

Abstract
Poor counter traction and poor field of vision make endoscopic submucosal dissection (ESD) difficult. Good counter traction allows dissections to be performed more quickly and safely. Position change, which utilizes gravity, is the simplest method to create a clear field of vision. It is useful especially for esophageal and colon ESD. The second easiest method is clip with line method. Counter traction made by clip with line accomplishes the creation of a clear field of vision and suitable counter traction thereby making ESD more efficient and safe. The author published this method in 2002. The name ESD was not established in those days; the name cutting endoscopic mucosal resection (EMR) or EMR with hook knife was used. The other traction methods such as external grasping forceps, internal traction, double channel scope, and double scopes method are introduced in this paper. A good strategy for creating counter traction makes ESD easier.
Keywords: Endoscopic submucosal dissection, Stomach neoplasms, Counterattraction, Surgical instruments
INTRODUCTION
There are some important factors that make endoscopic submucosal dissection (ESD) difficult such as the size of the tumor, fibrosis, bleeding, etc. However, the main factors that make ESD difficult are absence of counter traction and poor field of vision. Good counter traction allows for safe and speedy dissection. The key points to maintaining a good field of vision and counter traction are described in this paper.
POSITION CHANGE
The simplest method to get counter traction is position change. If the location of a lesion is situated so that gravity does not aid in the removal of blood and water, good counter traction cannot be obtained, and sometimes water and blood will interfere with the surgeon's field of vision. However, if the lesion is positioned to use gravity to keep the field of vision clear of blood and water the surgeon will have a clear field of vision. Additionally, gravity can be used to pull the mucosa which gives the surgeon adequate counter traction and further assists in creating a clear field of vision. Therefore, the patient should be positioned to make effective use of gravity during ESD.
Clip with sinker method increases the effects of gravity.1 A clip with sinker was attached to a target site at the edge of the exfoliated mucosa after circumferential mucosal incision. Then the weight of the sinker pulled down the partly resected mucosa allowing for good counter traction.
CLIP WITH LINE METHOD
If you can pull the target lesion, good counter traction can be made. The authors reported clip with line method in 2002.2 Figs. 1, 2 are reprints from the paper by permission of the publisher. It is a simple and useful method to make counter traction during ESD. A long, 3-0, silk line was tied to the arm part of the clip (HX-610-135; Olympus, Tokyo, Japan) (Fig. 3). Then the clip with line is reset in the cassette (Fig. 4).
Fig. 1.
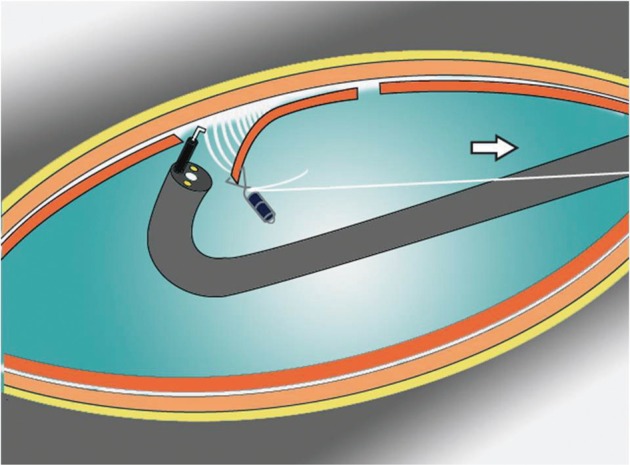
An illustration showing clip with line method. A clip with line was placed at the edge of the target lesion when the circumferential incision was completed. Good counter traction and a clear field of vision were obtained when the line was pulled very gently (reprinted from Oyama T, et al. Stomach Intest 2002;37:1155-1161, with permission).2
Fig. 2.
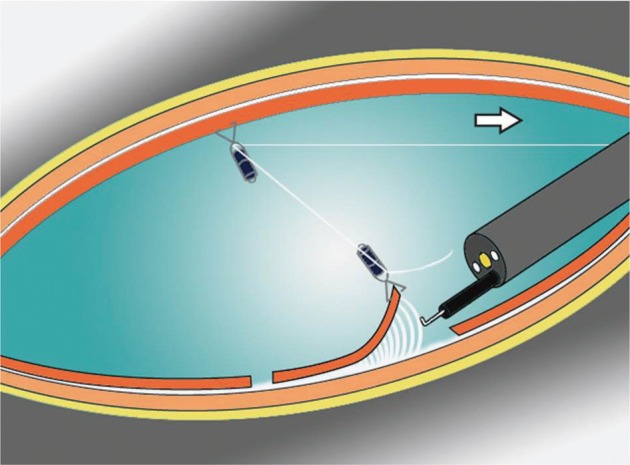
The second clip can change the direction of traction (reprinted from Oyama T, et al. Stomach Intest 2002;37:1155-1161, with permission).2
Fig. 3.
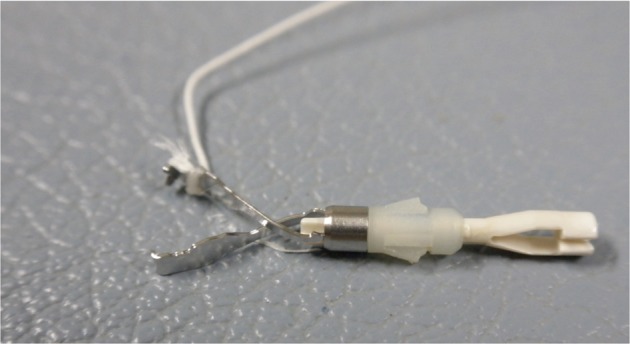
A long, 3-0, silk line was tied to the arm part of the clip.
Fig. 4.
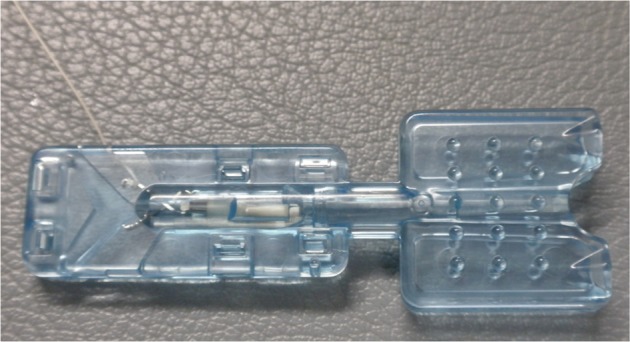
The clip with line is reset in the cassette. Then the clip with line can be set in the applicator like a usual clip.
The scope is withdrawn when the circumferential incision is finished (Figs. 5, 6). A clip applicator device (HX-110QR; Olympus) is inserted into the accessory channel of the endoscope, and the clip with line is mounted onto the tip of the applicator. Then the clip was drawn into the applicator device, and the applicator device is also drawn into the transparent hood for insertion into the endoscope.
Fig. 5.
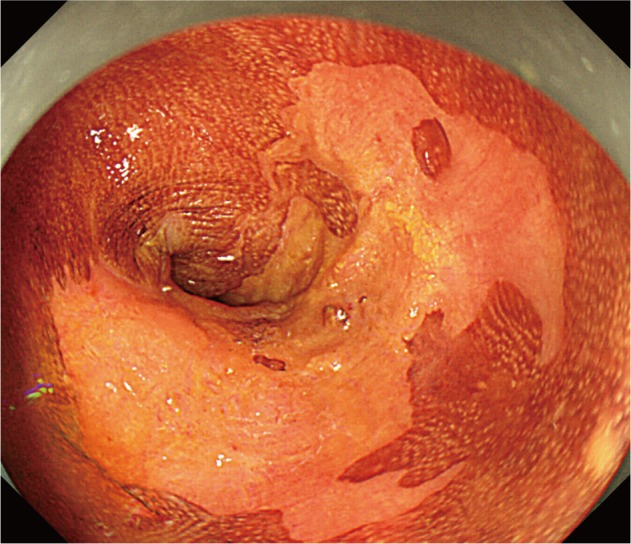
Endoscopy showed a well demarcated semicircumferential iodine unstaind lesion in the lower esophagus.
Fig. 6.
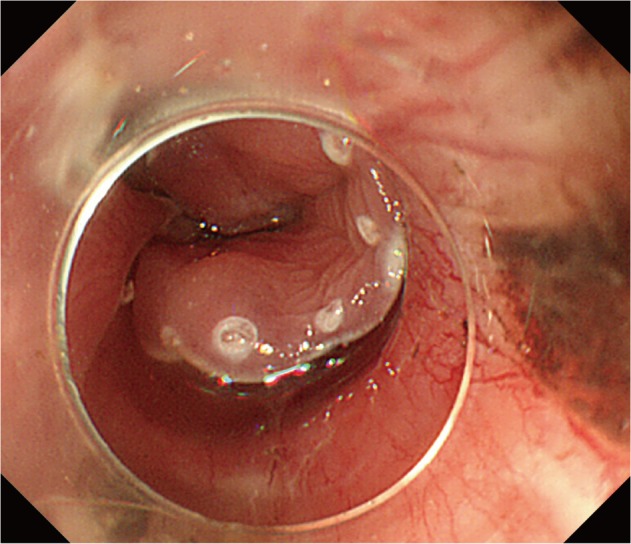
The circumferential incision was completed. The next step is submucosal dissection. However, the field of vision was not clear enough because the submucosal space is narrow.
The scope is inserted again, and the submucosal side of the target lesion is grasped (Fig. 7). After that the line is pulled very gently. Only a small amount of tension is required to create counter traction. This method also creates a clear field of vision (Figs. 8, 9). During submucosal dissection, tension is maintained with a 10-g sinker such as mouth piece. The 10-g sinker creates sufficient counter traction and tension without threatening to tear the submucosal layer.
Fig. 7.
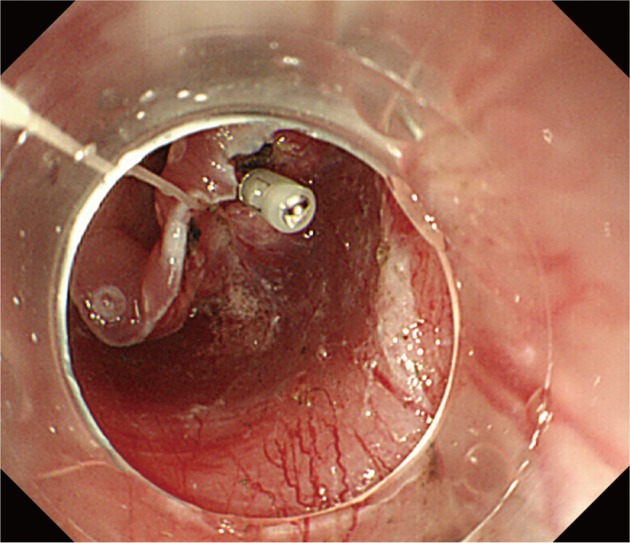
The clip with line was placed at the submucosal side of the targeted specimen.
Fig. 8.
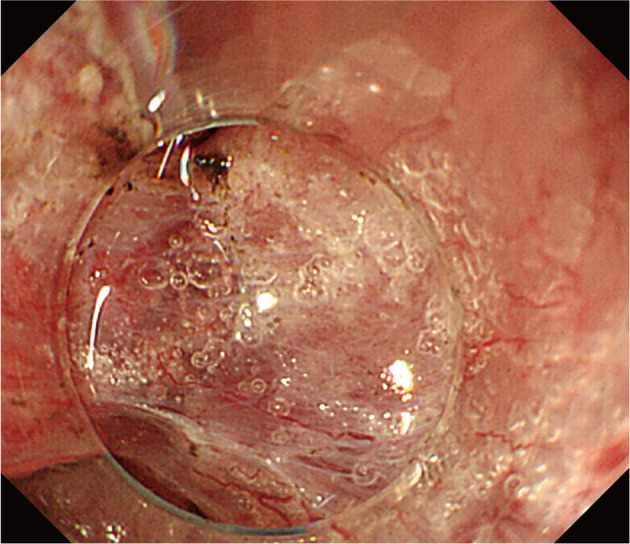
A clear field of vision and adequate counter traction were gained when the line was pulled gently.
Fig. 9.

Procedure after traction. (A, B) The movement of specimen could be stopped by the traction made by the line. Submucosal dissection was then performed more easily, safely, and quickly.
If you want to pull the line to anal side, the pulley method is useful (Fig. 2). A second clip is inserted and opened just before the line. The line was captured by the second clip and fixed at the opposite side of the stomach. Then, the first clip could be pulled to the anal side with the second clip acting like a pulley. Recently, similar ideas have been reported from Asian endoscopists.3-5
The clip with line method is a simple and useful method not only for gastric ESD, but also for esophageal, colonic, and duodenal ESD.6 It is especially useful for esophageal and gastric ESD when the cancer exists in the greater curvature of the gastric body.
EXTERNAL GRASPING FORCEPS METHOD
The external grasping forceps are captured by the other grasping forceps inserted into the working channel. The external grasping forceps are inserted with the help of the other grasping forceps after the circumferential mucosal resection. After the external grasping forceps are anchored at the margin of the lesion and the second grasping forceps are released. The distance from the tip of the endoscope to the dissected site can be adjusted by not only pulling but also by pushing the grasping forceps. Then good counter traction can be made.7,8 Great care was taken to avoid injuring the mucosa, especially at the esophagocardial junction.
INTERNAL TRACTION METHOD
Some methods to make internal traction have been reported. It is different from the clip with line method, in that a set of two clips connected by a rubber ring or nylon line was used. The first clip with rubber ring or nylon line was attached at the target part after circumferential mucosal incision.9,10 After that, the second clip was attached at the opposite sides of the lesion. This pulls up the lesion and opens up the resection margin. This makes submucosal dissection easier. It is a simple and easy method, but the control of the traction power is sometimes difficult.
DOUBLE CHANNEL SCOPE METHOD
A grasping forceps inserted into a channel of a double-channel scope can make counter traction during ESD.11,12 An outer sheath of an injection needle is also useful to make counter traction.13 The bottom of the dissected mucosal layer was pushed and lifted up using the injection sheath to reveal the submucosal layer and to ensure adequate counter traction of the cutting lines.
The advantage of this method is that it requires only a conventional grasping forceps or injection sheath. The disadvantage of double channel scope method is thicker size and long radius of curvature. Additionally, it is sometimes difficult to insert it into submucosal layer, and maneuverability is poorer than a thin therapeutic scope during ESD.
DOUBLE SCOPE METHOD
Some methods using a second endoscopy have been reported.14-17 The direction of traction could be controlled easily with the double scope method. However, the second scope sometimes disturbs the maneuverability of the main scope. Therefore, a thin scope is recommended for the second scope.
CONCLUSIONS
The key point to make ESD safer and faster is creating a clear field of vision. A transparent hood is necessary to maintain visualization during ESD. A strategy to maintain a clear field of vision is also necessary for safe ESD. There are some methods that create adequate counter traction. Position change and clip with line method are the simplest and easiest methods.
Footnotes
The author has no financial conflicts of interest.
References
- 1.Saito Y, Emura F, Matsuda T, et al. A new sinker-assisted endoscopic submucosal dissection for colorectal cancer. Gastrointest Endosc. 2005;62:297–301. doi: 10.1016/s0016-5107(05)00546-8. [DOI] [PubMed] [Google Scholar]
- 2.Oyama T, Kikuchi Y, Shimaya S, et al. Endoscopic mucosal resection using a hooking knife (hooking EMR) Stomach Intest. 2002;37:1155–1161. [Google Scholar]
- 3.Jeon WJ, You IY, Chae HB, Park SM, Youn SJ. A new technique for gastric endoscopic submucosal dissection: peroral traction-assisted endoscopic submucosal dissection. Gastrointest Endosc. 2009;69:29–33. doi: 10.1016/j.gie.2008.03.1126. [DOI] [PubMed] [Google Scholar]
- 4.Li CH, Chen PJ, Chu HC, et al. Endoscopic submucosal dissection with the pulley method for early-stage gastric cancer (with video) Gastrointest Endosc. 2011;73:163–167. doi: 10.1016/j.gie.2010.08.041. [DOI] [PubMed] [Google Scholar]
- 5.Okamoto K, Muguruma N, Kitamura S, Kimura T, Takayama T. Endoscopic submucosal dissection for large colorectal tumors using a cross-counter technique and a novel large-diameter balloon overtube. Dig Endosc. 2012;24(Suppl 1):96–99. doi: 10.1111/j.1443-1661.2012.01264.x. [DOI] [PubMed] [Google Scholar]
- 6.Oyama T. Endoscopic submucosal dissection using a hook knife. Tech Gastrointest Endosc. 2011;13:70–73. [Google Scholar]
- 7.Imaeda H, Iwao Y, Ogata H, et al. A new technique for endoscopic submucosal dissection for early gastric cancer using an external grasping forceps. Endoscopy. 2006;38:1007–1010. doi: 10.1055/s-2006-925264. [DOI] [PubMed] [Google Scholar]
- 8.Imaeda H, Hosoe N, Ida Y, et al. Novel technique of endoscopic submucosal dissection using an external grasping forceps for superficial gastric neoplasia. Dig Endosc. 2009;21:122–127. doi: 10.1111/j.1443-1661.2009.00842.x. [DOI] [PubMed] [Google Scholar]
- 9.Imaeda H, Hosoe N, Ida Y, et al. Novel technique of endoscopic submucosal dissection by using external forceps for early rectal cancer (with videos) Gastrointest Endosc. 2012;75:1253–1257. doi: 10.1016/j.gie.2012.02.018. [DOI] [PubMed] [Google Scholar]
- 10.Matsumoto K, Nagahara A, Sakamoto N, et al. A new traction device for facilitating endoscopic submucosal dissection (ESD) for early gastric cancer: the "medical ring". Endoscopy. 2011;43(Suppl 2 UCTN):E67–E68. doi: 10.1055/s-0030-1255923. [DOI] [PubMed] [Google Scholar]
- 11.Chen PJ, Chu HC, Chang WK, Hsieh TY, Chao YC. Endoscopic submucosal dissection with internal traction for early gastric cancer (with video) Gastrointest Endosc. 2008;67:128–132. doi: 10.1016/j.gie.2007.07.021. [DOI] [PubMed] [Google Scholar]
- 12.Neuhaus H, Costamagna G, Deviere J, et al. Endoscopic submucosal dissection (ESD) of early neoplastic gastric lesions using a new double-channel endoscope (the "R-scope") Endoscopy. 2006;38:1016–1023. doi: 10.1055/s-2006-944830. [DOI] [PubMed] [Google Scholar]
- 13.Yonezawa J, Kaise M, Sumiyama K, Goda K, Arakawa H, Tajiri H. A novel double-channel therapeutic endoscope ("R-scope") facilitates endoscopic submucosal dissection of superficial gastric neoplasms. Endoscopy. 2006;38:1011–1015. doi: 10.1055/s-2006-944779. [DOI] [PubMed] [Google Scholar]
- 14.Hijikata Y, Ogasawara N, Sasaki M, et al. Endoscopic submucosal dissection with sheath-assisted counter traction for early gastric cancers. Dig Endosc. 2010;22:124–128. doi: 10.1111/j.1443-1661.2010.00948.x. [DOI] [PubMed] [Google Scholar]
- 15.Uraoka T, Kato J, Ishikawa S, et al. Thin endoscope-assisted endoscopic submucosal dissection for large colorectal tumors (with videos) Gastrointest Endosc. 2007;66:836–839. doi: 10.1016/j.gie.2007.04.028. [DOI] [PubMed] [Google Scholar]
- 16.Uraoka T, Ishikawa S, Kato J, et al. Advantages of using thin endoscope-assisted endoscopic submucosal dissection technique for large colorectal tumors. Dig Endosc. 2010;22:186–191. doi: 10.1111/j.1443-1661.2010.00992.x. [DOI] [PubMed] [Google Scholar]
- 17.Ahn JY, Choi KD, Choi JY, et al. Transnasal endoscope-assisted endoscopic submucosal dissection for gastric adenoma and early gastric cancer in the pyloric area: a case series. Endoscopy. 2011;43:233–235. doi: 10.1055/s-0030-1256037. [DOI] [PubMed] [Google Scholar]