

The prevention of postoperative liver failure after extended hepatectomy often requires preoperative intervention to induce hypertrophy in the future liver remnant. Portal vein embolization (PVE) is the most commonly used intervention, but 4–6 weeks are required to induce significant hypertrophy in the remnant liver.1 Hepatic vein embolization can provide further hypertrophy over 2–3 weeks if PVE is inadequate.2 Two-stage hepatectomy with the use of PVE or portal vein ligation is an alternative strategy with which to address the challenge of residual liver volume.3 In a recent German multicentre study, Schnitzbauer and colleagues used a modification of the two-stage hepatectomy, designated the ‘associated liver partition with portal vein ligation staged hepatectomy’ (ALPPS).4 This procedure requires liver parenchymal transection just to the right of the umbilical fissure with simultaneous right portal vein ligation during the first stage of the operation, followed about a week later by completion right trisectionectomy. The ALPPS procedure resulted in a median increase in volume of the left lateral segment of 74% within 9 days with necrosis of segment IV (Fig. 1), but was associated with postoperative bile leak in five and death in three of 25 patients.4 The precise role and value of ALPPS are yet to be determined.
Figure 1.
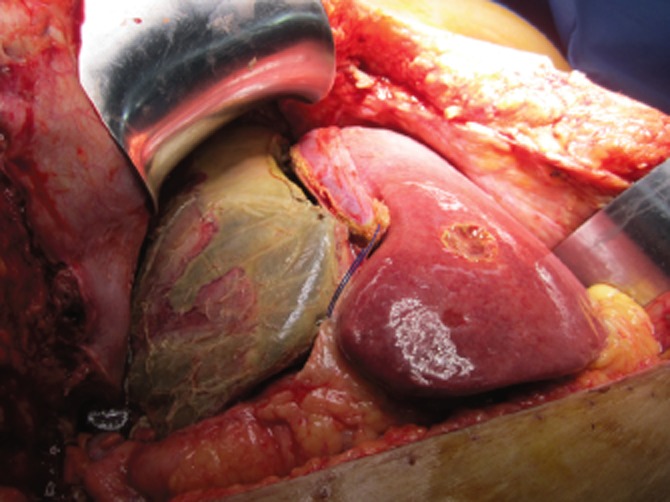
Operative photograph demonstrating massive hypertrophy of the left lateral segment and necrosis of segment IV at 8 days after stage 1 of the associated liver partition with portal vein ligation staged hepatectomy (ALPPS) procedure
References
- 1.Abulkhir A, Limongelli P, Healey AJ, Damrah O, Tait P, Jackson J, et al. Preoperative portal vein embolization for major liver resection: a meta-analysis. Ann Surg. 2008;247:49–57. doi: 10.1097/SLA.0b013e31815f6e5b. [DOI] [PubMed] [Google Scholar]
- 2.Hwang S, Lee SG, Ko GY, Kim BS, Sung KB, Kim MH, et al. Sequential preoperative ipsilateral hepatic vein embolization after portal vein embolization to induce further liver regeneration in patients with hepatobiliary malignancy. Ann Surg. 2009;249:608–616. doi: 10.1097/SLA.0b013e31819ecc5c. [DOI] [PubMed] [Google Scholar]
- 3.Jaeck D, Oussoultzoglou E, Rosso E, Greget M, Weber JC, Bachellier P. A two-stage hepatectomy procedure combined with portal vein embolization to achieve curative resection for initially unresectable multiple and bilobar colorectal liver metastases. Ann Surg. 2004;240:1037–1051. doi: 10.1097/01.sla.0000145965.86383.89. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Schnitzbauer A, Lang SA, Goessmann H, Nadalin S, Baumgart J, Farkas SA, et al. Right portal vein ligation combined with in situ splitting induces rapid left lateral liver lobe hypertrophy enabling two-staged extended right hepatic resection in small-for-size settings. Ann Surg. 2012;255:405–414. doi: 10.1097/SLA.0b013e31824856f5. [DOI] [PubMed] [Google Scholar]