

Abstract
Objectives
The aim of this study was to determine the geometric accuracy of cone beam CT (CBCT)-based linear measurements of bone height obtained with the Galileos CBCT (Sirona Dental Systems Inc., Bensheim, Hessen, Germany) in the presence of soft tissues.
Methods
Six embalmed cadaver heads were imaged with the Galileos CBCT unit subsequent to placement of radiopaque fiduciary markers over the buccal and lingual cortical plates. Electronic linear measurements of bone height were obtained using the Sirona software. Physical measurements were obtained with digital calipers at the same location. This distance was compared on all six specimens bilaterally to determine accuracy of the image measurements.
Results
The findings showed no statistically significant difference between the imaging and physical measurements (P > 0.05) as determined by a paired sample t-test. The intraclass correlation was used to measure the intrarater reliability of repeated measures and there was no statistically significant difference between measurements performed at the same location (P > 0.05).
Conclusions
The Galileos CBCT image-based linear measurement between anatomical structures within the mandible in the presence of soft tissues is sufficiently accurate for clinical use.
Keywords: tomography, cone-beam computed; cadaver; head
Introduction
Accuracy of measurements with respect to linear distance is vital for implant surgery or other surgical procedures performed in close proximity to vital structures, such as the inferior alveolar canal. Several studies have been carried out to determine the accuracy of cone beam CT (CBCT).1-7 However, these studies have utilized dry skulls without the soft tissue component. These studies have shown linear measurement to be accurate on CBCT images. Although the previous studies have shown CBCT to be accurate, some of the accuracy may be owing to the increase in contrast when soft tissues are replaced by air, and decreased scatter owing to the absence of soft tissues. It is important to determine if the accuracy of measurement is maintained with soft tissues intact as this would simulate a clinical situation more closely.
The aim of this study was to determine if the linear measurements made on the CBCT images are accurate when imaging is performed in the presence of soft tissues.
Materials and methods
The current study was based on six embalmed cadaver heads with intact soft tissue provided by the Department of Anatomy and Cell Biology of the Carver College of Medicine, University of Iowa. These specimens were either dentulous or edentulous in the areas where measurement was performed. The heads were sectioned such that the maxillary and mandibular alveolar arches were preserved along with the surrounding soft tissues. The specimens were mounted on a base of dental stone in order to ensure that the vertical orientation of the specimen was consistent for CBCT imaging and thereafter for sectioning with a band saw. Subsequently, fiduciary markers made of gutta percha were placed on either side of the mandible along the buccal and lingual alveolar ridges as follows. The selection of marker material was based on the radiopacity of the material and size of the marker such that they were more radiopaque than the surrounding tissues and small enough not to be visible in more than one or two orthogonal slices. Three markers were placed on the buccal surface of the alveolar process so that they were aligned and contiguous. A marker was placed, by eye, on the lingual so that it was in apparent alignment with the middle bead. The purpose of placing three markers buccally was to ensure that at least one of the markers was in alignment with the lingual bead on imaging. This plane of alignment determined the plane of measurement for both CBCT and physical measurements. The heads were then imaged using the Galileos CBCT unit (Sirona Dental Systems Inc., Bensheim, Hessen, Germany). Three-dimensional (3D) imaging data were acquired at 85 kV and 42 mAs. The scan time was 14 s. The X-ray detector for the unit was a 9 inch (23 cm) image intensifier and a charge-couple device camera. The fixed field of view size of 15 cm resulted in a scan volume of 15 × 15 × 15 cm. Reconstructed 3D data, together with the original two-dimensional projection views, were saved in a proprietary data format file. Once the images were reconstructed, they were viewed to check for the alignment of the beads on the orthoradial slices. The buccal bead that appeared to be best aligned with the lingual bead on the orthoradial slice was selected and noted on the specimen (Figure 1). In the CBCT images, the cross-sectional image that showed the lingual and one of the buccal markers in alignment was selected as the plane of measurement.
Figure 1.

Cone beam CT images showing the plane of measurement on the left side of the specimen. Top window: reconstructed panoramic image with the slicing window placed over the plane of measurement. Bottom left window: cross-sectional image corresponding to the slicing window on top. The image shows a cross-section of the mandible with spherical radiopaque markers placed over buccal and lingual alveolar ridges. A measurement tool was used to draw tangents along the superiormost and inferiormost points of the bone. Vertical distance was measured between the two tangents which depicted the height of bone at this location. Bottom right window: axial image showing the focal trough and the axial plane corresponding to the plane of measurement
An indelible ink marker was used on the specimen to indicate the proposed slicing plane. The plane selected corresponded to a line that connected the lingual bead to the buccal bead that appeared on the same orthoradial slice as the lingual bead, thereby ensuring that the physical cut of the specimen was identical to the orthoradial slice used for the measurement on the image (Figure 2). On this cross-sectional image, a horizontal tangent was drawn electronically using the measurement tool in Sirona software (Sirona Dental Systems Inc.) touching the most superior point on the bone and another touching the most inferior point of the bone. The vertical height was measured between these two tangents using the measurement tool in Sirona software. The same protocol was carried out on the opposite side of the mandible where fiduciary markers were also placed. Three measurements were obtained for each side of the mandible on three different days. All measurements throughout were made by the same single observer (RG). A similar procedure was followed for the remaining five specimens.
Figure 2.

Specimen mounted on a base, demonstrating the mandible surrounded by intraoral and extraoral soft tissues. The proposed plane of dissection, corresponding to the plane of measurement, is indicated by arrows
The specimens were dissected after imaging so that the maxilla, with its adjoining soft tissue, was removed. The mandible with surrounding soft tissues was retained. The specimens were then sliced using a band saw (Craftsman, Sears Roebuck & Co., Hoffman Estates, IL) along the plane marked previously using indelible ink.
The specimens were kept in the same vertical orientation as in the CBCT using the base made for each specimen. An instrument designed in the medical instrument shop (University of Iowa) was used to make a tangent to determine the highest and the lowest point. The purpose of using this instrument was to reproduce in the specimen the same superiormost and inferiormost points of the bone as in the image (Figure 3). These points were again marked with indelible ink. The distance between the two points was measured using a pair of digital vernier calipers (Mitutoyo Corporation, Kawasaki, Kanagawa, Japan) (Figure 4). The accepted measurement of the distance between the superiormost and inferiormost point of a given section of bone at a particular site was the mean of the measurements of the sectioned bone. This mean measurement was used as the physical measurement and the gold standard of the height of bone for the particular site. Three measurements were made at each site on three different days. In order to ensure that the measurement with vernier calipers was absolutely in the vertical plane, a 6 inch combination square was used as a guide for the vertical. The measurement was made so that the reading on the caliper was facing away from the measurer to avoid bias. The measurements of the height of bone obtained from CBCT images and caliper measurements from six specimens were compared.
Figure 3.

Tangent locater for determining the superiormost and inferiormost points of the cross-section of mandible on the specimen (indicated by arrows)
Figure 4.
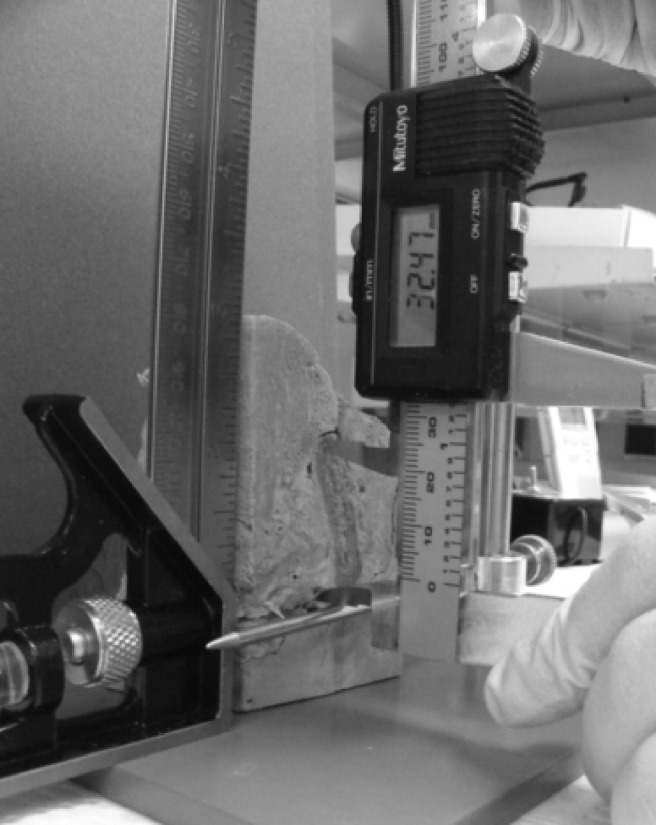
Physical measurement of bone height with calipers between the superiormost and inferiormost points of the cross-section of mandible
An overview of statistical methods
Descriptive statistics were calculated. A paired sample t-test was used to determine whether there was a significant difference between CBCT and physical measurements. The same test was also used for reliability measurements by testing for the difference between first and second, first and third, or second and third measurements which were made on the same specimen. In addition, the intraclass correlation was computed as a measure of agreement between the first and second, first and third, or second and third measurements.
Statistical analyses were carried out with the statistical package SAS® System version 9.1 (SAS Institute Inc, Cary, NC). All tests employed a 0.05 level of statistical significance.
Results
Data preparation
Six randomly selected cadaver heads were used in this study. Six paired (left and right) measurements were made from each specimen using CBCT measurement tool and calipers (two measurement modalities), comprising three pairs of CBCT and three pairs of physical measurements. In order to assure the independence of samples for performing the appropriate statistical analysis, for each measuring modalities, the average of three measurements at left or right side or the average of six measurements from the same specimen was used for the data analysis. Therefore, there were a total of six paired samples that were used for each measurement modality in this study.
Statistical analysis
Testing the difference between CBCT and physical measurements on each of the right and left sides as well as overall difference: in order to compare the two measurements made on the same head on the right side with CBCT and calipers, a new variable called “Diff_R” (Diff_R = CBCT_R–physical_R) was created. Similarly, another variable “Diff_L” (Diff_L = CBCT_L–physical_L) was created for the left side. In order to compare the overall difference between two measurements made from the same head with CBCT and calipers, a “Diff_Both” (Diff_Both = CBCT–physical) was created. A paired-sample t-test was used to determine whether the mean difference measurement value of two measurements on the right side, left side and the overall measurement was significantly equal to zero. The data revealed that there was no statistically significant difference between CBCT and physical measurements on the right side (P > 0.05), left side (P > 0.05) and overall (P > 0.05). The mean difference values are presented in Table 1. Figure 5 presents a graphical representation of the mean values of bone height using CBCT and calipers.
Table 1. Descriptive statistics of linear measurements of bone height (cone beam CT (CBCT) and physical).
| Variable a | Specimens (N) | Mean (mm) | Standard deviation | Min. (mm) | Max. (mm) | Median (mm) | Lower 95% CI for mean (mm) | Upper 95% CI for mean (mm) |
| CBCT_R | 6 | 30.48 | 6.97 | 20.54 | 37.76 | 32.71 | 23.17 | 37.80 |
| Physical_R | 6 | 30.90 | 6.35 | 22.34 | 37.96 | 32.69 | 24.24 | 37.56 |
| Diff_R | 6 | −0.42 | 0.75 | −1.80 | 0.19 | −0.11 | −1.20 | 0.37 |
| CBCT_L | 6 | 30.32 | 7.03 | 21.03 | 36.74 | 33.13 | 22.94 | 37.70 |
| Physical_L | 6 | 30.52 | 6.58 | 21.67 | 36.71 | 33.09 | 23.62 | 37.42 |
| Diff_L | 6 | −0.20 | 0.48 | −0.94 | 0.28 | −0.01 | −0.71 | 0.31 |
| CBCT | 6 | 30.40 | 6.81 | 21.39 | 37.25 | 32.92 | 23.26 | 37.55 |
| Physical | 6 | 30.71 | 6.27 | 22.76 | 37.34 | 32.89 | 24.13 | 37.29 |
| Diff_Both | 6 | −0.31 | 0.61 | −1.37 | 0.23 | −0.06 | −0.95 | 0.33 |
CI, confidence interval. aDiff_R = CBCT_R–physical_R; Diff_L = CBCT_L–physical_L; Diff_Both = CBCT–physical
Figure 5.
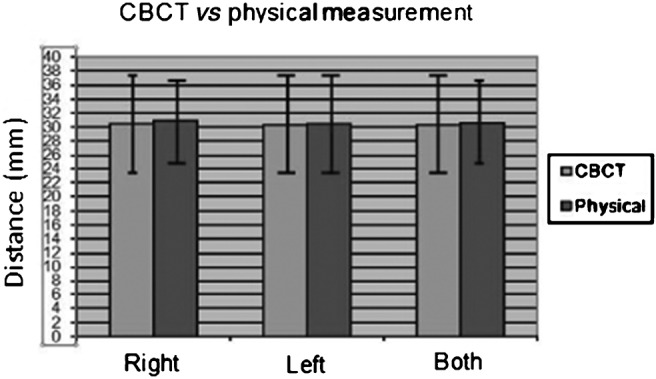
Cone beam CT (CBCT) vs physical measurements. Figure represents mean values of bone height using CBCT and calipers as measured on the right side, left side and overall (both)
Reliability of measurement: four measurements were made per specimen, two by calipers and two on CBCT images for both sides of the specimen. A total of 24 measurements were thus obtained for all 6 specimens. These measurements were repeated three times for each specimen. The measurements were assigned variables M1, M2 and M3 for the first, second and third measurements, respectively. In order to evaluate the reliability of duplicate measurements made by a single observer, three new variables, “Diff_M12” (Diff_M12 = first measurement–second measurement), “Diff_M13” (Diff_M13 = first measurement–third measurement), and “Diff_M23” (Diff_M23 = second measurement–third measurement), were created.
When combining measurements of two modalities (CBCT and physical) together, no statistically significant differences were found between the first and second measurements (P > 0.05), between the first and third measurements (P > 0.05) and between the second and third measurements (P > 0.05). The mean differences between each of those two measurements are presented in Table 2. In addition, intraclass correlation was computed as a measure of intraobserver agreement between the first and second, the first and third or the second and third measurements. Data showed that the intraclass coefficient was significantly different from zero (P < 0.05 for each instance) and intraclass coefficients of 0.9008 (first vs second measurements), 0.9004 (first vs third measurements) and 0.8950 (second vs third measurements) indicated strong agreement between the duplicated measurements made by the single observer.
Table 2. Mean difference between two measurements made by the same observer.
| Variable a | Specimens (N) | Mean (mm) | Standard deviation | Min. (mm) | Max. (mm) | Median (mm) | P-value |
| Diff_M12 | 24 | −0.08 | 0.24 | −0.44 | 0.30 | −0.11 | 0.1237 |
| Diff_M13 | 24 | −0.05 | 0.40 | −0.70 | 0.66 | −0.02 | 0.5608 |
| Diff_M23 | 24 | 0.03 | 0.26 | −0.33 | 0.51 | 0.00 | 0.5809 |
aDiff_M12 = Measurement1-Measurement2; Diff_M13 = Measurement1-Measurement3; Diff_M23 = Measurement2-Measurement3
Considering CBCT measurements only, there were no statistically significant differences between the first and second measurements (P > 0.05), between the first and third measurements (P > 0.05) and between the second and third measurements (P > 0.05). The mean differences between each of those two measurements are presented in Table 3. Additionally, data showed that the intraclass coefficient was significantly different from zero (P < 0.05 for each instance), and intraclass coefficients of 0.9096, 0.9067 and 0.9064 for each instance indicated strong agreement between the duplicated measurements made by a single observer.
Table 3. Mean difference between two measurements made by the same observer.
| Method = CBCT | |||||||
| Variable a | Specimens (N) | Mean (mm) | Standard deviation | Min. (mm) | Max. (mm) | Median (mm) | P-value |
| Diff_M12 | 12 | −0.09 | 0.19 | −0.44 | 0.16 | −0.12 | 0.1119 |
| Diff_M13 | 12 | −0.09 | 0.33 | −0.63 | 0.41 | 0.02 | 0.3402 |
| Diff_M23 | 12 | −0.00 | 0.26 | −0.33 | 0.51 | −0.01 | 0.9826 |
| Method = Physical | |||||||
| Variable a | Specimens (N) | Mean (mm) | Standard deviation | Min. (mm) | Max. (mm) | Median (mm) | P-value |
| Diff_M12 | 12 | −0.06 | 0.29 | −0.44 | 0.30 | −0.13 | 0.4714 |
| Diff_M13 | 12 | −0.00 | 0.46 | −0.70 | 0.66 | −0.09 | 0.9976 |
| Diff_M23 | 12 | 0.06 | 0.27 | −0.27 | 0.50 | 0.05 | 0.4524 |
CBCT, cone beam CT. aDiff_M12 = Measurement1–Measurement2; Diff_M13 = Measurement1–Measurement3; Diff_M23 = Measurement2–Measurement3
Regarding physical measurements, there were no statistically significant differences between the first and second measurements (P > 0.05), between the first and third measurements (P > 0.05) and between the second and third measurements (P > 0.05). The mean differences between each of those two measurements are presented in Table 3. Intraclass coefficient was significantly different from zero (P < 0.05 for each instance), and intraclass coefficients of 0.9001, 0.9029 and 0.8925 for each instance indicated strong agreement between the duplicated measurements made by a single observer.
Discussion
Radiological evaluation is necessary for information on quantity and quality of bone available for implant placement and to localize the anatomical structures.
The measurement error is generally required to be less than 1 mm on images made for implant treatment.8 In studies9,10 using cadaver mandibles, the measurement error was found to be less than 1 mm in 94% of cases using CT, 39% of cases with conventional tomography, 53% of cases using intraoral radiography and 17% of cases with panoramic radiography. CBCT is a new technology that provides cross-sectional images without superimposition or blurring11,12 and reduces the radiation dose significantly.13,14 CBCT provides 3D imaging dedicated to the maxillofacial region at a low cost and low dose of radiation.
Few studies have been carried out in the past evaluating the geometric accuracy of the available CBCT units. In these studies, linear measurements were made between anatomical sites of dry skulls using CBCT measuring tools and compared with caliper measurements1,2,4,5 or conventional CT measurements3 between the same points. The measurements were found to be sufficiently accurate for clinical use. Accuracy of linear measurements on multislice spiral CT images (Toshiba Aquilion, Toshiba Medical System Corp., Tokyo, Hongo, Japan) in comparison with caliper measurements utilizing cadaver heads with intact soft tissues was determined by Cavalcanti and co-workers.15 There was no apparent effect of the soft tissues on the accuracy of measurement as there was no statistically significant difference (P > 0.05) between imaging measurements and physical measurements obtained with calipers.
In the current study, the specimens selected were human embalmed cadaver heads with intact soft tissue around and within the jaws in its original anatomic relationship. This was in contrast with previous studies which utilized dry skulls for the evaluation of accuracy of linear measurements between anatomical points on the skull. The measurements in these studies were carried out between external points on the skull. This could be significantly different from measurements made between points within the bone as the X-ray beam undergoes attenuation on passing through not only external soft tissue but also the soft tissue within the bone. The image contrast is more when bone is imaged against air, as with a dry skull, than imaging bone against soft tissue, as in the case of live patients. Imaging dry skulls may show a high accuracy of measurement because the image contrast is high, which adds to the ease of delineating structures and boundaries of structures. Having soft tissue surrounding the bone not only reduces this contrast, but also provides an additional source of scatter radiation, thus altering the image contrast which may compromise accurate localization of points on images. Other than soft-tissue attenuation, the accuracy of measurement between different landmarks may be affected by a reduction in image quality due to metallic artifacts and patient motion. Variation in scanning protocol such as voxel size and number of projection images may also influence dimensional accuracy. This study has incorporated the issue of soft-tissue attenuation by using cadaver heads simulating patient heads as closely as possible. The soft tissue around both the jaws was intact during imaging as well as the tissue within the bone. Even though the CBCT images do not distinguish between the different types of soft tissues, the soft-tissue coverage as well as the internal soft tissue may degrade the image quality. Other factors such as patient motion, which may degrade image quality and thus compromise measurement accuracy, were not applicable in this situation as these were not live samples. Some specimens used in this study had metallic restorations, but measurements were not significantly affected in these samples as the associated artefacts were away from the region of measurements. In the current study, the linear measurements were made between the superiormost point and the inferiormost point of the mandibular bone at a particular plane. This plane of measurement was consistent between the CBCT and physical measurements. The plane was determined by placement of radiopaque fiduciary markers on the buccal and lingual surfaces of the bone such that both these markers were visualized on a single orthogonal slice on the CBCT images. The selection of the marker was based on the radiopacity of the material and size of the marker so that they were more radiopaque than the surrounding tissues and small enough not to be visible in more than one or two orthogonal slices. The orthogonal slice in which both the lingual and a buccal marker appeared was selected for measurement. The six specimens used in the current study were measured three times on both right and left sides at the same location by the same single observer. The results showed no statistically significant difference between the CBCT and physical measurements on the right side of the specimens (P > 0.05), on the left side (P > 0.05) and overall difference between CBCT and physical (P > 0.05). The data revealed that there were no statistically significant differences between the first and second measurements (P > 0.05), between the first and third measurements (P > 0.05) and between the second and third measurements (P > 0.05) showing reproducibility of measurements. The overall mean of the physical measurements (30.71) was higher than the overall mean of the CBCT measurements (30.40), although the difference was not statistically significant. The results from the current study were in agreement with similar studies carried out previously using skulls without soft-tissue components. However, the insignificant effect of soft tissues on the accuracy of measurements as determined from this study, using the Galileos CBCT, cannot be extrapolated to other commercially available CBCT units and these units need to be tested separately for accuracy. The current study shows that attenuation of X-rays by soft tissue did not affect the accuracy of measurements of bone height on images acquired in the Galileos CBCT unit. The drawback of the study was that the measurements were made by a single observer, which may introduce bias in the study even though the measurements were made three times for the same location and the observer did not directly see the physical measurements as the scale on the calipers was away from the observer. The detector used in the Galileos CBCT unit is an image intensifier which is known to introduce noise into the images. It did not adversely affect the accuracy of measurement on the images in the current study.
Based on the statistical evaluation of the CBCT and physical measurements it can be concluded that the Galileos CBCT unit is reliable for evaluation of linear measurements between anatomic structures within the mandible in the presence of soft tissues. Based on the requirement that the measurement error is less than 1 mm on images for pre-operative implant site assessment, the Galileos CBCT is sufficiently accurate for clinical use.
Acknowledgments
The University of Iowa, College of Dentistry, Dows Institute of Dental Research and the Department of Anatomy and Cell Biology are acknowledged for their contribution to the research.
References
- 1.Lascala CA, Panella J, Marques MM. Analysis of accuracy of linear measurements obtained by cone beam computed tomography (CBCTNewTom). Dentomaxillofac Radiol 2004;33:291–294 [DOI] [PubMed] [Google Scholar]
- 2.Ludlow JB, Laster WS, See M, Bailey LTJ, Hershey HG. Accuracy of measurements of mandibular anatomy in cone beam computed tomography images. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;103:534–542 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Mischkowski RA, Pulsfort R, Ritter L, Neugebauer J, Brochhagen HG, Keeve E, et al. Geometric accuracy of a newly developed cone-beam device for maxillofacial imaging. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;104:551–559 [DOI] [PubMed] [Google Scholar]
- 4.Stratemann SA, Huang JC, Maki K, Miller AJ, Hatcher DC. Comparison of cone beam computed tomography imaging with physical measures. Dentomaxillofac Radiol 2008;37:80–93 [DOI] [PubMed] [Google Scholar]
- 5.Periago DR, Scarfe WC, Moshiri M, Scheetz JP, Silveira AM, Farman AG. Linear accuracy and reliability of cone beam CT derived 3-dimensional images constructed using an orthodontic volumetric rendering program. Angle Orthodontist 2008;78:387–395 [DOI] [PubMed] [Google Scholar]
- 6.Veyre-Goulet S, Fortin T, Thierry A. Accuracy of linear measurement provided by cone beam computed tomography to assess bone quantity in the posterior maxilla: a human cadaver study. Clin Implant Dent Relat Res 2008;10:226–230 [DOI] [PubMed] [Google Scholar]
- 7.Lagravère MO, Carey J, Toogood RW, Major PW. Three-dimensional accuracy of measurements made with software on cone-beam computed tomography images. Am J Orthod Dentofacial Orthop 2008;134:112–116 [DOI] [PubMed] [Google Scholar]
- 8.Wyatt CC, Pharoah MJ. Imaging techniques and image interpretation for dental implant treatment. Int J Prosthodont 1998;11:442–452 [PubMed] [Google Scholar]
- 9.Petrikowski CG, Pharoah MJ, Schmitt A. Presurgical radiographic assessment for implants. J Prosthet Dent 1989;61:59–64 [DOI] [PubMed] [Google Scholar]
- 10.Bolin A, Eliasson S, von Beetzen M, Jansson L. Radiographic evaluation of mandibular posterior implant sites: Correlation between panoramic and tomographic determinations. Clin Oral Implants Res 1996;7:354–359 [DOI] [PubMed] [Google Scholar]
- 11.Mozzo P, Procacci C, Tacconi A, Martini PT, Andreis IA. A new volumetric CT machine for dental imaging based on the cone-beam technique: preliminary results. Eur Radiol 1998;8:1558–1564 [DOI] [PubMed] [Google Scholar]
- 12.Arai Y, Tammisalo E, Iwai K, Hashimoto K, Shinoda K. Development of a compact computed tomographic apparatus for dental use. Dentomaxillofac Radiol 1999;28:245–248 [DOI] [PubMed] [Google Scholar]
- 13.Ludlow JB, Davies-Ludlow LE, Brooks SL. Dosimetry of two extraoral direct digital imaging devices: NewTom cone beam CT and Orthophos Plus DS panoramic unit. Dentomaxillofac Radiol 2003;32:229–234 [DOI] [PubMed] [Google Scholar]
- 14.Hashimoto K, Arai Y, Iwai K, Araki M, Kawashima S, Terakado M. A comparison of a new limited cone beam computed tomography machine for dental use with a multidetector row helical CT machine. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2003;95:371–377 [DOI] [PubMed] [Google Scholar]
- 15.Cavalcanti MGP, Ruprecht A, Vannier MW. 3D volume rendering using multislice CT for dental implants. Dentomaxillofacial Radiology 2002;31:218–223 [DOI] [PubMed] [Google Scholar]