

Abstract
In this article we report a case of desmoplastic ameloblastoma in which chronological changes in the early development can be observed on dental radiographs. The tumour grew very slowly and did not appear to have a strong potential for local extension like typical ameloblastomas. Radiological findings of our case suggest the tumour arose from the periodontal membrane. However, it was not possible to obtain conclusive histopathological evidence.
Keywords: desmoplastic ameloblastoma, imaging, diagnosis
Introduction
Ameloblastomas are the most common benign odontogenic neoplasms. In 1984, Eversole et al first described the desmoplastic variant of ameloblastoma,1 which was included in the 1992 edition of the World Health Organization histopathological typing of odontogenic tumours. This tumour is a very rare variant of ameloblastoma.2,3
Recently, some authors have suggested that desmoplastic ameloblastoma tends to exhibit rapid growth2,4,5 and progressive behaviour.6 The potential for recurrence of desmoplastic ameloblastoma is considered to be very similar to that of other intraosseous ameloblastomas, excluding some subtypes of the unicystic ameloblastoma.7 However, the details of this have yet to be clarified.
In this paper, we present a case of desmoplastic ameloblastoma in which chronological changes in early development were observed on dental radiographs.
Case report
A 55-year-old female was referred to the Department of Oral and Maxillofacial Surgery, Niigata University Medical and Dental Hospital, Niigata, Japan, by her family dentist because of a mixed radiolucent/radiopaque lesion of the right maxilla identified on panoramic radiography. Almost a year before the first visit to the family dentist, she noticed a painless hard mass in the right maxillary premolar region and the mass had gradually increased in size. At the first medical examination a bone expansion was detected in the right maxillary premolar region. Buccolingual expansion of the maxillary process was observed and the maximum diameter was approximately 18 mm. The covering mucosa appeared to be normal. The adjacent right canine tooth was vital and the right first premolar tooth was non-vital. There was slight percussion pain in both teeth and no sensory paralysis was detected.
A panoramic radiograph (Figure 1) showed an ill-defined multilocular lesion with a honeycomb appearance between the canine and the first premolar of the right maxilla. Although the roots of both canine and the first premolar were displaced by the lesion, the floor of maxillary sinus remained normal.
Figure 1.

Panoramic radiograph from the initial examination. An ill-defined multilocular mixed radiopaque/radiolucent lesion between the canine and the first premolar of the right maxilla is shown. The roots of the canine and the second molar are displaced
A dental radiograph (Figure 2) showed disappearance of the lamina dura of the canine and the first premolar adjacent to the lesion. Root resorption of the teeth was not observed.
Figure 2.
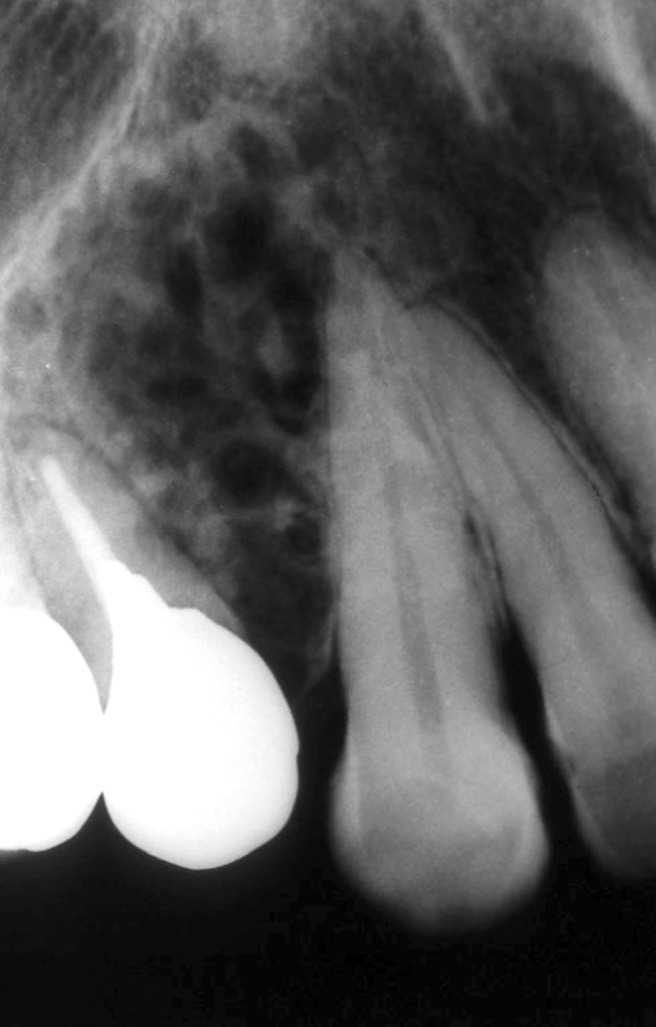
A dental radiograph from the initial examination. Note disappearance of lamina dura without root resorption of the canine and the first premolar
Axial CT in the bone window (Figure 3) demonstrated a lesion in the right maxillary alveolar process between the canine and the first premolar. The lesion mainly expanded the cortical plate of the maxillary alveolar process buccolingually. The margin of the lesion was unclear and irregular. The inside of the lesion showed an irregular matrix like a microcalcification. On a multiplanar reconstruction of the CT image parallel to the dental arch, the lamina dura of the canine adjacent to the lesion was also unclear and irregular (Figure 4). These findings raised the differential diagnosis of the lesion to an intraosseous benign tumour, such as odontogenic myxoma, fibro-osseous lesion or desmoplastic ameloblastoma.
Figure 3.

Axial CT in bone window at two different locations in the maxilla showing buccolingual expansion of the cortical plate of the maxillary alveolus
Figure 4.

Multiplanar reconstructed CT image parallel to the dental arch. Note the disappearance of the lamina dura of the canine adjacent to the lesion
After its benign nature was confirmed by biopsy, the patient underwent partial maxillectomy and histopathological examination of the surgically removed sample revealed that the lesion was a desmoplastic ameloblastoma (Figure 5a).
Figure 5.

Histopathological specimen (haematoxylin–eosin stain, ×100). (a) The specimen shows that the tumour is composed of rich fibrous connective tissue with a scattering of ameloblastomatous foci. (b) The ameloblastomatous foci are small and complicated in shape. The ameloblastomatous foci are often atrophic or hyperkeratotic owing to enhanced fibrosis around them
Histopathologically, the tumour was composed of rich fibrous connective tissue with a scattering of ameloblastomatous foci. The tumour foci were small, complicated in shape and often atrophic or hyperkeratotic owing to enhanced fibrosis around them (Figure 5b).
Dental radiographs taken 3 and 8 years before the patient's first visit to our hospital were provided by her family dentist (Figure 6a,b). At first the lesion could be identified as a small radiolucent focus near the alveolar crest between the canine and the first premolar. The lamina dura of the canine next to the lesion was unclear even at this stage. The lesion developed gradually and the lamina dura of the canine became increasingly unclear during the period of observation.
Figure 6.

(a) Dental radiograph 8 years before the first visit to our hospital. Note the radiolucent lesion between the canine and the first premolar near the alveolar crest (arrow). The lamina dura and the periodontal ligament space next to the lesion are unclear. (b) The dental radiograph 3 years before the first visit to our hospital. The lesion has developed in comparison with Figure 6a. The lamina dura and the periodontal ligament space of the canine have become increasingly unclear
Discussion
Histopathology of desmoplastic ameloblastoma is characterized by its infiltration into bone marrow spaces without a fibrous connective tissue capsule.8,9 The radiographic features of desmoplastic ameloblastoma are the mixed radiolucent/radiopaque lesion with an ill-defined margin similar to a benign fibro-osseous lesion.10 The histopathological and radiological appearance in this case was similar to these characteristics.
By monitoring the time-course change of the tumour on dental radiographs, it is suspected that this tumour developed from the cancellous bone near the alveolar ridge and grew very slowly. Root resorption of the adjacent teeth was not observed; therefore, this tumour did not seem to have strong potential for local expansion like typical ameloblastomas. There seemed to be some discrepancy between this case and those reported recently2-6 regarding radiographic features.
Some reports have suggested that desmoplastic ameloblastoma develops from the periodontal membrane of the related tooth. Moreover, some of them suggest that desmoplastic ameloblastoma might arise from epithelial rests of Malassez in the periodontal membrane.11,12 In this case, disappearance of the lamina dura and the periodontal ligament space of the adjacent canine root was clearly identified even on dental radiographs in the early stage of tumour development (Figure 6a). From those findings, it is speculated that this tumour arose from the periodontal membrane. However, it was not possible to obtain conclusive evidence from histopathological examination in this case.
References
- 1.Eversole LR, Leider AS, Hansen LS. Ameloblastomas with pronounced desmoplasia. J Oral Maxillofac Surg 1984;42:735–740 [DOI] [PubMed] [Google Scholar]
- 2.Louis PJ, Fugler RC, August M. Mixed radiolucent/radiopaque lesion of the maxilla. J Oral Maxillofac Surg 2000;58:86–90 [DOI] [PubMed] [Google Scholar]
- 3.Lam KY, Chan AC, Wu PC, Chau KY, Tideman H, Wei W. Desmoplastic variant of ameloblastoma in Chinese patients. Br J Oral Maxillofac Surg 1998;36:129–134 [DOI] [PubMed] [Google Scholar]
- 4.Manuel S, Simon D, Rajendran R, Naik BR. Desmoplastic ameloblastoma: a case report. J Oral Maxillofac Surg 2002;60:1186–1188 [DOI] [PubMed] [Google Scholar]
- 5.Pillai RS, Ongole R, Ahsan A, Radhakrishnan RA, Pai KM. Recurrent desmoplastic ameloblastoma of the maxilla: a case report. J Can Dent Assoc 2004;70:100–104 [PubMed] [Google Scholar]
- 6.Ng KH, Siar CH. Desmoplastic variant of ameloblastoma in Malaysians. Br J Oral Maxillofac Surg 1993;31:299–303 [DOI] [PubMed] [Google Scholar]
- 7.Philipsen HP, Reichart PA, Takata T. Desmoplastic ameloblastoma (including “hybrid” lesion of ameloblastoma). Biological profile based on 100 cases from the literature and own files. Oral Oncol 2001;37:455–460 [DOI] [PubMed] [Google Scholar]
- 8.Takata T, Miyauchi M, Ito H, Ogawa I, Kudo Y, Zhao M, et al. Clinical and histopathological analyses of desmoplastic ameloblastoma. Pathol Res Pract 1999;195:669–675 [DOI] [PubMed] [Google Scholar]
- 9.Takata T, Miyauchi M, Ogawa I, Zhao M, Kudo Y, Sato S, et al. So-called ‘hybrid’ lesion of desmoplastic and conventional ameloblastoma: report of a case and review of the literature. Pathol Int 1999;49:1014–1018 [DOI] [PubMed] [Google Scholar]
- 10.Wakoh M, Harada T, Inoue T. Follicular/desmoplastic hybrid ameloblastoma with radiographic features of concomitant fibro-osseous and solitary cystic lesions. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2002;94:774–780 [DOI] [PubMed] [Google Scholar]
- 11.Kawai T, Kishino M, Hiranuma H, Sasai T, Ishida T. A unique case of desmoplastic ameloblastoma of the mandible: report of a case and brief review of the English language literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1999;87:258–263 [DOI] [PubMed] [Google Scholar]
- 12.Kishino M, Murakami S, Fukuda Y, Ishida T. Pathology of the desmoplastic ameloblastoma. J Oral Pathol Med 2001;30:35–40 [DOI] [PubMed] [Google Scholar]