

Abstract
Castleman's disease of the parotid gland is an extremely rare entity, with fewer than 20 cases reported in world literature so far and only 1 previous case report describing the ultrasound findings. The Doppler findings of parotid Castleman's disease have never been described before to the best of the authors' knowledge. This report describes the ultrasonographic and Doppler findings in a histopathologically proven case of Castleman's disease of the left parotid gland in a young man.
Keywords: parotid gland, Castleman's disease, ultrasonography
Introduction
Castleman's disease, also known as angioproliferative lymph node hyperplasia, is a rare benign lymphoproliferative disorder.1 The majority of the cases occur in the thorax, with only approximately 10–15% of the cases occurring in the head and neck region.2 Castleman's disease of the parotid gland is extremely rare, with fewer than 20 cases reported in world literature so far and only one previous case report describing the ultrasonographic findings.3 This report describes the ultrasonographic and colour Doppler findings of a histopathologically proven case of parotid Castleman's disease in a 19-year-old man.
Case report
A 19-year-old man presented to the department with a left-sided facial swelling, which he first noticed when he was 10-years-old and which had gradually increased in size over the previous 3 years. There was no associated pain or fever. Local examination revealed a left-sided parotid swelling, soft in consistency, measuring approximately 3 × 4 cm. There was no associated facial weakness. Ultrasonographly revealed a uniformly hypoechoeic lesion within the superficial lobe of the left parotid gland measuring approximately 3 × 4.5 cm with smaller adjacent surrounding hypoechoeic lymph nodes (Figure 1). Doppler examination revealed exuberant vascularity with predominantly peripheral flow (Figure 2). Prominent penetrating feeding vessels entering the hilum were seen (Figure 3). The spectral wave form showed a low-resistance arterial wave pattern (Figure 4). Surgical excision was performed and histopathological examination was suggestive of Castleman's disease (Figure 5).
Figure 1.
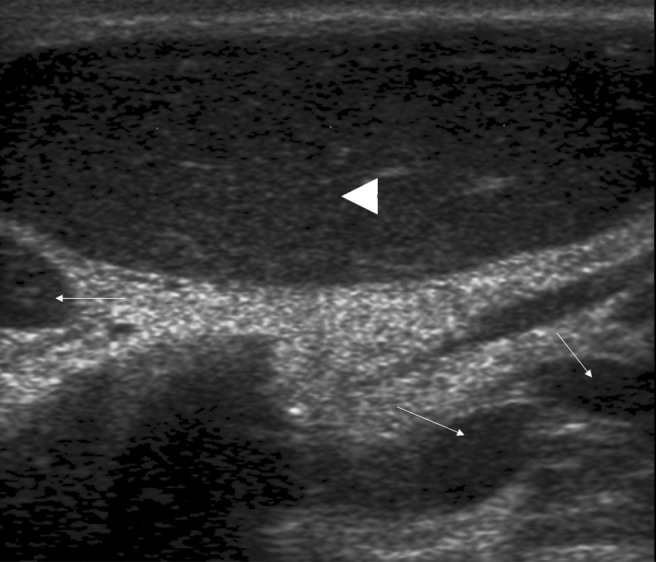
Ultrasonography of the left parotid region showing a uniformly hypoechoeic mass (arrowhead) arising from the superficial lobe of the left parotid gland. Smaller surrounding hypoechoeic intraparotid lymph nodes are seen (long white arrows)
Figure 2.
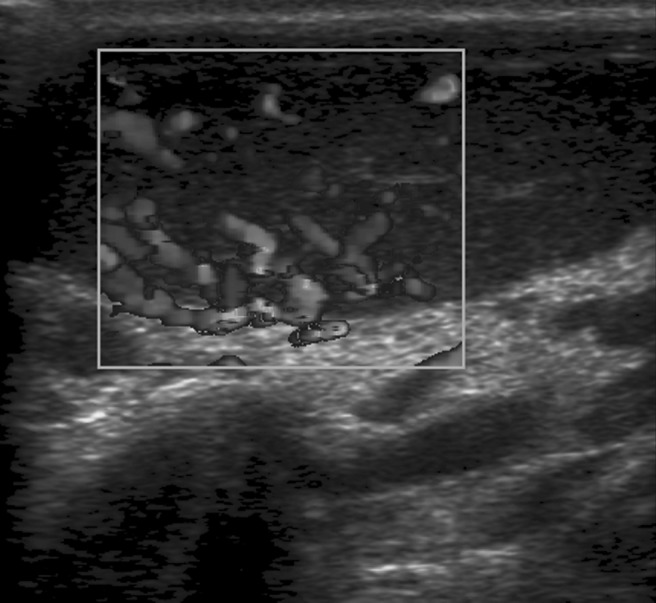
Doppler study of the mass showing exuberant peripheral vascularity
Figure 3.
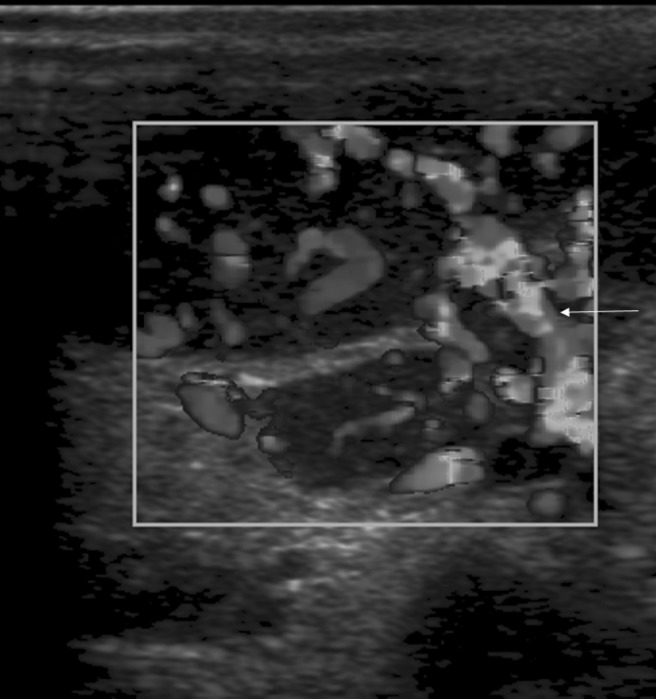
Doppler study of the mass showing prominent penetrating vessels entering the hilum (long white arrow)
Figure 4.
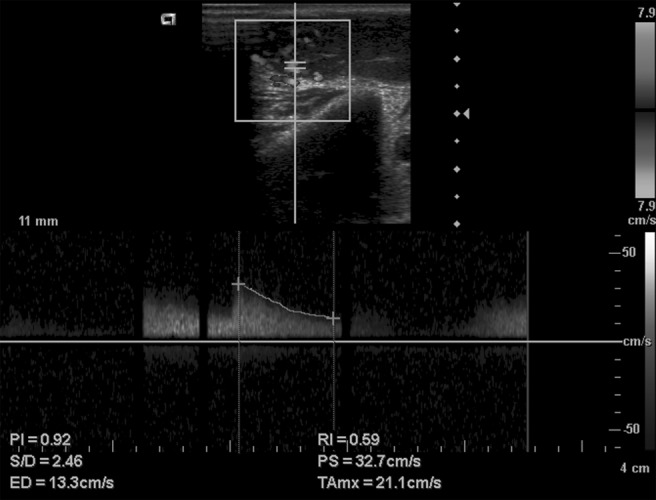
Spectral wave form showing a low-resistance arterial wave pattern
Figure 5.
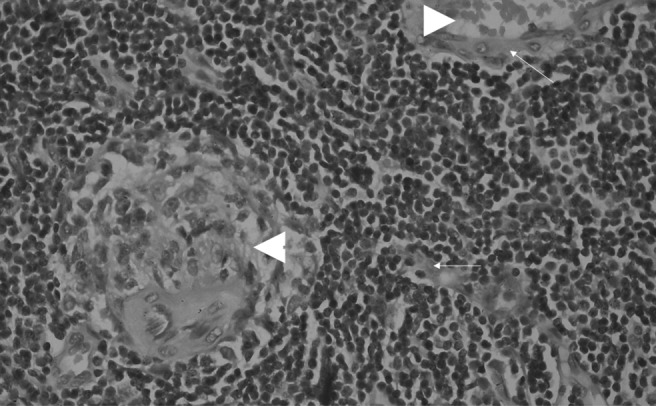
Photomicrograph (haematoxylin and eosin, 450×) showing germinal centres (white arrowheads) within a follicle with proliferative hyalinized capillaries (long white arrows)
Discussion
Castleman's disease, a benign lymphoproliferative disorder, may be localized or widespread, with the localized form having two histopathological types.3 The hyaline vascular type is seen in the majority of cases, commonly presenting with only pressure symptoms in young individuals.4
Parotid Castleman's disease is extremely rare. To the best of the authors' knowledge, fewer than 20 cases have been reported in world literature so far. There has been only one previous case report describing the ultrasonographic findings in parotid Castleman's disease, described in a 50-year-old man in whom ultrasound showed an ill-defined, heterogeneous, partly cystic mass with multiple intraparotid and cervical lymph nodes.3 In the present case, ultrasound showed a more homogeneously hypoechoeic mass with surrounding hypoechoeic intraparotid and cervical lymph nodes. The findings are more consistent with the sonographic findings described in Castleman's disease affecting other sites.5
The ultrasonographic findings are, however, not specific and may even be seen in lymphoma.5 However, the Doppler examination showed an exuberant vascular pattern with prominent peripheral vessels and penetrating feeding vessels entering the hilum, which is suggestive of Castleman's disease.2, 6 Colour Doppler and spectral analysis have been found to be useful in differentiating the different lymphadenopathies.7, 8 Benign lymph nodes are, by and large, avascular or show a hilar vascularity without peripheral flow, whereas in metastatic lymphadenopathy a spotted, peripheral or mixed pattern of vascularity is noted.8 However, the vascular patterns are not entirely specific. Benign causes, such as Kikuchi's disease, have been shown to depict an abnormal vascularity.7 Moreover, malignant conditions such as lymphoma, especially in the early stages, can depict a benign pattern of flow.8 Hence, spectral analysis is usually used to add to the specificity. Malignant lymph nodes usually depict a high resisitivity and pulsatility index (RI and PI, respectively) with a cut-off for the RI of more than 0.8 and for the PI of more than 1.5, increasing the specificity.7 The Doppler findings in parotid Castleman's disease have not been previously described in the literature. In our case, the spectral wave pattern showed a low-resistance arterial flow (RI of 0.59), which favours a benign aetiology, although the vascular pattern was of the mixed type with prominent peripheral as well as hilar flow.
Although imaging features can indicate the diagnosis, histopathological confirmation is usually required.3 Histopathological examination in this case showed germinal centres within follicles with interfollicular capillary proliferation showing hyalinization, suggestive of the hyaline vascular type of Castleman's disease.
To conclude, parotid Castleman's disease is a rare entity. Being superficial, it is readily assessed using ultrasound. The findings of a uniformly hypoechoeic mass showing exuberant peripheral vascularity with prominent penetrating hilar vessels and surrounding lymphadenopathy should indicate the diagnosis.
References
- 1.Keller AR, Hochholzer L, Castleman B. Hyaline-vascular and plasma-cell types of giant lymph node hyperplasia of the mediastinum and other locations. Cancer 1972;29:670–683 [DOI] [PubMed] [Google Scholar]
- 2.Ko SF, Hsieh MJ, Ng SH, Lin JW, Wan YL, Lee TY, et al. Imaging spectrum of Castleman's disease. AJR Am J Roentgenol 2004;182:769–775 [DOI] [PubMed] [Google Scholar]
- 3.Ahuja AT, Davey IC, Ng HK, Metreweli C. Ultrasound appearance of parotid Castleman's disease. J Clin Ultrasound. 1995;23:254–258 [DOI] [PubMed] [Google Scholar]
- 4.Hirst E, Williams HBL. Intrathoracic lymphoid hamartoma. Thorax 1964;19:469–476 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Williams JL, Kaude JV. Sonographic findings in a case of Castleman disease of the neck. J Ultrasound Med. 1986;5:593–594 [DOI] [PubMed] [Google Scholar]
- 6.Konno K, Ischida H, Hamashima Y, Komatsuda T, Massamune O. Color Doppler findings in Castleman's disease of the mesentery. J Clin Ultrasound 1998;26:474–478 [DOI] [PubMed] [Google Scholar]
- 7.Na DG, Lim HK, Byun HS, Kim HD, Ko YH, Baek JH. Differential diagnosis of cervical lymphadenopathy: usefulness of color Doppler sonography. AJR Am J Roentgenol 1997;168:1311–1316 [DOI] [PubMed] [Google Scholar]
- 8.Wu CH, Chang YL, Hsu WC, Ko JY, Sheen TS, Hsieh FJ. Usefulness of Doppler spectral analysis and power Doppler sonography in the differentiation of cervical lymphadenopathies. AJR Am J Roentgenol 1998;171:503–509 [DOI] [PubMed] [Google Scholar]