

Abstract
Rhabdomyosarcoma is a soft tissue malignant musculoskeletal tumor. It is a rare tumor in children but the most common cause of malignant obstructive jaundice in them. A 4-year-old child presented to us with obstructive jaundice and palpable liver. He was misdiagnosed as choledochal cyst on imaging studies; however, intraoperative and histopathological features confirmed the diagnosis of rhabdomyosarcoma. Mass excision and Roux en Y portoenterostomy was performed. Post operatively; the patient was put on multimodal chemotherapy. This, being an uncommon entity, is being reported with a review of the available literature.
Keywords: Biliary rhabdomyosarcoma, Choledochal cyst, Rhabdomyosarcoma in choledochal cyst
Introduction
Rhabdomyosarcoma (RMS), a soft tissue malignant musculoskeletal tumor, is a rare lesion in children, accounting for about 1 % of all malignancies [1]. Hepatobiliary RMS is a disease affecting young children at a median age of about 3 years. It is a rare tumor; however, it is the most common cause of obstructive jaundice due to neoplastic biliary obstruction in children [2].
We treated a case of RMS of the extrahepatic biliary tree, which was initially diagnosed to be a choledochal cyst. Being an extremely uncommon entity, it is being presented with a review of the available literature.
Case Report
A 4-year-old boy presented to the Department of Pediatric Surgery of the University Hospital with complaint of off and on right upper abdominal pain and jaundice, along with passage of clay coloured stool. On examination, icterus was present. The liver was palpable 2 cm below the right subcostal margin. There was no splenomegaly, ascites, skin rashes, or cervical lymphadenopathy.
The liver function tests showed raised parameters (SGOT and SGPT 124 and 107 IU/L, alkaline phosphate 3331.7 IU/L, total and direct bilirubin 11.8 and 6.6 mg%). Hepatitis B antigen was negative. Ultrasonography (USG) of the abdomen showed dilated common bile duct (CBD), and intrahepatic biliary channels were dilated. Computerized tomography (CT) scan showed fusiform dilation of CBD (4.5 cm × 2.3 cm). The right and left hepatic ducts and intarhepatic biliary radical were dilated with gradual tapering to periphery, suggestive of type 1 choledocal cyst.
Intraoperatively, there was no evidence of choledocal cyst, and the lump appeared to be a biliary RMS. Instead of a cyst, it was a firm mass. The tumor was carefully dissected from the portal vein and the hepatic artery. Before ensuring complete excision, 6Fr endoscope was introduced into the right and left hepatic ducts to ensure disease free margins. Excision of the involved CBD, along with gall bladder was performed. The continuity was restored by a Roux en Y portoenterostomy (Fig. 1a, b, c). There was no evidence of metastasis or lymph node involvement. The histopathology was suggestive of botryoid RMS (Figs. 2 and 3). Post operatively; the patient was put on Vincristin, Adriamycin and Cyclophosphamide (VAC) chemotherapy, however, after first cycle; the patient did not come in follow up for one and half month. When patient returned he had evidence of jaundice. On USG, there was a mass at the porta, which appeared to be the recurrence. Considering this, the chemotherapy was changed to Ifosphamide and Etoposide, alternating with VAC. Following this chemotherapy, jaundice relieved and USG revealed decrease in the size of the mass at porta by 50 %. Till now, 9 months have passed. If the mass at porta will show evidence of increase, radiotherapy will be added to the treatment protocol.
Fig. 1.

a Intraoperative picture showing the mass after a nick is made into it. b Roux-en-Y porto-enterostomy being performed. c Excised mass. The thread is tied towards the distal end
Fig. 2.
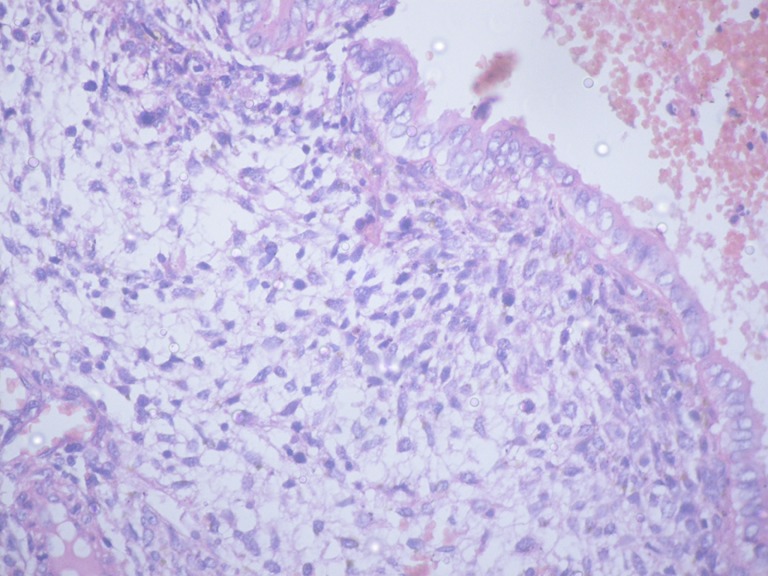
Microphotograph showing cambium layer below the mucosal surface strongly undifferentiated hyperchromatic malignant cells. (H & E stain ×200)
Fig. 3.
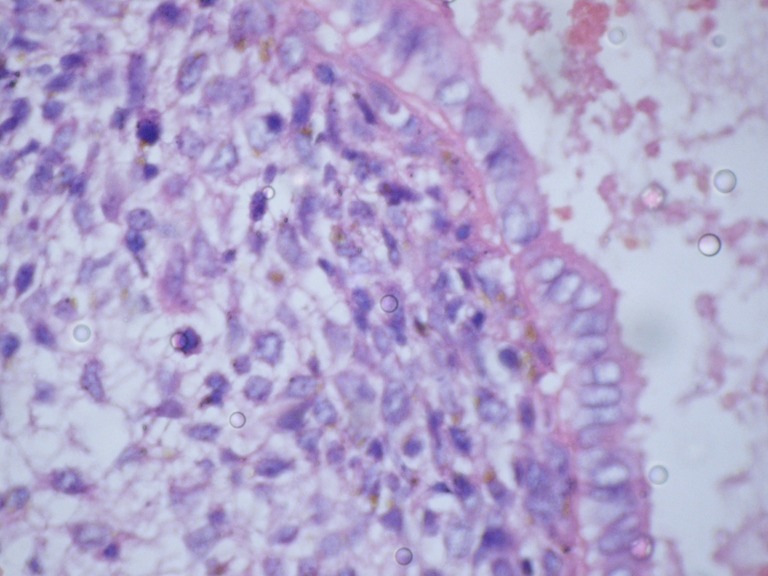
Higher malignification showing its pleomorphic undifferentiated malignant cells. (H & E stain ×400)
Discussion
RMS is a malignant tumour arising from skeletal muscle. The common sites seen in children and infants are head and neck, genitourinary tract, and retroperitoneum [3]. Tumours of the extra hepatic biliary tract are rare in childhood but they are the most common cause of malignant obstructive jaundice in children [2].
Biliary RMS is difficult to diagnose. It is a very rare disease with about 50 cases described in the literature, the largest series involving 25 patients over a period of 25 years [4]. It commonly presents with features of obstructive jaundice, which is seen as a presenting symptom in 60–80 % of cases, and may be accompanied by acholic stools and hepatomegaly [5]. In our case also, obstructive jaundice with hepatomegaly was the presenting feature. Pain, nausea and vomiting, and fever may also be noticed but they are not common [6].
It has been noted that unlike RMS at other sites, where alveolar or undifferentiated histology may be present, the biliary tract contains tumors of only embryonal or botryoid histology [4].
Imaging studies frequently misdiagnose it as choledochal cyst as noticed in our patient. However, it is suggested that for proper staging and planning of the management of the patient, both USG and CT scan may be needed [4]. There are certain reports where RMS was present within the choledochal cyst [7]. CT scan, by identifying the solid nature of the tumor, may help in differentiating it from choledochal cyst; however, it is not always possible, as seen in our patient. It can also help in staging the disease. Intraoperative finding of soft white tissue bits also correlates well with the gross features described for RMS. Immunohistochemical analysis is very useful in the diagnosis of embryonal RMS. More than 95 % of these tumors are positive for desmin [8]. In addition, nuclear staining with myogenin, a gene product that induces skeletal muscle differentiation, is useful in the diagnosis because of its specificity for RMS [8].
Current modalities of treatment include surgical removal, radiation, and chemotherapy [9]. Various workers have advocated aggressive surgical intervention in a belief that reduction of tumor bulk affects the outcome [4]. However, there are reports indicating very good response either to chemo and radiotherapy, or delayed surgery after chemotherapy. Gross total excision is not always possible. Despite this, probably due the presence of favorable histology, the prognosis is relatively good [4].
Based on the literature review and the outcome of our patient, the following treatment protocol may be adopted [4, 5, 10, 11]-
If the mass is resectable, complete excision, followed by chemotherapy.
If there is residual disease, positive lymph nodes or relapse, chemo and radiotherapy, followed by second look surgery. The chemotherapy may include addition of ifosfamide and etoposide to the VAC regime.
If there is extensive disease, neoadjuvant chemotherapy with or without radiotherapy, followed by second look surgery, if the mass decreases. In case of biliary obstruction, stenting may be performed.
To conclude, RMS should be considered in the differential diagnosis of any child presenting with features of obstructive jaundice and suspicion of choledochal cyst. Advances in surgery, radiotherapy, and chemotherapy have improved the prognosis and long-term survival.
References
- 1.Enzinger FM, Weiss SW. Rhabdomyosarcoma. In: Enzinger FM, Weiss SW, editors. Soft tissue tumors. 34. St Louis, Mo: Mosby; 2001. p. 790. [Google Scholar]
- 2.Ali S, Russo MA, Margraf L. Biliary rhabdomyoscarcoma mimicking choledochal cyst. J Gastrointestin Liver Dis. 2009;18:95–97. [PubMed] [Google Scholar]
- 3.Baker KS, Anderson JR, Link MP, Holcombe EG, Qualman SJ, Maurer HM, et al. Benefit of intensified therapy for patients with local or regional embryonal rhabdomyosarcoma: Results from the intergroup rhabdomyosarcoma study IV. J Clin Oncol. 2000;18:2427–2434. doi: 10.1200/JCO.2000.18.12.2427. [DOI] [PubMed] [Google Scholar]
- 4.Sanz N, Mingo L, Florez F, Rollan VV. Rhabdomyosarcoma of the biliary tree. Pediatr Surg Int. 1997;12:200–201. doi: 10.1007/BF01350002. [DOI] [PubMed] [Google Scholar]
- 5.Nemade B, Talapatra K, Shet T, Banavali S, Muckaden M, Laskar S. Embryonal rhabdomyosarcoma of the biliary tree mimicking a choledochal cyst. J Can Res Ther. 2007;3:40–42. doi: 10.4103/0973-1482.31971. [DOI] [PubMed] [Google Scholar]
- 6.Spunt SL, Lobe TE, Pappo AS, Parham DM, Wharam MD, Jr, Arndt C, et al. Aggressive surgery unwarranted for biliary tract Rhabdomyosarcoma. J Pediatr Surg. 2000;35:309–316. doi: 10.1016/S0022-3468(00)90030-7. [DOI] [PubMed] [Google Scholar]
- 7.Patil KK, Omojola MF, Khurana P, Iyengar JK. Embryonal rhabdomyosarcoma within a choledochal cyst. Can Assoc Radiol J. 1992;43:145–148. [PubMed] [Google Scholar]
- 8.Morotti RA, Nicol KK, Parham DM, et al. An immunohistochemical algorithm to facilitate diagnosis and subtyping of rhabdomyosarcoma: the Children’s Oncology Group experience. Am J Surg Pathol. 2006;30:962–968. doi: 10.1097/00000478-200608000-00005. [DOI] [PubMed] [Google Scholar]
- 9.Breneman J, Anderson J, Donaldson S, et al. Prognostic factors and outcome in childrens with metastatic rhbdomyosarcoma —a report from Intergroup Rhabdomyosarcoma Study IV. Int J Rad Oncol Biology Physics. 2001;51(Suppl.1):A 210. [Google Scholar]
- 10.Akers DR, Needham ME. Sarcoma botryoides (rhabdomyosarcoma) of the bile ducts with survival. J Pediatr Surg. 1971;6:474–479. doi: 10.1016/S0022-3468(71)80011-8. [DOI] [PubMed] [Google Scholar]
- 11.Davis GL, Kissane JM, Ishaz KG. Embryonal rhabdomyosarcoma (sarcoma botryoides) of the biliary tree. Report of five cases and a review of the literature. Cancer. 1969;24:333–342. doi: 10.1002/1097-0142(196908)24:2<333::AID-CNCR2820240216>3.0.CO;2-G. [DOI] [PubMed] [Google Scholar]