

Abstract
Objective
The aim of this study was to correlate the position of impacted maxillary canines on panoramic radiography with cone beam CT (CBCT) and analyse the labiopalatal position of canines and root resorption of permanent incisors in CBCT according to the mesiodistal position of canines on panoramic radiographs.
Methods
This study was a retrospective radiographic review of 63 patients with 73 impacted maxillary canines. The mesiodistal position of the canine cusp tip was classified by sector location and analysed on 73 impacted canines from 63 panoramic radiographs. The labiopalatal position of the impacted canines and root resorption of permanent incisors were evaluated with CBCT. The sector location on panoramic radiographs was compared with the labiopalatal position of impacted maxillary canines on CBCT. The statistical correlation between panoramic and CBCT findings was examined using the χ2 test and the Fisher's exact test.
Results
Labially impacted canines in CBCT were more frequent in Panoramic Sectors 1, 2 and 3, mid-alveolus impacted canines were more frequent in Sector 4 and palatally impacted canines were more frequent in Sector 5. There was a statistically significant association between the panoramic sectors of the impacted canines and the labiopalatal position of the canines (p < 0.001). Root resorption of permanent incisors showed a significant difference according to sector location (p < 0.001) and was observed in Sectors 3, 4 and 5.
Conclusions
This study suggests that the labiopalatal position of impacted canines and resorption of permanent incisors might be predicted using sector location on panoramic radiography.
Keywords: cuspid, teeth, impacted, radiography, panoramic, cone beam computed tomography
Introduction
Maxillary canines are the most commonly impacted teeth, second only to third molars.1,2 Disturbances in the eruption of maxillary permanent canines are common because they have the longest period of development, the most superior area of development and the most difficult path of eruption compared with any other tooth in the oral cavity.3,4 Impacted canines may result in several complications such as displacement and root resorption of adjacent teeth, cystic degeneration, canine ankylosis, shortening of the dental arch or combinations of these factors.5
Previous studies attempted to identify canine impactions early with the location of the canine cusp tip relative to the lateral incisor root on panoramic radiographs.6,7 The diagnostic information obtained from panoramic radiography is valuable for the overview and prediction of tooth eruption and treatment results. However, panoramic radiography has limitations in assessing the labiopalatal position of impacted canines and root resorption of incisors.8 The relatively high radiation dose and cost have restricted multidetector CT (MDCT) use in the evaluation of tooth impaction.9 The radiation dose of cone beam CT (CBCT) is significantly lower than MDCT and the typical overlap of dental structures visualized on panoramic radiographs is not observed.10,11 CBCT can identify and locate the position of impacted canines accurately and can also assess damage to the roots of adjacent teeth and amount of bone surrounding each tooth.4,12
Although many studies were performed on impacted canines using panoramic radiography or CBCT, we could not find any previous studies correlating the position of impacted maxillary canines on panoramic radiography with CBCT. Our study correlated the position of impacted maxillary canines on panoramic radiography with CBCT and analysed the labiopalatal position of maxillary canines and root resorption of permanent incisors relative to the mesiodistal position of maxillary canines on panoramic radiographs.
Materials and methods
This study was a retrospective radiographic review of 63 patients with 73 impacted maxillary canines. The study sample was selected from 76 patients who had CBCT ordered for localization of impacted maxillary canines after they had panoramic radiographs and clinical examinations at Pusan National University Hospital, Busan, Republic of Korea, between July 2008 and December 2009. This study was approved by the institutional review board. These patients were referred for CBCT scans by specialty clinics because they showed delayed eruption of maxillary canines or impacted canines. 13 patients with odontogenic tumours or cysts around impacted canines were excluded from the study. The patients were aged 10–56 years and the average age was 18.4 ± 10.6 years. Ten patients had bilaterally impacted canines (Table 1). Because the root of the maxillary canine is completely formed by the age of 13–15 years,13 patients were classified into two age groups: ≤ 15 years and > 15 years.
Table 1. Distribution of impacted maxillary canines according to gender and age.
|
n |
n |
Age (years) |
|||||
| ≤ 15 (years) | > 15 (years) | Total | Unilaterally | Bilaterally | Range | Mean ± SD | |
| Male | 19 | 9 | 28 | 24 | 4 | 10∼53 | 17.5 ± 9.6 |
| Female | 21 | 14 | 35 | 29 | 6 | 10∼56 | 19.1 ± 11.4 |
| Total | 40 | 23 | 63 | 53 | 10 | 10∼56 | 18.4 ± 10.6 |
SD, standard deviation.
Panoramic radiographs were made using a Proline XC (Planmeca, Helsinki, Finland) radiography unit. CBCT scans were acquired with a DCT Pro (Vatech Co., Hwasung, Republic of Korea). Scanning parameters were 90 kVp, 24 s, 4 mA, voxel size 0.4 mm and field of view 20×19 cm.
Paired panoramic radiographs and CBCT images from 63 patients were analysed. The mesiodistal position of the canine tip in relation to adjacent teeth was placed into a panoramic sector classification by Alessandri et al.14 The sector location was assessed on 73 impacted canines of 63 panoramic radiographs (Figure 1). The CBCT data volumes were reconstructed using Ez3D2009 CBCT software (Vatech Co.) and the labiopalatal position of impacted canines and resorption of incisors were assessed in static cross-sectional reformatted images. In assessing CBCT studies, each examiner reviewed the entire volume and was allowed to reformat images. The labiopalatal position of canines was classified as labial, mid-alveolus and palatal, depending on the relative position of the canine crown to adjacent teeth. Resorption of permanent incisors was classified as no resorption or resorption. No resorption meant intact root surfaces. Sector location on the panoramic radiographs was correlated with the labiopalatal position of impacted maxillary canines and resorption of incisors in CBCT images (Figure 2).
Figure 1.
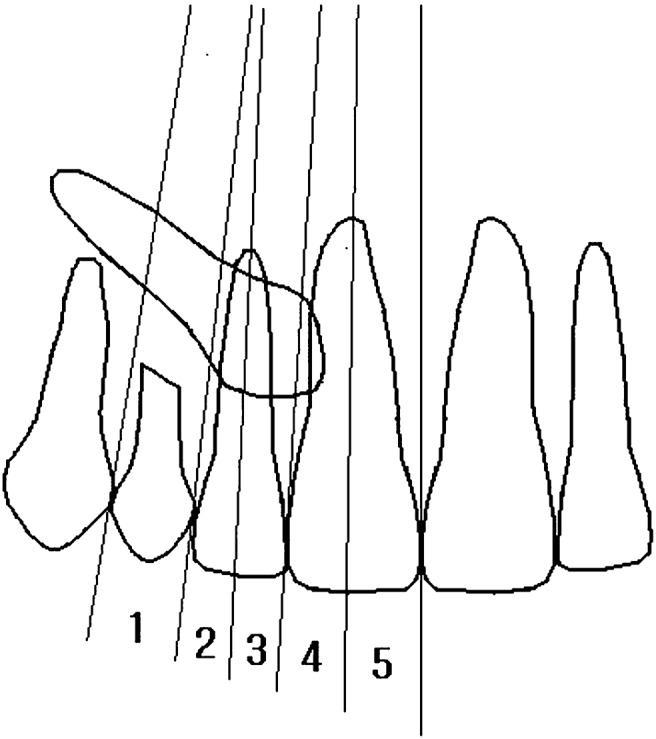
Mesiodistal position of canine cusp tip on panoramic radiography according to the sector location. (1) Corresponds to the deciduous canine; (2) indicates the distal aspect to the midline of the lateral incisor; (3) indicates the midline of the lateral incisor to the distal aspect of the central incisor; (4) indicates the distal aspect to the midline of the central incisor; and (5) indicates the midline of the central incisor to the midline of the maxillary arch
Figure 2.

(a-f) Sector location on panoramic radiograph was compared with the labiopalatal position of impacted maxillary canines in cross-sectional views of cone beam CT images. (a) Left maxillary canine is located in Sector 1 and labially impacted; (b) right maxillary canine is located in Sector 2 and labially impacted; (c) right maxillary canine is located in Sector 3 and labially impacted; (d) left maxillary canine is located in Sector 3 and labially impacted, and lateral incisor shows resorption; (e) left maxillary canine is located in Sector 4 and mid-alveolus impacted, and lateral incisor shows resorption; (f) left maxillary canine is located in Sector 5 and palatally impacted
Panoramic radiographs and CBCT volumes were reviewed twice by one oral and maxillofacial radiologist at an interval of 1 month. The other oral and maxillofacial radiologist rated the panoramic and CBCT images independently once. The panoramic radiographs and CBCT images were masked to hide patient identity and were shown in a random order. Intra-observer and interobserver agreement were evaluated using the kappa (κ) statistic. Intra-observer reliability was only established for one examiner. Intraobserver agreement was high for the panoramic images and CBCT results, showing a kappa value of 0.845 for sector location, 0.897 for labiopalatal location and 0.863 for root resorption (p < 0.001). Interobserver reliability was also high: 0.794 for sector location, 0.876 for labiolingual location and 0.825 for root resorption (p < 0.001). When the assessments of the two observers differed, a forced consensus was reached by discussion. The correlation between panoramic and CBCT findings was examined using the χ2 test and the Fisher's exact test. The level of significance was p < 0.05. All of the analyses were carried out with SPSS version 14.0 software (IBM Corporation, formally SPSS Inc, Armonk, NY).
Results
In the ≤ 15 years old group, labially impacted canines were most frequent and were more frequent in Sectors 1, 2 and 3. In the > 15 years old group, palatally impacted canines were most frequent and all cases of Sector 5 showed palatal impaction. Of the total 73 impacted maxillary canines, 30 (41.1%) were impacted labially, 23 (31.5%) in the mid-alveolus and 20 (27.4%) palatally. Labially impacted canines were more frequent in Sectors 1, 2 and 3, mid-alveolus impacted canines were most frequent in Sector 4 and palatally impacted canines were most frequent in Sector 5. There was a statistically significant association between the sectors of the canines and the labiopalatal position of the canines (p < 0.001, Table 2).
Table 2. The relationship between sector location on panoramic radiographs and labiopalatal position on cone beam CT images.
| Age (years) | Sector location | Labial | Mid-alveolus | Palatal | Total |
| ≤ 15 | 1 | 11 | 1 | 1 | 13 (27.1%) |
| 2 | 7 | 2 | 0 | 9 (18.8%) | |
| 3 | 5 | 2 | 1 | 8 (16.7%) | |
| 4 | 3 | 4 | 1 | 8 (16.7%) | |
| 5 | 0 | 6 | 4 | 10 (20.8%) | |
| Subtotal | 26 (54.2%) | 15 (31.3%) | 7 (14.6%) | 48 | |
| > 15 | 1 | 1 | 0 | 0 | 1 (4.0%) |
| 2 | 1 | 3 | 0 | 4 (16.0%) | |
| 3 | 1 | 0 | 1 | 2 (8.0%) | |
| 4 | 1 | 5 | 4 | 10 (40.0%) | |
| 5 | 0 | 0 | 8 | 8 (32.0%) | |
| Subtotal | 4 (16.0%) | 8 (32.0%) | 13 (52.0%) | 25 | |
| Total | 1 | 12 | 1 | 1 | 14 (19.2%) |
| 2 | 8 | 5 | 0 | 13 (17.8%) | |
| 3 | 6 | 2 | 2 | 10 (13.7%) | |
| 4 | 4 | 9 | 5 | 18 (24.7%) | |
| 5 | 0 | 6 | 12 | 18 (24.7%) | |
| Total | 30 (41.1%) | 23 (31.5%) | 20 (27.4%) | 73 (100%) |
In the ≤ 15 years group, Sectors 3, 4 and 5 showed root resorption of permanent incisors. In the > 15 years group, Sectors 4 and 5 showed root resorption. The ≤ 15 years group showed more frequent root resorption of permanent incisors than the > 15 years group but there was no statistically significant difference between the two groups. Resorption of permanent incisors was present in 22 patients (30.1%), was observed in Sectors 3, 4 and 5 and showed significant differences according to sector location (p < 0.001, Table 3). In both age groups, root resorption was more frequently observed in the mid-alveolus impacted canines (p < 0.001, Table 4).
Table 3. The relationship between sector location on panoramic radiographs and resorption on cone beam CT images.
| Age (years) | Sector location | No resorption | Resorption |
| ≤ 15 | 1 | 13 | 0 |
| 2 | 9 | 0 | |
| 3 | 5 | 3 | |
| 4 | 3 | 5 | |
| 5 | 2 | 8 | |
| Subtotal | 32 (66.7%) | 16 (33.3%) | |
| > 15 | 1 | 1 | 0 |
| 2 | 4 | 0 | |
| 3 | 2 | 0 | |
| 4 | 7 | 3 | |
| 5 | 5 | 3 | |
| Subtotal | 19 (76.0%) | 6 (24.0%) | |
| Total | 1 | 14 | 0 |
| 2 | 13 | 0 | |
| 3 | 7 | 3 | |
| 4 | 10 | 8 | |
| 5 | 7 | 11 | |
| Total | 51 (69.9%) | 22 (30.1%) |
Table 4. The relationship between labiopalatal position and resorption on cone beam CT images.
| Age (years) | Labiopalatal position | No resorption | Resorption |
| ≤ 15 | Labial | 23 | 3 |
| Mid-alveolus | 4 | 11 | |
| Palatal | 5 | 2 | |
| Subtotal | 32 (66.7%) | 16 (33.3%) | |
| > 15 | Labial | 4 | 0 |
| Mid-alveolus | 5 | 3 | |
| Palatal | 10 | 3 | |
| Subtotal | 19 (76.0%) | 6 (24.0%) | |
| Total | Labial | 27 | 3 |
| Mid-alveolus | 9 | 14 | |
| Palatal | 15 | 5 | |
| Total | 51 (69.9%) | 22 (30.1%) |
Discussion
The mesiodistal position of the impacted canines on panoramic radiographs showed a statistically significant correlation with the duration of treatment.15-17 Olive17 reported that canines impacted in Sectors 4 and 5 emerged after 21 months of treatment and canines in Sectors 2 and 3 emerged after 8 months of treatment. Therefore, sector location of impacted canines on panoramic radiography could be helpful in treatment planning for impacted canines. However, panoramic radiographs are two-dimensional images and lack information about the labiopalatal position of impacted canines and root resorption of adjacent teeth. Our study evaluated correlation of sector location on panoramic radiographs with the labiopalatal position of impacted canines and resorption of incisors on CBCT.
Lindauer et al7 reported that most canines destined to become palatally impacted had cusp tips overlapping or mesial to the lateral incisor root. In the ≤ 15 years group of our study, Sectors 1, 2 and 3 showed more frequent labially impacted canines, Sector 4 showed more frequent mid-alveolus and labially impacted canines and Sector 5 showed more frequent mid-alveolus and palatally impacted canines. In the > 15 years group, the sample size in each category of Sectors 1, 2 and 3 was too small to see a pattern. In the > 15 years group, Sector 4 showed more frequent mid-alveolus and palatally impacted canines and Sector 5 showed the most frequent palatally impacted canines. In total, 26 out of 30 labially impacted canines were located in Sectors 1, 2 and 3, while 15 out of 23 mid-alveolus impacted and 17 out of 20 palatally impacted canines were located mesially to the lateral incisor and were in Sectors 4 and 5. This suggests that sector location on panoramic radiography could be used to predict the labiopalatal position of impacted canines.
Warford et al18 found that sector location provided a greater influence on the prediction of impaction than on angulation, with canine location in the more mesial sectors substantially predictive of impaction. They reported that 48.6% of impacted canines were found in Sectors 3, 4 and 5.18 Lindauer et al7 found that 41.5% of impacted teeth occurred in Sectors 3, 4 and 5. Our study showed that 54.8% of impacted canines in the ≤ 15 years group and 80.0% of impacted canines in the > 15 years group were located in Sectors 3, 4 and 5. However, Alessandri et al13 analysed a sector location on panoramic radiographs obtained from patients aged between 8 and 11 years who were not seeking orthodontic treatment. They found that in these non-orthodontic patients only 7% of canines were in Sectors 3, 4 and 5.13
Diagnosis of root resorption by impacted canines might further reduce complications during treatment and the presence or absence of root resorption will determine the treatment plan.5 In our study, root resorption was associated with 22 (30.1%) of 73 impacted canines. The percentage of root resorption was lower than the 40.5% reported by Liu et al,19 38% reported by Ericson and Kurol20 and 66.7% reported by Walker et al.21 These differences may be related to differences in sampling and patient age. Ericson and Kurol22 reported that canines in the Sectors 3, 4 and 5 comprised 65% of root resorption and when the cusp of the canine was positioned mesially to the lateral incisor, which was in Sectors 4 and 5, the risk of complications increased three-fold. In our study, root resorption was observed only in Sectors 3, 4 and 5 and root resorption was not observed in Sectors 1 and 2. 11 out of 18 impacted canines in Sector 5 showed root resorption of permanent incisors. The root resorption of permanent incisors cannot be accurately judged from conventional projection radiography alone.5 CBCT imaging was significantly better than that of panoramic radiography for determining root resorption.12 Our study suggests that when canine impactions are suspected in Sectors 3, 4 and 5 on panoramic radiography, CBCT should be considered for those with suspected incisor resorption.
In conclusion, labially impacted canines in CBCT were more frequent in Sectors 1, 2 and 3 on panoramic radiographs, mid-alveolus impacted canines were more frequent in Sector 4 and palatally impacted canines were more frequent in Sector 5. Resorption of permanent incisors was observed in Sectors 3, 4 and 5. When maxillary canines are impacted or show delayed eruption in Sectors 3, 4 and 5 on panoramic radiographs, CBCT scans would be appropriate to localize the labiopalatal position of impacted canines and assess any root resorption. The labiopalatal position of impacted canines and resorption of permanent incisors might be predicted using sector location on panoramic radiography.
References
- 1.Cooke J, Wang HL. Canine impactions: incidence and management. Int J Periodontics Restorative Dent 2006;26:483–491 [PubMed] [Google Scholar]
- 2.Abron A, Mendro RL, Kaplan S. Impacted permanent maxillary canines: diagnosis and treatment. N Y State Dent J 2004;70:24–28 [PubMed] [Google Scholar]
- 3.Bishara SE. Impacted maxillary canines: a review. Am J Orthod Dentofacial Orthop 1992;101:159–171 [DOI] [PubMed] [Google Scholar]
- 4.Bedoya MM, Park JH. A review of the diagnosis and management of impacted maxillary canines. J Am Dent Assoc 2009;140:1485–1493 [DOI] [PubMed] [Google Scholar]
- 5.Alqerban A, Jacobs R, Lambrechts P, Loozen G, Willems G. Root resorption of the maxillary lateral incisor caused by impacted canine: a literature review. Clin Oral Investig 2009;13:247–255 [DOI] [PubMed] [Google Scholar]
- 6.Schindel RH, Duffy SL. Maxillary transverse discrepancies and potentially impacted maxillary canines in mixed-dentition patients. Angle Orthod 2007;77:430–435 [DOI] [PubMed] [Google Scholar]
- 7.Lindauer SJ, Rubenstein LK, Hang WM, Andersen WC, Isaacson RJ. Canine impaction identified early with panoramic radiographs. J Am Dent Assoc 1992;123:91–92 ,95–97 [DOI] [PubMed] [Google Scholar]
- 8.Freisfeld M, Dahl IA, Jäger A, Drescher D, Schüller H. X-ray diagnosis of impacted upper canines in panoramic radiographs and computed tomographs. J Orofac Orthop 1999;60:177–184 [DOI] [PubMed] [Google Scholar]
- 9.Schulze D, Heiland M, Thurmann H, Adam G. Radiation exposure during midfacial imaging using 4- and 16-slice computed tomography, cone beam computed tomography systems and conventional radiography. Dentomaxillofac Radiol 2004;33:83–86 [DOI] [PubMed] [Google Scholar]
- 10.Ludlow JB, Davies-Ludlow LE, Brooks SL. Dosimetry of two extraoral direct digital imaging devices: NewTom cone beam CT and Orthophos Plus DS panoramic unit. Dentomaxillofac Radiol 2003;32:229–234 [DOI] [PubMed] [Google Scholar]
- 11.Ludlow JB, Davies-Ludlow LE, Brooks SL, Howerton WB. Dosimetry of 3 CBCT devices for oral and maxillofacial radiology: CB Mercuray, NewTom 3G and i-CAT. Dentomaxillofac Radiol 2006;35:219–226 [DOI] [PubMed] [Google Scholar]
- 12.Alqerban A, Jacobs R, Souza PC, Willems G. In-vitro comparison of 2 cone-beam computed tomography systems and panoramic imaging for detecting simulated canine impaction-induced external root resorption in maxillary lateral incisors. Am J Orthod Dentofacial Orthop 2009;136:764.e1–11 [DOI] [PubMed] [Google Scholar]
- 13.Ash MM, Stanley JN. Wheeler's dental anatomy, physiology, and occlusion. 9th edn St. Louis, MO: Saunders Elsevier; 2010 [Google Scholar]
- 14.Alessandri BG, Zanarini M, Danesi M, Parenti SI, Gatto MR. Percentiles relative to maxillary permanent canine inclination by age: a radiologic study. Am J Orthod Dentofacial Orthop 2009;136:486.e1–6 [DOI] [PubMed] [Google Scholar]
- 15.Stewart JA, Heo G, Glover KE, Williamson PC, Lam EW, Major PW. Factors that relate to treatment duration for patients with palatally impacted maxillary canines. Am J Orthod Dentofacial Orthop 2001;119:216–225 [DOI] [PubMed] [Google Scholar]
- 16.Fleming PS, Scott P, Heidari N, Dibiase AT. Influence of radiographic position of ectopic canines on the duration of orthodontic treatment. Angle Orthod 2009;79:442–446 [DOI] [PubMed] [Google Scholar]
- 17.Olive RJ. Factors influencing the non-surgical eruption of palatally impacted canines. Aust Orthod J 2005;21:95–101 [PubMed] [Google Scholar]
- 18.Warford JH, Jr, Grandhi RK, Tira DE. Prediction of maxillary canine impaction using sectors and angular measurement. Am J Orthod Dentofacial Orthop 2003;124:651–655 [DOI] [PubMed] [Google Scholar]
- 19.Liu DG, Zhang WL, Zhang ZY, Wu YT, Ma XC. Localization of impacted maxillary canines and observation of adjacent incisor resorption with cone-beam computed tomography. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;105:91–98 [DOI] [PubMed] [Google Scholar]
- 20.Ericson S, Kurol PJ. Resorption of incisors after ectopic eruption of maxillary canines: a CT study. Angle Orthod 2000;70:415–423 [DOI] [PubMed] [Google Scholar]
- 21.Walker L, Enciso R, Mah J. Three-dimensional localization of maxillary canines with cone-beam computed tomography. Am J Orthod Dentofacial Orthop 2005;128:418–423 [DOI] [PubMed] [Google Scholar]
- 22.Ericson S, Kurol J. Resorption of maxillary lateral incisors caused by ectopic eruption of the canines. A clinical and radiographic analysis of predisposing factors. Am J Orthod Dentofacial Orthop 1988;94:503–513 [DOI] [PubMed] [Google Scholar]