrent cases.
| Treatment outcome (number of cases) | Number of males/females | Average age (range) (years) | ||
| Our 31 cases | Healing (22) | 10/12 | 16.5 (10–38) | P _ 0.0032∗∗ |
| Recurrence (9) | 1/8 | 38.1 (21–76) | ||
| Published cases (108 cases) | Healing (80)∗ | 29/27 | 19.0 (10–51) | P _ 0.104∗∗ |
| Recurrence (28)† | 7/12 | 25.7 (7–51) | ||
| Total | Healing (102)∗ | 39/39 | 18.3 (10–51) | P _ 0.0018∗∗ |
| Recurrence (37)† | 8/20 | 29.6 (7–76) | ||
| Total (139) | 47/59 | 21.1 |
∗,†Sex or age was not stated in 24 and 9 cases, respectively.
∗∗Independent t-test.
Table 3. Surgical procedures and the number of healing and recurrent cases.
| Surgical procedure | Case study |
Literature review |
Total recurrence rate | ||
| Healing |
Recurrence |
Healing |
Recurrence |
||
| (n _ 22) | (n _ 9) | (n _ 80) | (n _ 28) | (%) | |
| Curettage of the bone wall/exploration of the cavity | 17 | 7 | 58 | 20 | 29.3 |
| Fenestration | 3 | 2 | 8 | 0 | 15.4 |
| Packing the cavity with material∗ | 0 | 0 | 8 | 0 | 0 |
| Aspiration | 0 | 0 | 1 | 0 | 0 |
| Osteotomy of the condyle | 0 | 0 | 1 | 0 | 0 |
| Unknown/not recorded | 2 | 0 | 4 | 8 | – |
∗Gelfoam was applied in five cases. Bone tip, gelatine sponge or gauze pack was applied in one case each.
Relationship between the radiographic findings and prognosis
In our case study, the ten defined findings could be assessed in all but two cases. In one case, the lesion did not contact the lamina dura; in the other case, bone expansion was not assessed because of the absence of an occlusal radiograph. In the published cases, most described only a few findings, if any. The findings concerning the lamina dura, cavity margin and bone expansion were described in only 22, 16 and 31 of the 108 published cases, respectively. Overall, the results were similar between the two studies (Table 4). Most of the lesions with a radiographic finding of an intact lamina dura or smooth margin healed after surgery, whereas more than 60% recurred in cases with the finding of an absent lamina dura, root resorption, scalloped margin, radiopaque mass or multiple cavities.
Table 4. The number of cases with each radiographic finding and the treatment outcome.
| Radiographic finding | Our cases |
Published cases |
Total |
|||||
| Healing (n _ 22) | Recurrence (n _ 9) | Healing (n _ 80) | Recurrence (n _ 28) | Healing | Recurrence | Recurrence rate (%) | ||
| Intact lamina dura | 17 | 0 | 15 | 2 | 32 | 2 | 5.9 | |
| Absent lamina dura | 5 | 8 | 2 | 3 | 7 | 11 | 61.0 | |
| Root resorption | 1 | 4 | 0 | 0 | 1 | 4 | 80.0 | |
| Smooth margin | 20 | 1 | 0 | 0 | 20 | 1 | 4.8 | |
| Scalloped margin | 2 | 8 | 7 | 9 | 9 | 17 | 65.4 | |
| No expansion | 9 | 2 | 10 | 1 | 19 | 3 | 13.6 | |
| Smooth expansion | 12 | 3 | 14 | 6 | 26 | 13 | 33.3 | |
| Nodular expansion | 0 | 4 | ||||||
| Radiopaque mass∗ | 1 | 5 | 2 | 8 | 3 | 13 | 81.3 | |
| Multiple cavities† | 1 | 5 | 4 | 9 | 5 | 14 | 73.7 | |
In the survey of the published cases, most of the cases described only a few findings, if any, and the number of the findings was not 10 but 9 because bone expansion was reported as either absent or present, whereas the authors described it as absent, smooth or nodular in our cases. Therefore, the number of rows in the first 2 columns is 10 and that in the following 5 columns is 9
∗The histology was cemento-osseous dysplasia in eight cases, tooth in three cases, bone in one case and unknown in four cases.
†Osseous dysplasia was associated in seven cases.
Radiographic classification
The cases in the present study were divided into two groups based on the findings of the lamina dura: 17 cases with an intact lamina dura and 13 cases with an absent lamina dura (Table 5). In the cases with an intact lamina dura, the associated findings were only a smooth margin and no or smooth bone expansion, all cases healed. Whereas in 13 cases with an absent lamina dura, a scalloped margin, root resorption, nodular bone expansion, radiopaque mass or multiple cavities were observed, there was recurrence after surgery in 8 cases. No other meaningful classification of the cases was found, other than those of the lamina dura.
Table 5. Radiographic classification of our 30 cases based on the presence of the lamina dura and the distribution of the other radiographic findings in each group.
| Margin |
Root resorption | Expansion |
Radiopaque mass | Multiple cavities | Number of cases with recurrence | ||||
| Smooth | Scalloped | No | Smooth | Nodular | |||||
| Intact lamina dura (17 cases) | 17 | 0 | 0 | 6 | 10 | 0 | 0 | 0 | 0 |
| Absent lamina dura (13 cases) | 4 | 9 | 5 | 5 | 4 | 4 | 6 | 6 | 8 |
In the survey of published cases, evaluation of the radiographic classification of the cases was difficult because of imperfect descriptions concerning the radiographic findings in most of the reports. Only four cases reported all of the findings concerning the lamina dura, cavity margin and bone expansion.
Discussion
The radiographic examination provides much clinical information about SBC lesions, including the presence of associated conditions such as osseous dysplasia and fibrous dysplasia. Shear19 pointed out that the careful interpretation of good radiographs was most valuable in diagnosis. Nevertheless, most authors have used radiographs only to show an outline of the lesion, and no extensive radiographic study has been conducted.
Relationship between the radiographic findings and prognosis
All of our cases with an intact lamina dura healed after treatment, and spontaneous healing was reported in cases with an intact lamina dura.5, 20 Recurrence was confirmed in only 2 of the 17 published cases with an intact lamina dura. Therefore, an intact lamina dura could be used as a sign of probable healing after surgery. However, the lamina dura may be resorbed partially in cases considered to have an intact lamina dura or some lamina dura might remain in cases deemed to have an absent lamina dura. The finding of a lamina dura is useful for predicting the prognosis, but a decision should be avoided in borderline cases. The finding of an absent lamina dura has not been emphasised in SBC studies, but it was not rare and was considered a sign of possible recurrence after surgery (Table 4). A high recurrence rate in cases with a scalloped margin (multilocular appearance) was confirmed in a long-bone SBC study.21 This has not been assessed in jawbone SBCs, although we observed recurrence in 65.4% (17/26) of cases with a scalloped margin versus 4.8% (1/21 cases) of cases with a smooth margin. Therefore, a scalloped margin is a sign of possible recurrence, although this should not be confused with the interdental scalloping associated with an intact lamina dura. The relationship between the presence of bone expansion and the recurrence rate has not been investigated. In this study, the recurrence rate was greater in cases with bone expansion than in those without bone expansion. In addition, the nature of the expansion (smooth or nodular) was important for predicting the prognosis; most of the cases with smooth expansion healed, whereas all four cases with nodular expansion recurred in our case study (Table 4). In 8 of the 16 cases with a radiopaque mass in the cavity, the mass was OD and recurrence occurred in 7. Melrose et al22 confirmed in their follow-up study of SBCs associated with OD that three of nine cases recurred after surgery. SBCs with OD should be recognized as having a high potential for recurrence after treatment. A radiopaque mass other than OD was seen in eight cases, and six of them recurred after surgery. There might be a relationship between these masses and prognosis, but this cannot be discussed at present. In cases with multiple cavities, the reported recurrence rate is high.22, 23 In the present study (reviewed cases plus the authors own) as well, 14 of 19 cases with multiple cavities recurred after surgery. In addition, we noted a high proportion of multiple cavities in SBCs affecting the jawbone: 13.6% (18/132 cases) in this study, and 21.4% (3/14),11 20% (3/15),24 6.2% (10/161)23 and 4.0% (2/51)10 in reported studies. Even after excluding cases with OD, 12 cases (9.4%) had multiple cavities in our study. The jawbone is thought to possess a peculiar nature that generates SBC lesions. It is speculated that this is associated with odontogenic tissue, because SBCs frequently occur in the body of the mandible and are associated with OD.2, 22, 25
Radiographic classification and prognosis
Our study suggested that SBC cases can be classified into two groups radiographically, and the classification might be related to the prognosis (Table 5). Lesions in one group had the findings of only an intact lamina dura, smooth margin and no/smooth bone expansion and will heal after surgery, whereas lesions in the other group can include findings of an absent lamina dura, root resorption, scalloped margin, nodular expansion, radiopaque mass or multiple lesions and may recur.
In conclusion, radiographic assessment is considered useful for forecasting the prognosis of SBC lesions. In cases with the radiographic features of absent lamina dura, scalloped margin, nodular bone expansion, radiopaque mass and/or multiple cavities, the necessity for long-term follow-up and the possibility of repeated surgery should be considered.
References
- 1.Weber AL, Kaneda T, Scrivani SJ, Aziz S. Jaws and temporomandibular joints. In: Som PM, Curtin HD (eds). Head and neck imaging, 4th edn. St. Louis: Mosby, 2003, pp 942–943 [Google Scholar]
- 2.White SC, Pharoah MJ. Oral radiology principles and interpretation, 5th edn. St. Louis: Mosby, 2004, pp 405–409. [Google Scholar]
- 3.Shafer WG, Hine MK, Levy BM. A textbook of oral pathology, 4th edn. Philadelphia: WB Saunders, 1983, pp 541–544. [Google Scholar]
- 4.Damante JH, Da S, Guerra EN, Ferreira Jr O. Spontaneous resolution of simple bone cysts. Dentomaxillofac Radiol 2002;31:182–186 [DOI] [PubMed] [Google Scholar]
- 5.Sapp JP, Stark ML. Self-healing traumatic bone cysts. Oral Surg Oral Med Oral Pathol 1990;69:597–602 [DOI] [PubMed] [Google Scholar]
- 6.Chapman PJ, Romaniuk K. Traumatic bone cyst of the mandible: regression following aspiration. Int J Oral Surg 1985;14:290–294 [DOI] [PubMed] [Google Scholar]
- 7.Howe GL. “Haemorrhagic cysts” of the mandible. II. Br J Oral Surg 1965;3:77–91 [DOI] [PubMed] [Google Scholar]
- 8.Narang R, Jarrett JH. Large traumatic bone cyst of the mandible. J Oral Surg 1980;38:617–618 [PubMed] [Google Scholar]
- 9.Lindsay JS, Martin WR, Green HG. Traumatic bone cyst treated with homogenous bone graft. Report of a case. Oral Surg Oral Med Oral Pathol 1966;21:536–542 [DOI] [PubMed] [Google Scholar]
- 10.Matsumura S, Murakami S, Kakimoto N, Furukawa S, Kishino M, Ishida T, et al. Histopathologic and radiographic findings of the simple bone cyst. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998;85:619–625 [DOI] [PubMed] [Google Scholar]
- 11.MacDonald-Jankowski DS. Traumatic bone cysts in the jaws of a Hong Kong Chinese population. Clin Radiol 1995;50:787–791 [DOI] [PubMed] [Google Scholar]
- 12.Dellinger TM, Holder R, Livingston HM, Hill WJ. Alternative treatments for a traumatic bone cyst: a longitudinal case report. Quintessence Int 1998;29:497–502 [PubMed] [Google Scholar]
- 13.Horner K, Forman GH, Smith NJ. Atypical simple bone cysts of the jaws. I. Recurrent lesions. Clin Radiol 1988;39:53–57 [DOI] [PubMed] [Google Scholar]
- 14.Vijayaraghavan K, Whitlock RI. An unusual case of “haemorrhagic” bone cyst. Br J Oral Surg 1975;13:64–72 [DOI] [PubMed] [Google Scholar]
- 15.Moss M, Levey A. The traumatic bone cyst: report of three cases. J Am Dent Assoc 1966;72:397–402 [Google Scholar]
- 16.Ivy RH, Curtis L. Hemorrhagic or traumatic cysts of mandible. Int J Orthodont 1937;23:640–643 [Google Scholar]
- 17.Blum T. Unusual bone cavities in the mandible: a report of three cases of traumatic bone cysts. J Am Dent Assoc 1932;19:281–301 [Google Scholar]
- 18.Chang CH, Stanton RP, Glutting J. Unicameral bone cysts treated by injection of bone marrow or methylprednisolone. J Bone Joint Surg Br 2002;84:407–412 [DOI] [PubMed] [Google Scholar]
- 19.Shear M. Cysts of the oral regions. Oxford, UK: Butterworth-Heinemann, 1992 [Google Scholar]
- 20.Szerlip L. Traumatic bone cysts. Resolution without surgery. Oral Surg Oral Med Oral Pathol 1966;21:201–204 [DOI] [PubMed] [Google Scholar]
- 21.Campanacci M, Capanna R, Picci P. Unicameral and aneurysmal bone cysts. Clin Orthop Relat Res 1986;204:25–36 [PubMed] [Google Scholar]
- 22.Melrose RJ, Abrams AM, Mills BG. Florid osseous dysplasia. A clinical-pathologic study of thirty-four cases. Oral Surg Oral Med Oral Pathol 1976;41:62–82 [DOI] [PubMed] [Google Scholar]
- 23.Kaugars GE, Cale AE. Traumatic bone cyst. Oral Surg Oral Med Oral Pathol 1987;63:318–324 [DOI] [PubMed] [Google Scholar]
- 24.Saito Y, Hoshina Y, Nagamine T, Nakajima T, Suzuki M, Hayashi T. Simple bone cyst. A clinical and histopathologic study of fifteen cases. Oral Surg Oral Med Oral Pathol 1992;74:487–491 [DOI] [PubMed] [Google Scholar]
- 25.Waldron CA, Giansanti JS, Browand BC. Sclerotic cemental masses of the jaws (so-called chronic sclerosing osteomyelitis, sclerosing osteitis, multiple enostosis, and gigantiform cementoma). Oral Surg Oral Med Oral Pathol 1975;39:590–604 [DOI] [PubMed] [Google Scholar]