

Abstract
Background
In recent years (2000 to 2007), ambient levels of fine particulate matter (PM2.5) have continued to decline as a result of interventions, but the decline has been at a slower rate than previous years (1980 to 2000). Whether these more recent and slower declines of PM2.5 levels continue to improve life expectancy and whether they benefit all populations equally is unknown.
Methods
We assembled a dataset for 545 U.S. counties consisting of yearly county-specific average PM2.5, yearly county-specific life expectancy, and several potentially confounding variables measuring socioeconomic status, smoking prevalence and demographic characteristics for the years 2000 and 2007. We used regression models to estimate the association between reductions in PM2.5 and changes in life expectancy for the period 2000 to 2007.
Results
A decrease of 10 µg/m3 in the concentration of PM2.5 was associated with an increase in mean life expectancy of 0.35 years SD= 0.16 years, p = 0.033). This association was stronger in more urban and densely populated counties.
Conclusions
Reductions in PM2.5 were associated with improvements in life expectancy for the period 2000 to 2007. Air pollution control in the last decade has continued to have a positive impact on public health.
Since the 1970s, enactment of increasingly stringent air quality controls has led to improvements in ambient air quality in the United States at costs that the U.S. Environmental Protection Agency (EPA) has estimated as high as $25 billion per year.1 However, even with the well-established link between long-term exposure to air pollution and adverse effects on health,2 the extent to which more recent regulatory actions have benefited public health remains in question.
Air pollutant concentrations have been generally decreasing in the U.S., with substantial differences in reductions across metropolitan areas. Levels of fine particulate matter air pollution (particulate matter < 2.5 µm in aerodynamic diameter, PM2.5) remain relatively high in some areas. In a 2010 study, the EPA estimated that 62 U.S. counties, accounting for 26% of their total study population, had PM2.5 concentrations not in compliance with the National Ambient Air Quality Standards (NAAQS).3
Reductions in particulate matter air pollution are associated with reductions in both cardiopulmonary and overall mortality.2 In the mid-1990s, the Harvard Six Cities Study4 and the American Cancer Society (ACS) study5 reported associations of cardiopulmonary mortality risk with chronic exposure to fine particulate air pollution while controlling for smoking and other individual risk factors. Reanalysis and extended analyses of these studies have confirmed that fine particulate air pollution is an important independent environmental risk factor for cardiopulmonary disease and mortality.6–12 Additional cohort studies, population-based studies, and short-term time-series studies have also shown associations between reductions in air pollution and reductions in human mortality.13–21 More recently, studies have suggested an association between PM2.5 and life expectancy,22,23 a well-documented and important measure of overall public health.24–26
As our primary analysis, we estimate the association between changes in PM2.5 and in life expectancy in 545 U.S. counties during the period 2000 to 2007. This period is of particular interest, as the EPA restarted wide collection of PM2.5 data in 1999–2000, after stopping the nationwide PM2.5 monitoring program during the mid-1980s and most of the 1990s. . In secondary analyses, we extended to 2007 the data and statistical analysis originally reported by Pope and colleagues23 for the period 1980–2000, and investigated whether the relationship reported by Pope et al23 persists in the more recent years.
METHODS
Data
We constructed and analyzed three data sets to estimate the association between changes in life expectancy and changes in PM2.5 during the period 2000 to 2007 in 545 counties (Dataset 1), and to investigate whether the association previously reported by Pope et al23 persists when the data on the same 211 counties are extended to the year 2007 (Datasets 2 and 3).
Dataset 1 included information on 545 U.S. counties for the years 2000 and 2007. These counties include all counties with available matching PM2.5 data for 2000 and 2007. Additionally, unlike previous work in which counties were located only in metropolitan areas,23 Dataset 1 is comprised of counties in both metropolitan and non-metropolitan areas. Figure 1 shows the counties in this dataset shaded according to life expectancy in 2000 and 2007. Variables in this dataset were available at the county level, for both 2000 and 2007, and included: life expectancy, PM2.5, per capita income, population, proportions who were high school graduates, and proportions who were white, black, or Hispanic. Because data on smoking prevalence were not available for all 545 counties, we used age-standardized death rates for lung cancer and chronic obstructive pulmonary disease (COPD) as proxy variables for smoking prevalence.27,28 Death rates were calculated in 5-year age groups and age-standardized for the 2000 U.S. population of adults 45 years of age or older. Daily PM2.5 data were obtained from the EPA’s Air Quality System (AQS - http://www.epa.gov/ttn/airs/airsaqs/detaildata/downloadaqsdata.htm). Daily PM2.5 levels for each county were averaged across monitors within that county using a trimmed mean approach; those daily county-level means were further averaged across days to obtain a county-specific yearly PM2.5 average.29
Figure 1.
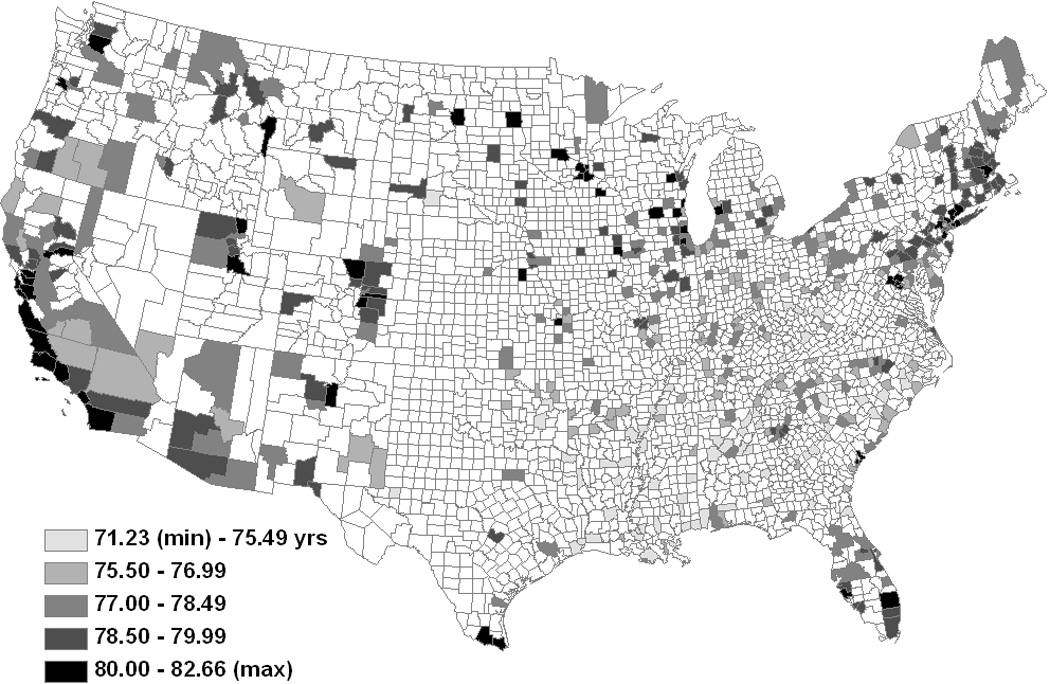
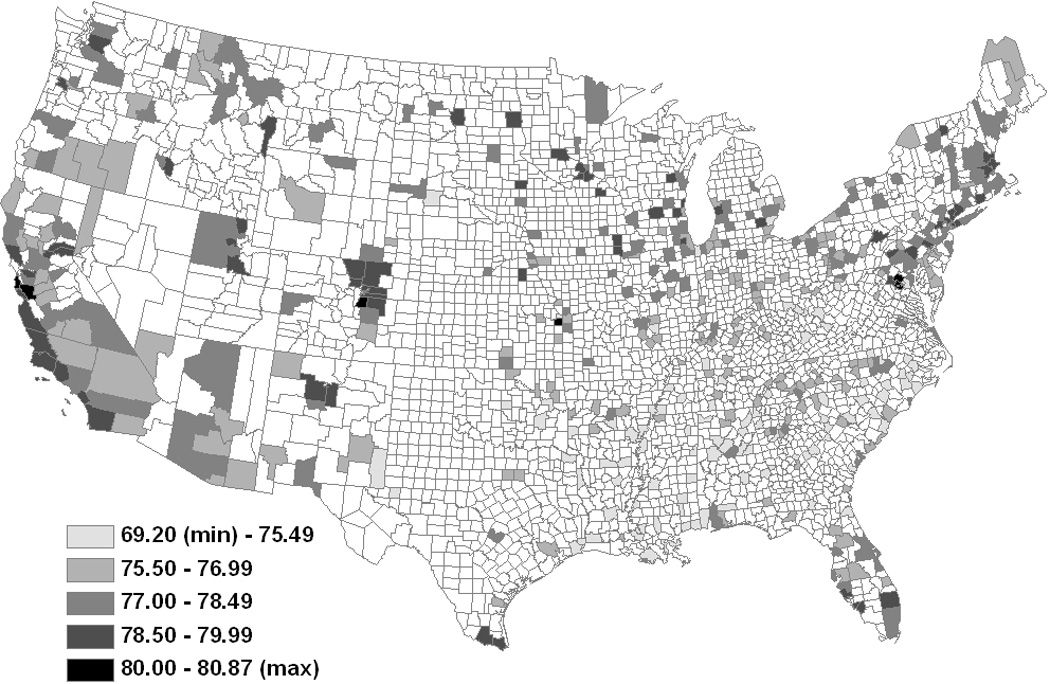
Map of U.S. with the 545 counties from Dataset 1 shaded according to year (A) 2000 and (B) year 2007 life expectancies.
County–level life expectancies were calculated by applying a mixed-effects spatial Poisson model to mortality data from the National Center for Health Statistics (NCHS) and population data from the U.S. Census to obtain robust estimates of the number of deaths in each county.30 These estimated counts were then used to calculate county life expectancies using standard life table techniques, which we discuss in more detail in the eAppendix (Section A).
Socioeconomic and demographic variables were obtained from the U.S. Census and the American Community Survey except per capita income, which was obtained from the Bureau of Economic Analysis. All yearly income variables were adjusted for inflation with 2000 as the base year. Age-standardized death rates for lung cancer and COPD were calculated using mortality data from NCHS using death rates for 2005 to serve as a proxy for 2007 (NCHS data for 2007 was not readily available). Lastly, data on smoking prevalence (proportion of the population who are current smokers) were available from the Behavioral Risk Factor Surveillance System in both 2000 and 2007 for 383 of the 545 counties.
Dataset 2 included data for the year 1980 and the year 2000 for the same 211 U.S. counties included in the 51 metropolitan statistical areas (MSAs) previously analyzed by Pope and colleagues.23 This dataset is identical to that in the paper by Pope et al,23 where it is described in more detail.
Dataset 3 extended Dataset 2 to 2007. All data were available at the county level except for PM2.5, which for the year 1980 was available only at the MSA level and for the year 2007 was available at the county level for only 113 of the 211 counties originally included in Pope et al.23 Thus, for the year 2007, we assigned the same PM2.5 values to all the counties that shared an MSA, consistent with the previous analysis.23 Details and results pertaining to Datasets 2 and 3 are summarized in the eAppendix (Section B1).
Statistical Analysis
Cross-sectional and first-difference linear regression models were fitted to all three datasets. Specifically, we regressed life expectancy versus PM2.5 levels across counties separately for the years 1980 (Dataset 2), 2000 (Datasets 1 and 2), and 2007 (Datasets 1 and 3). We then regressed changes in life expectancy over the years 2000 to 2007 (Datasets 1 and 3), 1980 to 2000 (Dataset 2), and 1980 to 2007 (Dataset 3) versus changes in PM2.5 over those same periods adjusted for changes in the socioeconomic, demographic, and proxy smoking variables outlined above. Additionally for our largest dataset (Dataset 1: 545 counties, 2000 to 2007), we also performed several stratified and weighted analyses. More specifically, we estimated the effect of changes in PM2.5 on life expectancy in models stratified by: 1) percentage of the population with an urban residence in 2000; 2) population density in 2000; 3), land area in 2000; 4) PM2.5 levels in 2000; 5) 5-year in-migration in 2000; and 6) change in average yearly temperature over the entire period. These stratified analyses allowed us to examine whether PM2.5 effects on life expectancy were different in counties with particular demographic or weather characteristics. The sensitivity of our results to model specification was further assessed by fitting models weighted by: 1) total population; 2) year 2000 population density; and 3) inverse land area. We included direct measures of the change in prevalence of smoking for the subgroup of counties with matching data on smoking prevalence (383 out of 545), and fit separate models for men and women to determine if effects differed by sex. To account for the correlation due to clustering of counties in the same MSA, robust clustered standard errors were calculated for all models.23,31 Specifically, the variance of the vector of estimated regression coefficients, βest, is given by: Var(βest) = (XTX)−1(XTVestX) (XTX)−1, where Vest is a block-diagonal matrix with non-zero blocks V0,j = (yj − μest,j)(yj − μest,j)T, where j indexes the MSAs. βest is equal to the ordinary least squares estimator. Models were estimated using either REGRESS in STATA version 11.0, lm() in R version 2.11.1, or PROC SURVEYREG in SAS version 9.2.
RESULTS
We report the results of our primary analysis, which estimated the cross-sectional relationship between life expectancy and PM2.5, and between changes in life expectancy and changes in PM2.5, for the period 2000 to 2007 in 545 US counties (Dataset 1). Results of the secondary analyses of the counties studied by Pope et al23 using Datasets 2 and 3 are in the eAppendix (Section B; eTables 1a,b and 2a,b). Table 1 lists the summary statistics for the variables in Dataset 1. In 2000, 189 of the 545 counties had a PM2.5 level greater than the current 3-year NAAQS level of 15µg/m3; by 2007 only 48 of those 189 were not in compliance with the NAAQS. On average, PM2.5 levels decreased at a rate of 0.22 µg/m3 per year, a rate 33% lower than observed in the 211 counties analyzed for the period 1980 to 2000 (0.33 µg/m3 per year).23
Table 1.
Summary Characteristics of the 545 Counties Analyzed for the years 2000 and 2007
| Variable | Mean (SD) |
|---|---|
| Life Expectancy (yr) | |
| 2000 | 76.7 (1.7) |
| 2007 | 77.5 (2.0) |
| Change | 0.8 (0.6) |
| PM2.5 (µg/m3) | |
| 2000 | 13.2 (3.4) |
| 2007 | 11.6 (2.8) |
| Reduction | 1.6 (1.5) |
| Per Capita Income (in thousands of $) | |
| 2000 | 27.9 (7.4) |
| 2007 | 30.4 (7.9) |
| Change | 2.5 (2.3) |
| Population (in hundreds of thousands) | |
| 2000 | 3.5 (6.3) |
| 2007 | 3.8 (6.6) |
| Change | 0.3 (0.6) |
| High School Graduates (prop of population) | |
| 2000 | 0.81 (0.07) |
| 2007 | 0.85 (0.06) |
| Change | 0.04 (0.02) |
| Black Population (prop of population) | |
| 2000 | 0.115 (0.138) |
| 2007 | 0.117 (0.139) |
| Change | 0.002 (0.017) |
| Hispanic Population (prop of population) | |
| 2000 | 0.119 (0.189) |
| 2007 | 0.098 (0.135) |
| Change | −0.021 (0.057) |
| Deaths from Lung Cancer (no./10,000 pop.)* | |
| 2000 | 16.4 (3.5) |
| 2007 | 15.5 (3.8) |
| Change | −0.9 (2.2) |
| Deaths from COPD (no./10,000 pop.)* | |
| 2000 | 12.8 (3.1) |
| 2007 | 12.5 (3.5) |
| Change | −0.3 (2.1) |
2005 death rates are used as a proxy for 2007 death rates. COPD denotes chronic obstructive pulmonary disease.
Figures 2A and 2B show life expectancies plotted against PM2.5 levels for the years 2000 and 2007. Consistent with Pope et al,23 cross-sectional regression models showed a negative association between life expectancy and PM2.5 in both years. Details are summarized in the eAppendix (Section C).
Figure 2.
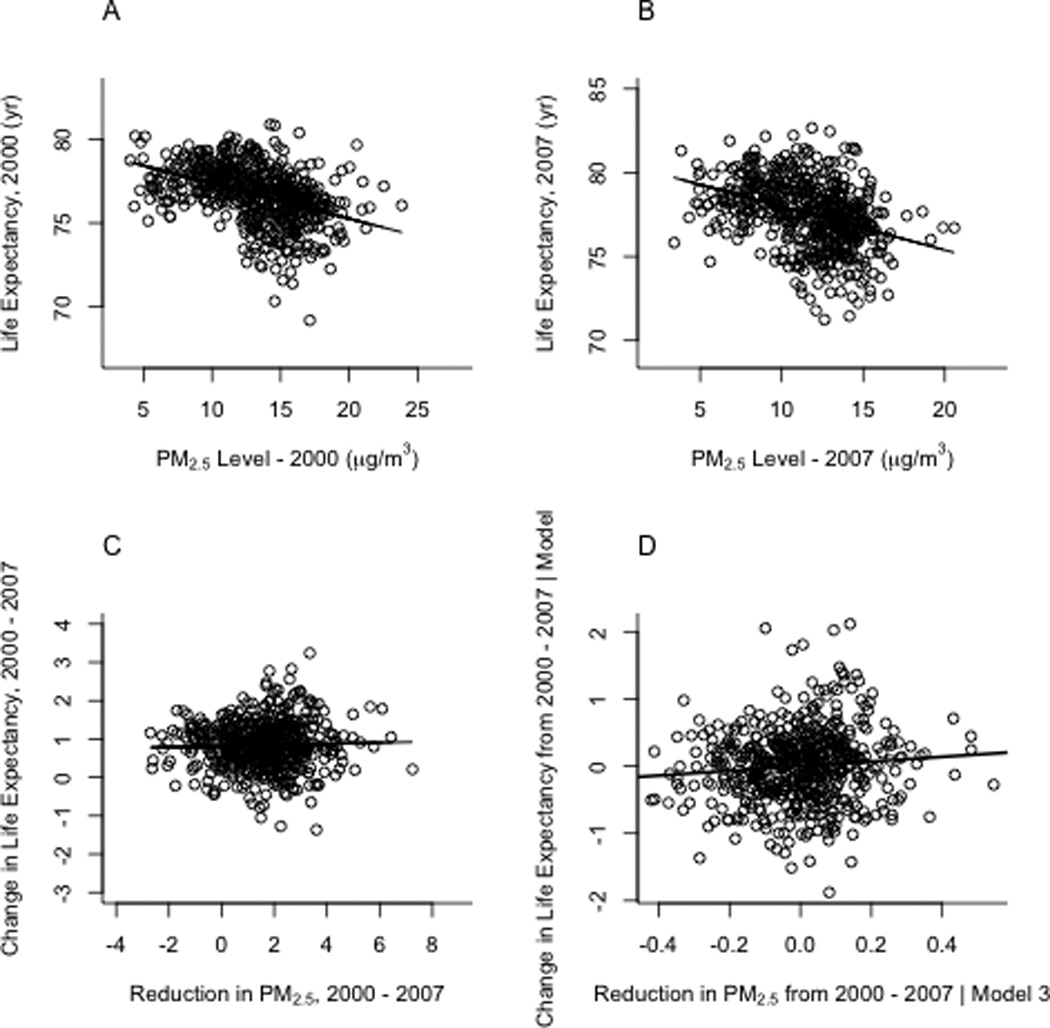
Cross-sectional life expectancies plotted vs PM2.5 levels for (A) 2000 and (B) 2007 in Dataset 1. The slopes of the regression lines correspond to estimates from the simple model: LE = intercept + slope*PM2.5 in both the 2000 and 2007 plots. (C) On the left the data are plotted as change in life expectancy vs change in PM2.5 over the period 2000 –2007. The regression line corresponds to the simple model ΔLE = intercept + slope*ΔPM2.5(Model 1 in Table 2). (C) On the right is the added variable plot for PM2.5 corresponding to Model 3 in Table 2.
Figures 2C and 2D show changes in life expectancy plotted against changes in PM2.5 levels for 2000 to 2007. We also plotted the estimated regression lines under Models 1 and 3 of Table 2, defined below.
Table 2.
Results of Selected Regression Models for County-level Analysis, 2000 to 2007. Regression coefficients (SE)
| Variable | Model 1 | Model 2 | Model 3 | Model 4 | Model 5a | Model 6b | Model 7c | Model 8 d | Model 9e |
|---|---|---|---|---|---|---|---|---|---|
| No. of county units | (n=545) | (n=545) | (n=545) | (n=545) | (n=257) | (n=307) | (n=169) | (n=545) | (n=545) |
| Intercept | 0.82 (0.04) | 1.08 (0.08) | 1.00 (0.08) | 1.03 (0.07) | 0.97 (0.10) | 0.91 (0.11) | 0.84 (0.15) | 0.79 (0.15) | 0.67 (0.15) |
| Reduction in PM2.5 (10µg/m3) | 0.14 (0.19) | 0.35 (0.17) | 0.35 (0.16) | 0.34 (0.16) | 0.30 (0.23) | 0.72 (0.22) | 0.95 (0.31) | 0.74 (0.24) | 0.96 (0.28) |
| Change in income (in thousands of $) | -- | 0.013 (0.017) | 0.017 (0.018) | -- | 0.005 (0.018) | 0.02 (0.02) | −0.01 (0.03) | 0.03 (0.02) | 0.05 (0.02) |
| Change in population (in hundreds of thousands) | -- | 0.13 (0.05) | 0.11 (0.05) | 0.11 (0.04) | 0.07 (0.05) | 0.06 (0.04) | 0.02 (0.04) | 0.07 (0.06) | 0.34 (0.12) |
| Change in high-school graduates (proportion of population) | -- | −9.12 (1.61) | −7.98 (1.56) | −7.83 (1.57) | −7.27 (1.95) | −4.42 (2.60) | 4.04 (3.20) | −1.94 (3.35) | −3.30 (3.45) |
| Change in black population (proportion of population) | -- | −6.55 (2.05) | −6.34 (1.97) | −6.43 (2.00) | −7.86 (3.07) | −9.02 (2.27) | −12.56 (3.59) | −11.14 (3.00) | −6.21 (2.97) |
| Change in Hispanic population (proportion of population) | -- | −2.16 (0.47) | −2.03 (0.47) | −2.13 (0.49) | −2.12 (0.59) | −2.46 (0.68) | −0.95 (0.62) | −3.25 (0.63) | −4.57 (0.75) |
| Change in lung cancer mortality rate (no./10,000 population) | -- | -- | −0.02 (0.02) | −0.02 (0.02) | −0.02 (0.02) | −0.05 (0.03) | −0.05 (0.05) | −0.07 (0.02) | −0.07 (0.03) |
| Change in COPD mortality rate (no./10,000 population) | -- | -- | −0.05 (0.01) | −0.05 (0.02) | −0.05 (0.02) | −0.06 (0.03) | −0.06 (0.05) | −0.08 (0.02) | −0.06 (0.02) |
Included only counties with the largest year 2000 population in the MSA.
Included only counties with a year 2000 population density > 200 ppl/sq. mile.
Included only counties with a year 2000 urban rate > 90%.
Weighted by the square root of the year 2000 population density.
Weighted by the inverse of county land area.
Table 2 summarizes estimated regression coefficients for the association between changes in PM2.5 and changes in life expectancy for 545 counties for 2000 to 2007 for selected regression models. When controlling for changes in all available socioeconomic and demographic variables as well as smoking prevalence proxy variables (Model 3), a 10 µg/m3 decrease in PM2.5 was associated with an estimated mean increase in life expectancy of 0.35 years (SE= 0.16 years, p = 0.033). The estimated effect of PM2.5 on life expectancy was consistent across models adjusting for various patterns of potentially confounding variables (e.g. Models 2 – 4). Models 5 – 9 of Table 2 show the results for select stratified and weighted regressions. In counties with a population density greater than 200 people per square mile, a 10 µg/m3 decrease in PM2.5 was associated with an increased life expectancy of 0.72 (0.22 years, p< 0.01) (Model 6), compared with −0.31 years (0.22 years, p = 0.165) in counties with less than 200 people per square mile (P difference <0.01). In counties whose proportion of urban residences was greater than 90 percent, a 10 µg/m3 decrease in PM2.5 was associated with an increased life expectancy of 0.95 (0.31, p< 0.01)(Model 7), compared with −0.16 (0.16 years, p = 0.299) in counties with less than 90% urban residences (P difference < 0.01).
When we re-estimated Model 3 of Table 2 using the square root of population density as the weight (Model 8), the estimated effect of a 10µg/m3 reduction of PM2.5 on life expectancy was more than double that observed in our un-weighted analysis (0.74 [0.24] vs. 0.35 [0.16]). When that same model was weighted by the inverse of county land area (Model 9), the effect was nearly triple that of the un-weighted analysis (0.96 [0.27]). Additional details regarding stratified and weighted analyses are provided in eTables 3 and 4 of the eAppendix.
We conducted similar analyses for the 211-county dataset for 1980 to 2007 and from 2000 to 2007, the results of which are presented in eTables 2a and 2b of the eAppendix, respectively. Results for the period from 1980 to 2000 were identical to those reported by Pope et al.23
Figure 3 summarizes the point estimate and 95% confidence interval for the effect of a 10 µg/m3 decrease in PM2.5 on life expectancy for a select un-weighted and un-stratified regression model in each dataset/time period. Models fitted using Datasets 2 and 3 (left) controlled for changes in income, population, proportion of the population that is black, lung cancer death rate, and COPD death rate, corresponding to Model 4 in eTables 2a,b. Models fitted using Dataset 1 controlled for all available variables and correspond to Model 3 in Table 2. These estimates were fairly consistent, though estimates corresponding to the counties from Pope et al23 for the period 2000 to 2007 appeared slightly larger than those from other analyses.
Figure 3.
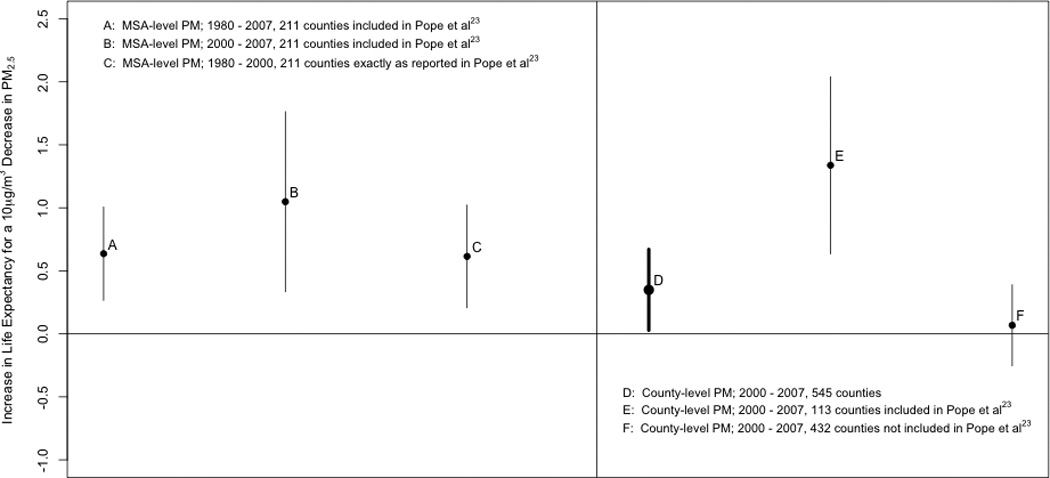
Point estimates (circles) and 95% confidence intervals (vertical lines) for the effect of a 10µg/m3 decrease in PM2.5 on life expectancy. Estimates A and B were obtained from Dataset 3; Estimate C was obtained from Dataset 2. Estimates A, B, and C were adjusted for changes in income, population, proportion of the population that is black, lung cancer death rate, and COPD death rate (Model 4, eTables 2a,b). Estimates D, E, and F were obtained from Dataset 1, adjusted for changes in income, population, proportion of high school graduates, proportion of the population that is black, proportion of the population that is Hispanic, lung cancer death rate, and COPD death rate (Model 3, Table 2).
In the analyses stratified by sex, the estimated effect of a 10µg/m3 reduction in PM2.5 for the covariate pattern corresponding to Model 3 of Table 2 was an additional 0.59 (0.17) years of life expectancy for women and 0.08 (0.20) years for men (P difference = 0.027). Differences by sex were also observed in stratified and weighted models, although with less precision. Sex differences were smaller in the most urban counties (urban rate > 90%). Similar results were observed for the period 1980 to 2000 in Dataset 2. (Sex-specific results are presented in eTable 5.)
Effect estimates were not highly sensitive to the inclusion of the estimated change in smoking prevalence. Table 3 summarizes the results for the inclusion/exclusion of the smoking prevalence variable across several models. For example, when Model 3 in Table 2 was re-estimated for the 383 counties with matching smoking prevalence data, a reduction of 10µg/m3 was associated with an increase in life expectancy of 0.49 (0.19) years without including change in smoking prevalence in the model, and 0.47 (0.19) when including those changes. Similar results for smoking were observed in our stratified and weighted models, as well as in our models for men and women separately.
Table 3.
Comparison of results of select models for inclusion of smoking variable vs. no inclusion of smoking variable
| Selected counties and analysis |
No. Counties |
Full model, with smoking β (SE, p) for 10 µg/m3 PM2.5 |
Full model, no smoking β (SE, p) for 10 µg/m3 PM2.5 |
|---|---|---|---|
| All Counties | 383 | 0.47(0.19, 0.013) | 0.49(0.19, 0.011) |
| 2000 population density (persons per square mile) | |||
| >800 | 110 | 0.52(0.43, 0.230) | 0.53(0.43, 0.221) |
| >600 | 139 | 0.68(0.30, 0.028) | 0.68(0.30, 0.027) |
| >400 | 187 | 0.71(0.26, 0.007) | 0.70(0.25, 0.007) |
| >200 | 272 | 0.67(0.22, 0.003) | 0.65(0.22, 0.004) |
| < 200 | 111 | −0.50(0.30, 0.100) | −0.39(0.30, 0.193) |
| 2000 urban rate | |||
| >90% | 157 | 0.76(0.28, 0.009) | 0.76(0.28, 0.008) |
| >95% | 101 | 1.01(0.31, 0.002) | 0.98(0.32, 0.003) |
| <90% | 226 | −0.14(0.20, 0.483) | −0.13(0.20, 0.513) |
| 2000 population density & 2000 urban rate | |||
| >200 & >90% | 100 | 0.95(0.32, 0.004) | 0.93(0.32, 0.005) |
| Regression weighted by square root of 2000 population density (All counties) | 383 | 0.77(0.24, 0.002) | 0.76(0.25, 0.003) |
| Regression weighted by inverse of county land area (All counties) | 383 | 0.81(0.26, 0.002) | 0.74(0.27, 0.007) |
| Sex | |||
| Men | 383 | 0.20(0.23, 0.389) | 0.22(0.23, 0.343) |
| Women | 383 | 0.71(0.20, 0.001) | 0.72(0.20, <0.001) |
Covariates include change in income, change in population, change in high-school graduates, change in proportion of black population, change in proportion of Hispanic population, change in lung cancer mortality rate, change in COPD mortality rate. Analysis used: SAS 9.2, PROC SURVEYREG, clustered by MSA, using the “weight” statement, and STATA 11.0, REGRESS.
DISCUSSION
Data on air pollution and life expectancy from 545 U.S. counties in 2000 and 2007 show that recent declines in PM2.5 to relatively low levels continue to prolong life expectancy in the US. These benefits are largest among the most urban and densely populated counties. These associations were estimated controlling for socioeconomic and demographic variables as well proxy variables for and direct measures of smoking prevalence.
In previous studies, a 10 µg/m3 decrease in PM2.5 has been associated with gains from 0.42 to 1.51 years of life expectancy.22,23 Here, a decrease of 10µg/m3 in PM2.5 was associated with an increase in life expectancy of 0.35 (0.16) for 545 counties for the period from 2000 to 2007. An increase in life expectancy of 0.56 (0.19) was estimated for the same 211 counties included in the Pope et al23 analysis but extended to the period 1980 to 2007. The estimated effect in those 211 counties from 2000 to 2007 was equal to 1.00 (0.32). Stratified and weighted analyses within the 545 counties from 2000 to 2007 yielded larger estimates between 0.72(0.22) and 1.12(0.32) – broadly in agreement with those previously reported.
From 2000 to 2007, the average increase in life expectancy across the counties in this study was 0.84 years, and the average decrease in PM2.5 in those same counties was 1.56µg/m3. While PM2.5 reductions presumably account for some of the improvements in life expectancy over this period, it is only one of many contributing factors. Other factors may include improvements in the prevention and control of the chronic diseases of adulthood, particularly cardiovascular diseases (CVD) and stroke,32,33 and changes in the risk factors associated with them, including medical advances, declines in smoking, and decreases in blood pressure and cholesterol.33 Given the well-established link between air pollution and CVD mortality,5,7–8 and changes in other CVD risk factors, issues of multicausality and competing risk make it difficult to quantify exactly the changes in life expectancy attributable to reductions in PM2.5. However, if we consider one of our more conservative effect estimates (Model 3, Table 2) the 1.56µg/m3 reduction in PM2.5 accounts for about 0.055 years (1.56×0.035) of additional life expectancy, or roughly 7% of the increase in life expectancy. Using the estimate from our most urban counties (Model 7, Table 2), the increase in life expectancy attributable to the average reduction in PM2.5 was 0.148 years (1.56×0.095), or as much as 18% of the total increase.
An interesting aspect of this study was how pronounced the PM2.5 effect was for the original 211 counties from 2000 to 2007. Given that they were originally selected simply on the availability of matching pollution data, what is special about these counties that results in larger estimates of the effect of PM2.5 on life expectancy? The stratified and weighted analyses suggest plausible explanations. For instance, the 211 counties were all in metropolitan areas, and the stratified analyses suggest that the effect of PM2.5 on life expectancy is greatest in the most urban counties. One possible reason is that the composition of PM2.5 is different in urban areas,34 causing PM2.5 to have a larger health impact. Another possibility is the “non-metropolitan mortality penalty” – the recent phenomenon in which mortality rates are higher in rural compared with urban areas.35 While it is not clear why the mortality gap between metro and non-metro areas has widened, some hypotheses include greater improvements in standards of care in metro areas, changes in uninsurance rates, changes in disease incidence, and changes in health behaviors.35 These, however, would be valid explanations only if they occurred at different rates in metropolitan areas compared with rural areas. If so, then perhaps failure to include variables that captured one or more of these differences could explain the different estimates of the effect of PM2.5 on life expectancy.
Alternatively, metropolitan areas are more densely populated than non-metro areas. Our models that stratified by population density showed that the effect of PM2.5 on life expectancy is greatest in the most densely populated study areas (those with a population density of at least 200 people per square mile)—possibly suggesting a role for differential exposure misclassification. That is, in densely populated areas, it is more likely that any two people from the same area are exposed to the same level of PM2.5 with perhaps less exposure misclassification. This possibility was supported in our models weighted by the square root of population density and the inverse of land area, which placed more weight on the most densely populated counties and the smallest counties. In these models the effect of a 10 µg/m3 decrease in PM2.5 on life expectancy was much larger than the equivalent un-weighted analysis.
Another interesting finding was the difference in the effect of changes in PM2.5 on men and women. Findings in the literature regarding the effects of air pollution by sex for long-term exposure have been mixed. Studies using the American Cancer Society and Harvard Six-Cities cohorts show no significant difference in pollution-related mortality between men and women.4–8,10 Studies using a Medicare cohort have reported different effects by age and region, but did not stratify by sex.28,36–37 In a study using the Adventist Health cohort, Chen et al38 reported a large effect of PM2.5 on fatal coronary heart disease (CHD) in women but no association in men. Similarly, in separate studies, Lipsett et al,39 using a cohort of women (California Teachers’ Study), reported associations between particulate matter and cardiovascular mortality, while Puett et al,40 using a cohort of men (Male Health Professionals), found no association with all-cause mortality or fatal CHD. For our main analysis using all 545 counties, we find a larger effect of PM2.5 on women, suggesting that reductions in PM2.5 are more beneficial to gains in life expectancy for women. Models fitted using data for the period from 1980 – 2000 as in Pope et al23 showed similar results. Future work should investigate more thoroughly the possibility of different PM2.5-mortality associations for men versus women.
One factor that appeared to play no role in the PM2.5 and life expectancy relationship, however, was baseline PM2.5 level. This is in agreement with the findings by Pope and colleagues,23 and implies that, while we may see differences across levels of population density, urban rate, and land area, this is not due to these areas having a higher or lower baseline PM2.5 level. Furthermore, this finding suggests that there is no clear threshold below which further reductions in PM2.5 levels provide no benefit (eAppendix, eTable 3). The fact that our results were not sensitive to the inclusion of direct measures of change in smoking prevalence suggests that the estimated gains in life expectancy for a 10µg/m3 reduction in PM2.5 are not a result of confounding due to changes in smoking prevalence.
Unlike previous cross-sectional analyses,16,17 we were able to estimate the association between county-specific temporal changes in PM2.5 levels and county-specific temporal changes on life expectancy adjusted by temporal changes in several potential confounding factors. By looking at within-county temporal changes, we reduce the potential bias due to unmeasured confounding. Further, by estimating clustered robust standard errors at the MSA level, we took a conservative approach in accounting for potential spatial correlation between neighboring counties.
Our analysis has the strengths of using some of the largest available datasets, and applying relatively simple analyses. Additionally, we improved on the original analysis by constructing a dataset with PM2.5 measured at the county level, in contrast to the more coarse MSA-level readings used in previous studies.7,23
The analysis is limited, however, in its ability to control for all potential unmeasured confounding. Additionally, in comparing selected years, we do not fully exploit potentially informative data between those years. Furthermore, sophisticated analyses of the U.S. Medicare population by Greven et al,36 did not observe associations between “local” trends in PM2.5 levels and “local” trends in mortality in 814 zip code level locations in the U.S. for the period 2000 – 2006. “Local” trends were defined as the difference between monitor-specific trends and national trends. The Medicare cohorts, however, consisted only of people age 65 and older, whereas our life expectancy calculations integrate over all ages. Also, other studies using Medicare based cohorts have found significant associations between PM2.5 and overall mortality.28,37 Future work is needed to investigate whether these differences among studies are due to differences in statistical models, data sources, or populations studied.
It is also worth considering whether life expectancy was the most appropriate outcome to consider in our model. Because life expectancies are calculated from age-specific mortality rates, perhaps a model with age-specific mortality rates as the outcome would be more appropriate, allowing the age groups most affected by PM2.5 exposure to be pinpointed precisely.
In summary, our study reports strong evidence of an association between recent further reductions in fine-particulate air pollution and improvements in life expectancy in the United States, especially in densely populated urban areas.
Supplementary Material
Acknowledgments
Sources of Funding:
Funding for all authors was provided by the U.S. Environmental Protection Agency (R-834894). Additional funding was provided by the U.S. EPA (RD-83479801), National Institutes of Health (ES019560 and ES012054), Harvard-NIEHS Center for Environmental Health (ES000002), NIEHS (T32ES007142), MRC Strategic Grant, and the Health Effects Institute.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Contributor Information
Andrew W. Correia, Department of Biostatistics, Harvard School of Public Health, 655 Huntington Avenue, HSPH Building 2, 4th Floor, Boston, MA 02115
C. Arden Pope, III, Department of Economics, Brigham Young University, 142 Faculty Office Building, Provo, UT 84602.
Douglas W. Dockery, Departments of Environmental Health and Epidemiology, Harvard School of Public Health, 655 Huntington Avenue, HSPH Building 1, 1301B, Boston, MA 02115
Yun Wang, Department of Biostatistics, Harvard School of Public Health, 655 Huntington Avenue, HSPH Building 2, 4th Floor, Boston, MA 02115.
Majid Ezzati, MRC-HPA Centre for Environment and Health and Department of Epidemiology and Biostatistics, Imperial College London, Norfolk Place, St Mary’s Campus, London W2 1PG.
Francesca Dominici, Department of Biostatistics, Harvard School of Public Health, 655 Huntington Avenue, HSPH Building 2, 4th Floor, Boston, MA 02115, fdominic@hsph.harvard.edu, P: (617) 432-1056; F: (617)-739-1781.
Bibliography
- 1.United States Environmental Protection Agency. The benefits and costs of the Clean Air Act, 1970 – 1990. 1997 Oct 15; [Google Scholar]
- 2.Pope P., III Mortality effects of longer term exposures to fine particulate air pollution: review of recent epidemiological evidence. Inhalation Toxicology. 2007;19:33–38. doi: 10.1080/08958370701492961. [DOI] [PubMed] [Google Scholar]
- 3.Schmidt M, Hassett-Sipple B, Rajan P. PM2.5 Air Quality Analyses – Memorandum to PM NAAQS Review. United States Environmental Protection Agency. 2010 Jul 22; [Google Scholar]
- 4.Dockery DW, Pope CA, III, Xu X, Spengler JD, Ware JH, Fay ME, et al. An association between air pollution and mortality in six U.S. cities. N Engl J Med. 1993;329:1753–1759. doi: 10.1056/NEJM199312093292401. [DOI] [PubMed] [Google Scholar]
- 5.Pope CA, III, Thun MJ, Namboodiri MM, Dockery DW, Evans JS, Speizer FE, et al. Particulate air pollution as a predictor of mortality in a prospective study of U.S. adults. Am J Respir Crit Care Med. 1995;151:669–674. doi: 10.1164/ajrccm/151.3_Pt_1.669. [DOI] [PubMed] [Google Scholar]
- 6.Krewski D, Burnett RT, Goldberg MS, Hovver K, Siemaitycki J, Jerrett M, et al. Reanalysis of the Harvard Six Cities Study and the American Cancer Society Study of particulate air pollution and mortality: special report. Cambridge, MA: Health Effects Institute; 2000. [DOI] [PubMed] [Google Scholar]
- 7.Pope CA, III, Burnett RT, Thun MJ, Calle EE, Krewski D, Ito K, et al. Lung cancer, cardiopulmonary mortality, and long-term exposure to fine particulate air pollution. JAMA. 2002;287:1132–1141. doi: 10.1001/jama.287.9.1132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Pope CA, III, Burnett RT, Thurston GD, Thun MJ, Calle EE, Krewski D, et al. Cardiovascular mortality and long-term exposure to particulate air pollution: epidemiological evidence of general pathophysiological pathways of disease. Ciculation. 2004;109:71–77. doi: 10.1161/01.CIR.0000108927.80044.7F. [DOI] [PubMed] [Google Scholar]
- 9.Jerrett M, Burnett RT, Ma R, Pope CA, III, Krewski D, Newbold KB, et al. Spatial analysis of air pollution and mortality in Los Angeles. Epidemiology. 2005;16:727–736. doi: 10.1097/01.ede.0000181630.15826.7d. [DOI] [PubMed] [Google Scholar]
- 10.Laden F, Schwartz J, Speizer FE, Dockery DW. Reduction in fine particulate air pollution and mortality: Extended follow-up of the Harvard Six Cities study. Am J Respir Crit Care Med. 2006;173:667–672. doi: 10.1164/rccm.200503-443OC. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Krewski D, Burnett R, Goldberg M, et al. Reanalysis of the harvard six cities study, part I: validation and replication. Inhalation Toxicology. 2005;17:335–342. doi: 10.1080/08958370590929402. [DOI] [PubMed] [Google Scholar]
- 12.Krewski D, Burnett R, Goldberg M, et al. Reanalysis of the harvard six cities study, part II: sensitivity analysis. Inhalation Toxicology. 2005;17:343–353. doi: 10.1080/08958370590929439. [DOI] [PubMed] [Google Scholar]
- 13.Burnett R, Ma R, Jerrett M, et al. The spatial association between community air pollution and mortality: a new method of analyzing correlated geographic cohort data. Environmental Health Perspectives. 2001;109(suppl 3):375–380. doi: 10.1289/ehp.01109s3375. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Samet JS, Dominici F, Curriero FC, Coursac I, Zeger SL. Fine particulate air pollution and mortality in 20 U.S. cities, 1987 – 1994. NEJM. 2000;343(24):1742–1749. doi: 10.1056/NEJM200012143432401. [DOI] [PubMed] [Google Scholar]
- 15.Schwartz J, Coull B, Laden F, Ryan L. The effect of dose and timing of dose on the association between airborne particles and survival. Environmental Health Perspectives. 2008;116(1):64–69. doi: 10.1289/ehp.9955. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Evans J, Tosteson T, Kinney P. Cross-sectional mortality studies and air pollution risk assessment. Environmental International. 1984;10(1):55–83. [Google Scholar]
- 17.Özkaynak H, Thurston G. Associations between 1980 U.S. mortality rates and alternative measures of airborne particle concentration. Risk Analysis. 1987;7:449–461. doi: 10.1111/j.1539-6924.1987.tb00482.x. [DOI] [PubMed] [Google Scholar]
- 18.Pope CA, III, Dockery D. Health effects of fine particulate air pollution: lines that connect. Journal of the air & waste management association. 2006;56(6):709–742. doi: 10.1080/10473289.2006.10464485. [DOI] [PubMed] [Google Scholar]
- 19.Schwartz J. Particulate air pollution and daily mortality in Detroit. Environmental Research. 1991;56:204–213. doi: 10.1016/s0013-9351(05)80009-x. [DOI] [PubMed] [Google Scholar]
- 20.Schwartz J. Particulate air pollution and daily mortality in Steubenville, Ohio. American Journal of Epidemiology. 1992;135:12–19. doi: 10.1093/oxfordjournals.aje.a116195. [DOI] [PubMed] [Google Scholar]
- 21.Dominici F, McDermott A, Zeger SL. Airborne particulate matter and mortality: timescale effects in four U.S. cities. American Journal of Epidemiology. 2003;157:1055–1065. doi: 10.1093/aje/kwg087. [DOI] [PubMed] [Google Scholar]
- 22.Tainio M, Tuomisto J, Hänninen J, et al. Parameter and model uncertainty in a life-table model for fine particles (PM2.5): a statistical modeling study. Environmental Health. 2007;6:24. doi: 10.1186/1476-069X-6-24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Pope CA, III, Ezzati M, Dockery D. Fine-particulate air pollution and life expectancy in the United States. New England Journal of Medicine. 2009;360(4):376–386. doi: 10.1056/NEJMsa0805646. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Brunekreef B. Air pollution and life expectancy: is there a relation? Occupational and Environmental Medicine. 1997;54:781–784. doi: 10.1136/oem.54.11.781. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.McMichael A, Henderson H, Brunekreef B, Cohen A. Inappropriate use of daily mortality analyses to estimate longer-term mortality effects of air pollution. International Journal of Epidemiology. 1998;27:450–453. doi: 10.1093/ije/27.3.450. [DOI] [PubMed] [Google Scholar]
- 26.Rabl A. Interpretation of air pollution mortality: number of deaths or years of life lost? Journal of the Air and Waste Management Association. 2003;53(1):41–50. doi: 10.1080/10473289.2003.10466118. [DOI] [PubMed] [Google Scholar]
- 27.Peto R, Lopez AD, Boreham J, et al. Mortality from tobacco in developed countries: indirect estimation from national vital statistics. Lancet. 1992;339:1268–1278. doi: 10.1016/0140-6736(92)91600-d. [DOI] [PubMed] [Google Scholar]
- 28.Eftim SE, Samet JM, Janes H, et al. Fine particulate matter and mortality: a comparison of the Six Cities and American Cancer Society cohorts with a Medicare cohort. Epidemiology. 2008;19:209–216. doi: 10.1097/EDE.0b013e3181632c09. [DOI] [PubMed] [Google Scholar]
- 29.Peng RD, Dominici F. Statistical methods for environmental epidemiology in R: a case study in air pollution and health. Springer; 2008. [Google Scholar]
- 30.Kulkarni S, Lavin-Rector A, Ezzati M, Murray CJ. Falling behind: life expectancy in U.S. counties from 2000 to 2007 in an international context. Population Health Metrics. 2011;9:16. doi: 10.1186/1478-7954-9-16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Diggle P, Liang K, Zeger SL. Analysis of longitudinal data. Oxford: Clarendon Press; 1994. [Google Scholar]
- 32.Yeh RW, Normand SL, Wang Y, Barr CD, Dominici F. Geographic disparities in the incidence and outcomes of hospitalized myocardial infarction: Does a rising tide lift all boats? Circ Cardiovasc Qual Outcomes. 2012;5:197–204. doi: 10.1161/CIRCOUTCOMES.111.962456. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Shrestha LB. Life expectancy in the United States. CRS Report for Congress. 2005 [Google Scholar]
- 34.Louie PK, Chow JC, Chen LW, et al. PM2.5 chemical composition in Hong Kong: urban and regional variations. Science of the Total Environment. 2005;338(3):267–281. doi: 10.1016/j.scitotenv.2004.07.021. [DOI] [PubMed] [Google Scholar]
- 35.Cossman JS, James WL, Cosby AG, Cossman RE. Underlying causes of the emerging nonmetropolitan mortality penalty. American Journal of Public Health. 2010;100(8):1417–1419. doi: 10.2105/AJPH.2009.174185. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Greven S, Dominici F, Zeger SL. An approach to the estimation of chronic air pollution effects using spatio-temporal information. Journal of the American Statistical Association. 2011;106(494):396–406. doi: 10.1198/jasa.2011.ap09392. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Zeger SL, Dominici F, McDermott A, Samet J. Mortality in the Medicare population and chronic exposure to fine particulate air pollution in urban centers (2000 – 2005) Environmental Health Perspectives. 2008;116(12):1614–1618. doi: 10.1289/ehp.11449. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Chen LH, Knutsen SF, Shavlik D, et al. The association between fatal coronary heart disease and ambient particulate air pollution: Are females at greater risk? Environmental Health Perspectives. 2005;113(12):1723–1729. doi: 10.1289/ehp.8190. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Lipsett MJ, Ostro BD, Reynolds P, et al. Long-term exposure to air pollution and cardiorespiratory disease in the California Teachers Study cohort. Am J Respir Crit Care Med. 2011;184(7):828–835. doi: 10.1164/rccm.201012-2082OC. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Puett RC, Hart JE, Suh H, Mittleman M, Laden F. Particulate matter exposures, mortality, and cardiovascular disease in the health professionals follow-up study. Environmental Health Perspectives. 2011;119(8):1130–1135. doi: 10.1289/ehp.1002921. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.