

Abstract
Objectives
The purpose of this study was to compare the accuracy of diagnoses of occlusal caries lesions from digital images captured using a photostimulable phosphor (PSP) sensor under in vivo and in vitro conditions and to present useful clinical data regarding the clinical application of the system.
Methods
The study sample comprised 60 mandibular third molars (30 sound and 30 with occlusal caries) requiring extraction. A pre-extraction and post-extraction image of each tooth were acquired using a PSP sensor. A stopwatch was used to record the time required for the clinical procedures. Patient comfort or discomfort during image acquisition was also recorded. Images were evaluated twice by three observers using a five-point scale. Kappa coefficients were calculated to assess intra- and interobserver agreement. Receiver operating characteristic (ROC) curves were used to assess the diagnostic performance of each observer for both in vivo and in vitro images. The t-test was used to compare Az values, with a significance level set at 0.05 (α _ 0.05). The time required for clinical imaging procedures in patients who claimed discomfort and in those who did not was compared using the Mann–Whitney U-test.
Results
Intraobserver agreement was almost perfect, whereas interobserver agreement was fair to moderate. No statistically significant differences were found in the accuracy of diagnoses of occlusal caries lesions using in vivo and in vitro digital images. The median time needed for image exposure was 1.04 min and the median time needed to complete the image acquisition procedure was 1.45 min.
Conclusions
The diagnosis of accuracy of occlusal caries lesions using in vivo and in vitro digital images yielded similar results.
Introduction
Solid-state detectors and photostimulable phosphor (PSP) plates are the intraoral digital radiographic techniques most commonly used in clinical dentistry for diagnosing different lesions.1 A PSP consists of a polyester base coated with crystalline halide emulsion composed of a europium-activated barium fluorohalide compound. PSP plates absorb and store X-ray energy, which is then released as phosphorescence upon stimulation by another light of an appropriate wavelength.2, 3 Digital systems offer several advantages over conventional silver halide analogue radiographic film, including reusability, reduced radiation dosage, time saving, image enhancement and ease of storage, retrieval and communication.1–4
Numerous in vitro studies have assessed the accuracy of different types of digital intraoral sensors in various diagnostic tasks that include detection of caries,5, 6 root resorption,7, 8 root fracture9, 10 and periapical lesions.11, 12 Although in vitro radiographic studies are designed to simulate clinical conditions, there are numerous variables in actual clinical practice that influence the diagnostic accuracy of two-dimensional intraoral digital and film-based diagnostic systems. These variables include angulation of the central beam, exposure time, receptor sensitivity, processing, viewing conditions, observer experience, superimposition of anatomical structures, lesion location/size and the position of the tooth in the jaw.
Considering the many recently published in vitro studies that have attempted to assess the diagnostic ability of different radiographic systems, it is important to know the extent to which in vitro findings are applicable to the clinical situation. Although the accuracy of caries diagnosis from conventional film radiographs taken in vitro has been found to be similar to that of films taken in vivo,13 no similar study has been published comparing the diagnostic accuracy of in vitro and in vivo digital intraoral radiographic systems. Therefore, the aim of the present study was to compare the diagnostic accuracy of digital images obtained using a PSP sensor from the same tooth under both in vivo and in vitro conditions in the detection of occlusal caries. The study also presents useful clinical data regarding the clinical application of one PSP system (Digora Optime, Soredex, Tuusula, Finland) in terms of time efficiency and patient comfort.
Materials and methods
The study sample consisted of 60 mandibular third molars requiring extraction for reasons including pericoronitis, ectopic localization, caries and orthodontic indication. The teeth were obtained from 60 patients, who gave their informed consent to participate in the study. Of the 60 teeth included, clinical examination and subsequent histological analysis showed 30 to be sound and 30 to have occlusal caries. Pre-extraction (in vivo) and post-extraction (in vitro) images of each tooth were taken with a Trophy Trex radiographic unit (Croissy, Beaubourg, France) operated at 65 kVp and 8 mA. Images were recorded using a Digora Optime PSP digital intraoral system, which includes a feature that automatically erases residual image signals. Image recording was set at a 40 µm (super) pixel size, 14 bit greyscale, and 12.5 lp mm−1 spatial resolution. A size 2 imaging plate was used.
In total, 60 in vivo and 60 in vitro images were obtained. Exposure times for in vivo and in vitro conditions were determined by consensus. Pulpal root canal, dentine and enamel visibility were used as indicators of optimal image quality.
In vivo imaging was performed using standardized paralleling technique equipment (Rinn Manufacturing Company, Elgin, IL) with a focus–receptor distance of 20 cm and an image exposure time of 0.20 s. A stopwatch was used to record both the time required for image exposure and the time required for the final image to appear on the monitor. Patient comfort or discomfort during in vivo imaging was also observed and recorded by one researcher. Pain and vomiting reflex experienced by the patient was considered as discomfort during in vivo imaging. Obtaining PSP images in vivo consisted of the following procedures: loading the plates into barrier envelopes; attaching the envelope to the film holder; fixing the patient's position using paralleling-technique equipment; exposing the plate; opening the barrier envelope; and immediately scanning the plate under subdued lighting.
Teeth were extracted, cleaned and individually stored in 2% thymol solution. Each tooth was embedded in an acrylic block and placed behind a 1-cm-thick acrylic plate to simulate soft tissue. In vitro imaging was then performed by recording one image of each tooth bucco-lingually in the ortho-radial projection, with a focus–receptor distance of 20 cm and an image exposure time of 0.16 s. (Figures 1 and 2 show, respectively, in vivo and in vitro digital images of a mandibular third molar tooth with occlusal caries lesion).
Figure 1.

In vivo digital image of a mandibular third molar tooth with occlusal caries lesion taken with the Digora Optime PSP system
Figure 2.

In vitro digital image of a mandibular third molar tooth with occlusal caries lesion taken with the Digora Optime PSP system
In vivo and in vitro intraoral digital radiographs were evaluated separately in a dimly lit room by three oral radiologists experienced in image interpretation. The presence or absence of occlusal caries lesion was scored using the following five-point scale: 1, caries definitely present; 2, caries probably present; 3, uncertain/unable to tell; 4, caries probably not present; 5, caries definitely not present. No time restriction was placed on the observers. Images were evaluated in random order on a 38 cm computer monitor (Toshiba Satellite) with a screen resolution of 1024 × 768 pixels and 32 bit colour depth using the PSP system's software, DfW2.5 (Digora, Soredex). The observers were permitted free use of the software's built-in enhancement tools. Observers viewed all images twice, with a 2 week interval between viewing, to eliminate memory bias, in order to assess intraobserver agreement.
Histological validation of caries status was performed by serially sectioning each tooth mesiodistally in parallel to the long axis of the crown. Both sides of each section were examined under a stereomicroscope (10×) (Stemi 2000; Carl Zeiss, Jena, Germany) by one of the study authors, who recorded each tooth as either sound or as having a carious lesion, which was defined as a demineralized white or yellowish-brown discoloured area in the enamel or dentine. Histological analysis revealed 30 sound teeth and 30 teeth with occlusal caries (7 enamel and 23 dentine).
Intra- and interobserver agreements were assessed by calculating kappa coefficients.14 Kappa coefficients were evaluated according to the following criteria: < 0, no agreement; 0.0–0.20, slight agreement; 0.21–0.40, fair agreement; 0.41–0.60, moderate agreement; 0.61–0.80, substantial agreement; 0.81–1.00, almost perfect agreement. The diagnostic accuracy of each observer was measured by comparing receiver operating characteristic (ROC) curves for in vivo and in vitro images with the histological gold standard. Az values were calculated using the MedCalc statistical software package (Mariakerke, Belgium), and the t-test was used to compare Az values, with a level of 0.05 considered to be statistically significant. In addition, the time required for clinical procedures in patients who claimed discomfort and in those who did not was compared using the Mann–Whitney U-test.
Results
Kappa values for intraobserver agreement and interobserver agreement are given in Table 1. Kappa values for intraobserver agreement were almost perfect for all observers. Interobserver kappa values for the two readings between different observers were found to be fair to moderate.
Table 1. Kappa values for intraobserver agreement and interobserver agreement.
| Image type | |||
| Observer | In vivo | In vitro | |
| Intraobserver agreement kappa values | |||
| Observer 1 | 0.879 | 0.960 | |
| Observer 2 | 0.960 | 0.920 | |
| Observer 3 | 0.879 | 0.883 | |
| Interobserver agreement kappa values | |||
| Observers | Reading | In vivo | In vitro |
| Observer 1–Observer 2 | 1st reading | 0.438 | 0.490 |
| 2nd reading | 0.436 | 0.392 | |
| Observer 1–Observer 3 | 1st reading | 0.439 | 0.424 |
| 2nd reading | 0.380 | 0.447 | |
| Observer 2–Observer 3 | 1st reading | 0.386 | 0.495 |
| 2nd reading | 0.549 | 0.456 | |
No statistically significant differences were found in the accuracy of diagnosis of occlusal caries lesions using in vivo and in vitro digital images for the three observers. Az values for both image types for each observer for their first readings are shown in Table 2. ROC curves, showed no significant difference in the three observers' diagnostic accuracy of occlusal caries lesions using in vivo and in vitro images. Comparison of ROC curves, for assessments made using in vivo and in vitro images by observer 1, observer 2 and observer 3, are shown in Figures 3, 4 and 5, respectively.
Table 2. Az values for both image types for each observer for their first readings.
| Observer | Image type | Az values | Difference between areas (DBA) | Standard error of DBA | 95% CI of DBA | Significance of DBA |
| 1 | In vivo | 0.859 | 0.027 | 0.040 | −0.052 to 0.105 | 0.506 |
| In vitro | 0.886 | |||||
| 2 | In vivo | 0.861 | 0.022 | 0.051 | −0.078 to 0.122 | 0.663 |
| In vitro | 0.883 | |||||
| 3 | In vivo | 0.872 | 0.007 | 0.047 | −0.085 to 0.099 | 0.878 |
| In vitro | 0.879 |
Figure 3.
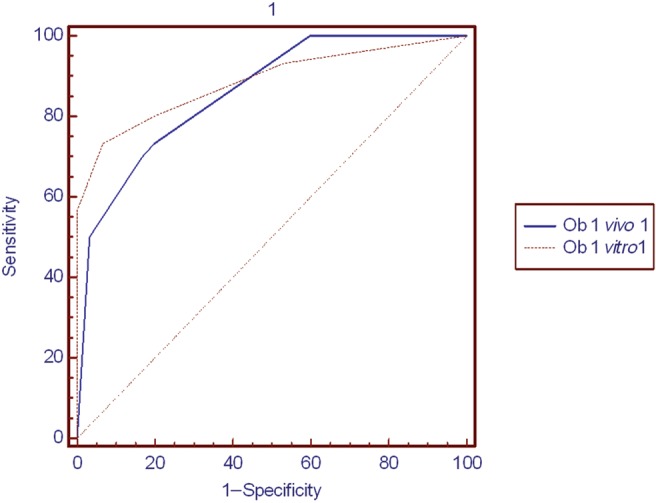
Comparison of ROC curves for assessments made using in vivo and in vitro images by observer 1
Figure 4.
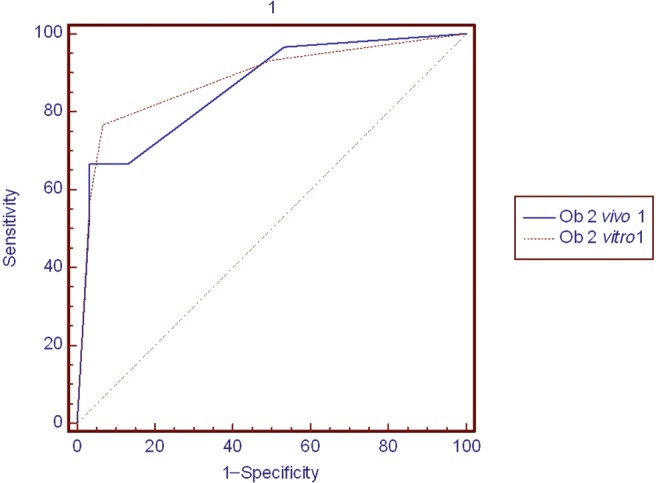
Comparison of ROC curves for assessments made using in vivo and in vitro images by observer 2
Figure 5.
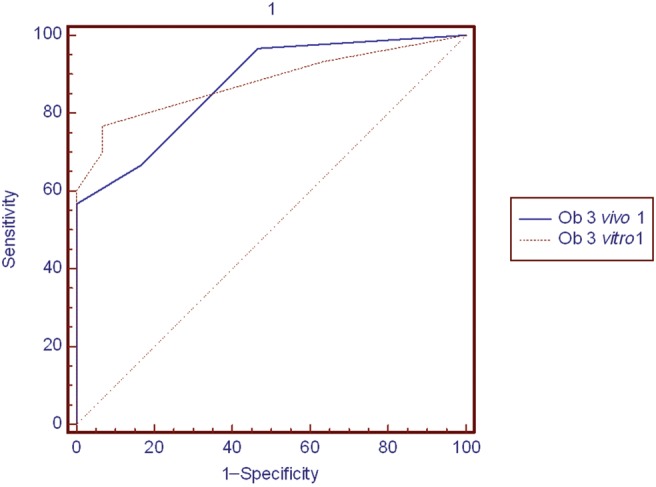
Comparison of ROC curves for assessments made using in vivo and in vitro images by observer 3
The median time required for image exposure (plate loading, envelope attachment, fixing patient position and plate exposure) was found to be 1.04 min (minimum 0.50 min and maximum 2.38 min), and the median total time required to complete the image acquisition procedure was found to be 1.45 min (minimum 1.21 min and maximum 3.24 min). A significant difference was found in both image exposure time and total image acquisition time between patients complaining of discomfort and those with no discomfort (P < 0.001). Among the 9 patients with discomfort, the median image exposure and total image acquisition times were, respectively, 2.26 min and 2.34 min, compared with only 1.02 min and 1.42 min, respectively, among the 51 patients with no discomfort.
Discussion
The present study found that the digital images obtained using a PSP sensor under clinical conditions provided similar diagnostic accuracy to in vitro images obtained in the laboratory in the detection of occlusal caries lesions. Although in vitro Az values were higher than in vivo Az values for all observers, the differences were not statistically significant. This study found almost perfect intraobserver agreement and fair to moderate interobserver agreement both in vivo and in vitro. Moreover, single in vivo digital radiographs of mandibular third molar teeth were very good in terms of time efficiency.
The frequent need for extraction of the mandibular third molar, along with the fact that occlusal caries is the most frequent lesion to affect teeth, facilitated the collection of data on both in vivo and in vitro imaging in our study. The results are similar to those of another study conducted with film radiographs that found no statistically significant differences between the ROC curves for in vivo and in vitro imaging in the diagnostic accuracy of occlusal (in vivo 0.767; in vitro 0.826) or proximal (in vivo 0.707; in vitro 0.735) caries.13 Compared with the mean Az values of that study, the Az values of the different observers in the present study were higher. In the authors opinion, providing an Az value for each observer separately is of greater statistical value than providing a mean Az value. The relatively higher Az values for in vitro images in this study can be explained by the large number of occlusal deep dentine caries and the small number of occlusal caries that were confined to enamel.
The authors believe that the closeness in diagnoses among observers and between in vivo and in vitro Az values in this study is due to the utilization of the digital software enhancement tools to adjust contrast, density, image size, sharpness and inversion parameters, which allowed observers to minimize, to a certain extent, any patient-related negative effects on clinical imaging. It should be noted that the present study was not designed to evaluate the effectiveness of different enhancement tools in occlusal caries detection, and there is still controversy regarding the effects of image enhancement on diagnostic accuracy. In one in vitro study that compared the accuracy of occlusal caries diagnoses using original and enhanced digital images, the manipulation of images using sharpness, zoom and pseudocolour tools did not affect the detection of occlusal caries lesions.6 The same study found moderate to good intraobserver agreement and good interobserver agreement, with Az values between 0.66 and 0.76 for four sixth-year dental students who acted as observers. Both this study and the present study conflict with well-known classical experimental studies that have demonstrated poor and average intra- and interobserver values for radiographic evaluation.15, 16
Because occlusal caries may progress without visible breakdown of the enamel structure, visual examination alone is not always sufficient for diagnosing occlusal caries, whereas probing, which is also used routinely in clinical examination, may cause trauma. For these reasons, it has become important to identify non-traumatic, non-invasive techniques that can accurately diagnose occlusal caries. In one of a number of recent studies assessing the diagnostic accuracy of different non-invasive techniques, an older version of an RVG system (Trophy, Vincennes, France) showed greater mean sensitivity in diagnosing occlusal caries than conventional radiography.17 Another study found digital radiography capable of detecting over 70% of deep lesions, without giving rise to additional false-positive diagnoses.18 A similar detection rate of 70% was found in another study which showed that digital radiography with contrast stretch performed better than both visual inspection and film; moreover, when contrast-manipulated digital radiographs were combined with visual inspection, the accuracy of diagnosis increased by 33%, but with an 11% increase in false positives.19 Another study found radiography to be of almost no value in the detection of proximal enamel caries lesions, but of some value in the detection of dentinal lesions on occlusal surfaces. ROC curve areas ranged from 0.62 for the Visualix (Gendex, Monza, Italy) digital dental system to 0.79 for D- and E-speed film, with no statistically significant differences among radiographic methods for either proximal or occlusal surfaces.20
Important factors affecting the performance of PSP systems include signal-to-noise ratio, PSP plate and scanner quality. The scanning resolution of storage phosphor plate radiographs was found to have no effect on the detection of proximal caries lesions. The Az value for the radiographs scanned with Digora FMX at 7.8 lp mm−1, Digora Optime at both 7.8 lp mm−1 and 12.5 lp mm−1, and Dürr VistaScan (Dürr Dental, Bietigheim-Bissingen, Germany) at 20 lp mm−1 were similar and all higher than the Dürr VistaScan at 10 lp mm−1. Mean Az values ranged between 0.599 and 0.742 for the different PSP systems utilized.21 In the present study, occlusal caries lesions were rather deep, which explains the larger ROC values compared with the above-mentioned study, which assessed proximal caries lesions. Caries diagnosis did not improve when using high-resolution settings compared with the standard settings of different digital intraoral imaging systems.22 Diagnostic accuracy of caries lesions was little influenced by an increase in spatial resolution and bit depth from 8 bit to 12 or 16 bit within digital radiographic system brands.23 The ability to detect caries has also been shown to increase with observer experience.24 Diagnostic accuracy (mean ROC curve area 0.92–0.98) and intraexaminer and interexaminer reproducibility have also been shown to be significantly higher in the detection of occlusal demineralization using the subtraction technique compared with paired digital images viewed side by side, indicating that the subtraction method can be used successfully to monitor occlusal caries.25
In the present study, only nine patients (15%) experienced notable discomfort (including pain and vomiting) during image exposure. The PSP plate is known to be sharp-edged and less flexible than film and can be damaged or broken when bent or otherwise subjected to excessive force. Moreover, the barrier envelope in which the plate is placed is larger than the plate itself, making it difficult for the technician to place the detector in the patient's mouth.
Obviously, there were retakes in the present study. In 14 patients, 2 retakes were necessary, and in 3 patients 3 retakes were necessary. However, only the time taken to obtain the accurate image was considered in the statistical analysis. Considering the general difficulties related to obtaining an image in the mandibular third molar region because of position and alignment of the third molars in the oral cavity and the time needed for an automatic processor to develop a film (3–6 min), the results suggest very good efficiency in terms of the time required to obtain a single radiograph in routine clinical practice. However, because patient-related difficulties may increase the time required for image exposure under clinical conditions, additional studies are essential for the assessment of clinical time efficiency and versatility of the newer digital systems.
One drawback of the Digora Optime scanner system is that it has a slot for scanning only one plate at a time instead of multiple slots that could be used to scan several plates simultaneously. In a previous study that compared the efficiency of two PSP dental imaging systems in terms of the time required to complete a full-mouth intraoral survey using a single manikin and operator, no statistically significant differences were found in either the time required for exposure or the total time required for obtaining a full-mouth series using the DenOptix (Kavo-Gendex, Des Plaines, IL) and the ScanX (Air Techniques, Hicksville, NY) scanners. The mean times required for exposure and for the total procedure were, respectively, 13.94 min and 31.2 min for the DenOptix and 14.61 min and 27.1 min for the ScanX.3
Conclusions
Assessment of images obtained using a PSP sensor (Digora Optime) from the same tooth under both clinical and laboratory conditions for the detection of occlusal caries revealed highly comparable results. Furthermore, in vivo time efficiency was found to be very good for single radiographs of mandibular third molars.
Acknowledgment
The authors would like to thank Ozan Bora of Soredex for providing the Digora Optime system.
References
- 1.Ludlow JB, Mol A. Digital imaging. In: White SC, Pharoah MJ (eds). Oral radiology: Principles and interpretation (5th ed). St. Louis: Mosby, 2004, pp 225–244 [Google Scholar]
- 2.Hildebolt CF, Couture RA, Whiting BR. Dental photostimulable phosphor radiography. Dent Clin North Am 2000;44:273–297 [PubMed] [Google Scholar]
- 3.Ramamurthy R, Canning CF, Scheetz JP, Farman AG. Time and motion study: a comparison of two photostimulable phosphor imaging systems used in dentistry. Dentomaxillofac Radiol 2006;35:315–318 [DOI] [PubMed] [Google Scholar]
- 4.Farman AG, Farman TT. A comparison of 18 different x-ray detectors currently used in dentistry. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005;99:485–489 [DOI] [PubMed] [Google Scholar]
- 5.Hintze H, Wenzel A, Frydenberg M. Accuracy of caries detection with four storage phosphor systems and E speed radiographs. Dentomaxillofac Radiol 2002;31:170–175 [DOI] [PubMed] [Google Scholar]
- 6.Kositbowornchai S, Basiw M, Promwang Y, Moragorn H, Sooksuntisakoonchai N. Accuracy of diagnosing occlusal caries using enhanced digital images. Dentomaxillofac Radiol 2004;33:236–240 [DOI] [PubMed] [Google Scholar]
- 7.Kamburoğlu K, Barenboim SF, Kaffe I. Comparison of conventional film with different digital and digitally filtered images in the detection of simulated internal resorption cavities: an ex vivo study in human cadaver jaws. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;105:790–797 [DOI] [PubMed] [Google Scholar]
- 8.Kamburoğlu K, Tsesis I, Kfir A, Kaffe I. Diagnosis of artificially induced external root resorption using conventional intraoral film radiography, CCD, and PSP: an ex vivo study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;106:885–891 [DOI] [PubMed] [Google Scholar]
- 9.Tsesis I, Kamburoğlu K, Katz A, Tamse A, Kaffe I, Kfir A. Comparison of digital with conventional radiography in detection of vertical root fractures in endodontically treated maxillary premolars: an ex vivo study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;106:124–128 [DOI] [PubMed] [Google Scholar]
- 10.Kositbowornchai S, Nuansakul R, Sikram S, Sinahawattana S, Saengmontri S. Root fracture detection: a comparison of direct digital radiography with conventional radiography. Dentomaxillofac Radiol 2001;30:106–109 [DOI] [PubMed] [Google Scholar]
- 11.Wallace JA, Nair MK, Abomr D, Colaco MF, Kapa SF. A comparative evaluation of the diagnostic efficacy of film and digital sensors for detection of simulated periapical lesions. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2001;92:93–97 [DOI] [PubMed] [Google Scholar]
- 12.Stavropoulos A, Wenzel A. Accuracy of cone beam dental CT, intraoral digital and conventional film radiography for the detection of periapical lesions. An ex vivo study in pig jaws. Clin Oral Invest 2007;11:101–106 [DOI] [PubMed] [Google Scholar]
- 13.Hintze H, Wenzel A. Clinical and laboratory radiographic caries diagnosis. A study of the same teeth. Dentomaxillofac Radiol 1996;25:115–118 [DOI] [PubMed] [Google Scholar]
- 14.Fleiss JL. Statistical methods for rates and proportions (2nd edn). New York, NY: John Wiley & Sons, 1981, pp 229–232. [Google Scholar]
- 15.Goldman M, Pearson AH, Darzenta N. Endodontic success: who is reading the radiograph? Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1972;33:432–437 [DOI] [PubMed] [Google Scholar]
- 16.Goldman M, Pearson AH, Darzenta N. Reliability of radiographic interpretations. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1974;38:287–293 [DOI] [PubMed] [Google Scholar]
- 17.Wenzel A, Hintze H, Mikkelsen L, Mouyen F. Radiographic detection of occlusal caries in noncavitated teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1991;72:621–626 [DOI] [PubMed] [Google Scholar]
- 18.Wenzel A, Larsen MJ, Fejerskov O. Detection of occlusal caries without cavitation by visual inspection, film radiographs, xeroradiographs, and digitized radiographs. Caries Res 1991;25:365–371 [DOI] [PubMed] [Google Scholar]
- 19.Wenzel A, Fejerskov O. Validity of diagnosis of questionable caries lesions in occlusal surfaces of extracted third molars. Caries Res 1992;26:188–194 [DOI] [PubMed] [Google Scholar]
- 20.Hintze H, Wenzel A, Jones C. In vitro comparison of D- and E-speed film radiography, RVG, and Visualix digital radiography for the detection of enamel approximal and dentinal occlusal caries lesions. Caries Res 1994;28:363–367 [DOI] [PubMed] [Google Scholar]
- 21.Li G, Berkhout WE, Sanderink GC, Martins M, van derStelt PF. Detection of in vitro proximal caries in storage phosphor plate radiographs scanned with different resolutions. Dentomaxillofac Radiol 2008;37:325–329 [DOI] [PubMed] [Google Scholar]
- 22.Berkhout WE, Verheij JG, Syriopoulos K, Li G, Sanderink GC, van derStelt PF. Detection of proximal caries with high-resolution and standard resolution digital radiographic systems. Dentomaxillofac Radiol 2007;36:204–210 [DOI] [PubMed] [Google Scholar]
- 23.Wenzel A, Haiter-Neto F, Gotfredsen E. Influence of spatial resolution and bit depth on detection of small caries lesions with digital receptors. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;103:418–422 [DOI] [PubMed] [Google Scholar]
- 24.Souza-Zaroni WC, Ciccone JC, Souza-Gabriel AE, Ramos RP, Corona SAM, Palma-Dibb RG. Validity and reproducibility of different combinations of methods for occlusal caries detection: an in vitro comparison. Caries Res 2006;40:194–201 [DOI] [PubMed] [Google Scholar]
- 25.Ricketts DNJ, Ekstrand KR, Martignon S, Ellwood R, Alatsaris M, Nugent Z. Accuracy and reproducibility of conventional radiographic assessment and subtraction radiography in detecting demineralization in occlusal surfaces. Caries Res 2007;41:121–128 [DOI] [PubMed] [Google Scholar]