

Abstract
BACKGROUND/AIM:
Laparoscopic excision of a choledochal cyst (CC) with hepaticojejunostomy gained a wide acceptance in the treatment of children even in neonatal period. Although, the use of prenatal diagnostic techniques causes a significant increase in antenatal diagnosis of CC, the time of surgical intervention during infancy is still controversial. A retrospective study was performed to evaluate the results of laparoscopic management of CC with special emphasis on antenatal diagnosis and treatment, and to compare the results with open procedure.
MATERIALS AND METHODS:
The patients who were diagnosed with choledochal cyst and underwent either open or laparoscopic hepaticojejunostomy in two centres, hopital d’enfant de La Timone from Marseille and hopital Robert Debre from Paris between November 2000 and December 2009 were included in the study. The data obtained from medical reports were evaluated for sex, time of antenatal diagnosis, age at time of operation, operative time, time of postoperation.
RESULTS:
A total of 19 hepaticojejunostomy were performed, including 10 open procedures (group A), and 9 laparoscopic procedures (group B, 4 were diagnosed prenatally, without conversion to open procedure). There were 3 boys and 16 girls, ranging in age from 2 weeks to 16 years. Patients in the group A were older than patients in the group B. The mean hospital stay and time to return of bowel fuction was longer in the group B. there were 60% of pre-operative complications in group A versus 22% in group B. There was one postoperative complications in group B (biliary leakage nedeed redo surgery). No significant differences were found between different parameters except for operative time (288.56 min in the group B versus 206 min in the group A. (p = 0.041)).
CONCLUSIONS:
Our initial experience indicates that the laparoscopic approach in infancy is technically feasible, safe, and effective, with a low morbidity and a comparable outcome to the open approach. Therefore, we propose a laparoscopic approach for antenatally diagnosed CC as early as possible, before the onset of complications.
Keywords: Choledochal cyst, laparoscopy, antenatal, resection
INTRODUCTION
The advance and wide spread use of prenatal diagnosis leads prompt diagnosis of choledochal cyst (CC) even as early as 15 weeks of gestation.[1] However, the optimal strategy of management, especially regarding the best timing of intervention, has not been established. The technical difficulty of hepaticojejunostomy and the occurrence of postoperative complications in neonatal period are still challenging.[2]
Total excision of cyst with Roux-en-Y hepaticoenterostomy is the treatment of choice of CC in both adults and children. The first laparoscopic treatment of CC was introduced by Farello et al, in children.[3] Subsequently, many reports confirm that laparoscopic approach is also feasible and safe in children with long operative time and technique difficulties. Although the feasibility of laparoscopic resection of CC in early infancy is still unclear and needs further evaluation, these preliminary results force us to revise the policy of surgical treatment timing in CC. Therefore, we perform a retrospective study to evaluate the results of laparoscopic treatment of CC with a special emphasis on antenatal diagnosis and treatment and to compare results with open procedure.
MATERIALS AND METHODS
Materials
The patients who were diagnosed as choledocal cyst and underwent either open or laparoscopic hepaticojejunostomy in two centres, hopital d’enfant de La Timone from Marseille and hopital Robert Debre from Paris between November 2000 and December 2009 were included in the study. The data obtained from medical reports were evaluated for sex, time of antenatal diagnosis, age at time of operation, operative time (incision to dressing), time of postoperative bowel recovery (first bowel movement), length of hospital stay, pre and postoperative complications and follow up retrospectively. The results of patients who underwent laparoscopic approach were compared with the ones who had open surgery.
Statistical Analysis
The data obtained from medical reports were analysed with SPSS 15.0 using Mann- Whitney U and Fisher's test. Probability value less than 0.05 were considered to be significant.
Operative Procedures
Open surgical approach
The patients who underwent open surgery had a right extended subcostal incision with or without an operative cholangiography. The complete excision of CC with creation of Roux-en-Y hepaticojejunostomy was the choice of treatment in this group.
Laparoscopic approach
A five-port technique was used as laparoscopic approach. Under general anaesthesia, a vertical umbilical incision was performed for a 5-10 mm (according to the age of the patient) 30° laparoscope and carbon dioxide pneumoperitoneum was obtained at the pressure of 7-9 mmHg. Four additional ports were placed under direct laparoscopic visualization. A 5 mm port at the left 11th intercostal space was used for gripping the diaphragm. Two 3-5 mm ports were placed either side and slightly above the umbilicus and a 5 mm port was inserted at the left lower quadrant below the umbilicus. Operative cholangiography was performed in all patients. The umbilical incision was extended to 1.5 or 2 cm to exteriorize the jejunum. After identifying the ligament of Treitz laparoscopically, the proximal jejunum 40 cm distal to the ligament was captured and exteriorized through umbilical trocar. Roux-en-Y jejunojejunostomy with one-layer interrupted sutures was carried out manually. The closed jejunum limb was lifted through a mesocolon incision at the right side. The CC were completely resected by using the laparoscopic ultrasonic coagulating shears and the monopolar Hook to the normal-appearing common hepatic duct proximally and to near the pancreatic duct distally. The hepaticojejunostomy was created using interrupted 5-0 polygloctin suture. The laparoscopic procedure was completed with hepatic biopsy in some of the cases.
RESULTS
The total number of 19 patients who underwent either open (n:10) or laparoscopic (n:9) hepaticojejunostomy for CC was included in the study. The mean age of the patients at the time of operation was 62.5 months (range: min: 12 and max: 192 months) and 53.7 months (range min: 12 days and max: 156 months) in open and laparoscopic approach groups, respectively (P > 0.05). The male female ratio was 3:7 in open approach group and 1:8 in laparoscopic group. Four patients were diagnosed antenatally with the guidance of both prenatal USG and MRI. Figure 1 illustrates the antenatal MRI diagnosis of a patient with CC. One patient who diagnosed antenatally was underwent open procedure where other three had laparoscopic intervention. The mean age of antenatal diagnosis was 23 weeks of gestation (range: 22-24 weeks). The demographic and clinical features of patients with antenatal diagnosis are summarized in Table 1. Among the patients with antenatal diagnosis, one patient had progressive cholestasis and underwent open surgery. At the time of this case, laparoscopic approach was not the initial treatment option for CC in our department. MR-choloangiopancreography (MRCP) was used for the diagnosis of CC in patients without antenatal diagnosis. According to Todani's description, patients were classified as type I (n: 17) and type 4 (n: 2) CC.[4] The common pancreaticobiliary duct was noted in 7 patients. The mean diameter of the cysts was found 25, 26 mm (range: 12 - 80 mm). Postnatal MRCP was also confirmed the diagnosis of CC in patients with antenatal diagnosis.
Figure 1.
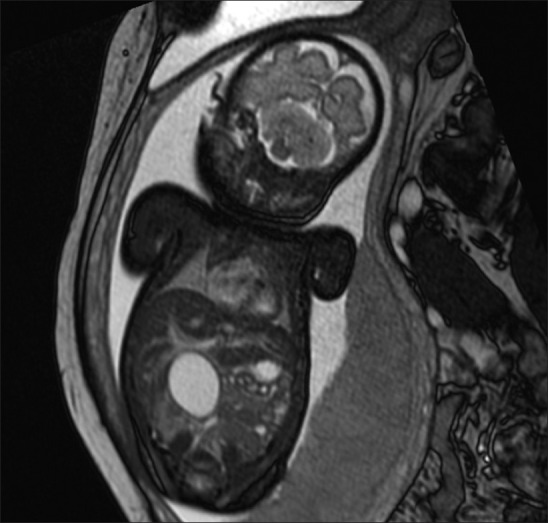
Antenatal MRI diagnosis of a patient with choledochal cyst
Table 1.
Demographic and clinical features of patients with antenatal diagnosis

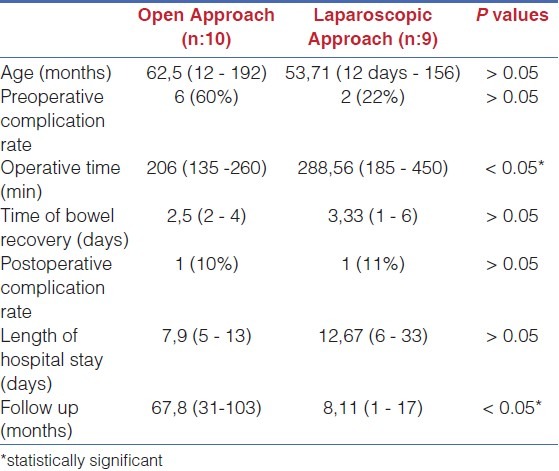
The clinical features and outcome of the surgical treatment in patients with open and laparoscopic surgery is listed in Table 2. Cholangitis, cholestasis and pancreatitis are assessed as the preoperative complications of CC. Preoperative complications were noted in 6 patients with open surgery (60%) and 2 patients (22%) in laparoscopic procedure group (P > 0.05). One patient in open surgery group had hepatic artery injury peroperatively. Conversion to an open surgery did not need in any laparoscopic procedure. The postoperative complications of the hepaticojejunostomy were bile leakage and pancreatitis. Bile leakage was seen in one patient who underwent laparoscopic excision. The patient with bile leakage required another laparoscopic intervention. Pancreatitis was occurred in one patient after open surgery. No statistical difference was detected between groups for postoperative complications (P > 0.05). When mean hospital stay, operative time, postoperative bowel recovery time and follow up are compared between open and laparoscopic approach groups, statistical difference was detected in mean operative time and follow up periods [Table 3]. The mean operative time was found significantly higher in laparoscopic approach group (288.56 minutes) when compared to open surgery group (206 minutes) (P < 0.05, Mann Whitney U test). The follow up period was also shorter in laparoscopy group (8. 11 months, range: 1- 17 months) than open surgery group (67,80 months, range 31-103 months) (P < 0.05, Mann Whitney U test).
Table 2.
Description of the patients
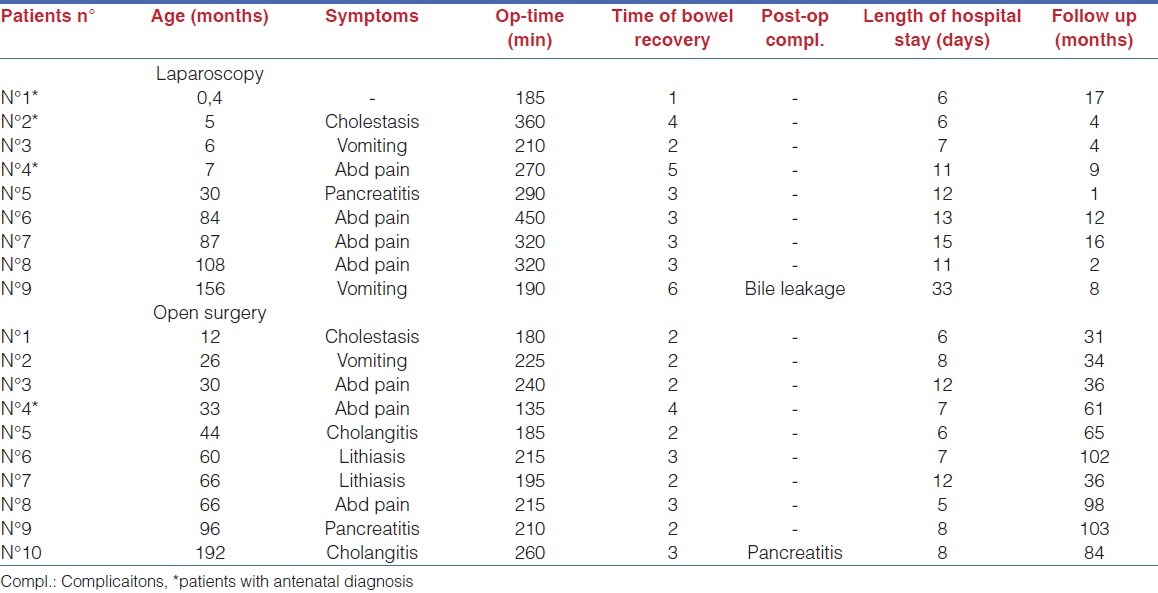
Table 3.
Comparison of open and laparoscopic approach for parameters
DISCUSSION
In our study, we found more preoperative complications in the group operated by laparotomy, even if the statistical test is not significant. Moreover, we found similar results when comparing complications and postoperative recovery. The long-term follow up is shorter in the laparoscopic group, as patients have been operated recently. It remains to demonstrate that long-term results in patients managed laparoscopically are as good, if not better, as those managed by conventional approach, by decreasing bowel adhesions rate.
Complete excision of cysts and hepaticojejunostomy is the optimal definitive procedure for CC.[5] Laparoscopic approach to a CC was firstly described by Farelo et al, in a 6 years old child.[6] Since then, several authors[3,4,7–15] highlighted the advantages of laparoscopic surgery in CC such as magnified view, ease of identification and dissection of critical structures, particularly, in the main bile duct.[16] They also emphasized the technical challenge of the hepaticojejunostomy as the most difficult and time consuming step. The overall results of these data suggest that laparoscopic approach in the treatment of CC is feasible and safe with limited complications.
The widespread use of antenatal US lead to increase in frequency of early diagnosis. However, the appropriate age of surgery has become debated. Some authors favor neonatal treatment of CC because of having prompt differential diagnosis of type I biliary atresia and avoiding the complications of CC such as cholesthasis and biliary chirosis. About half of the patients with antenatally diagnosed CC are asymptomatic at birth.[10] Since most of the patients have stenosis distal to the cyst, clinical symptoms such as recurrent jaundice, liver dysfunction, ascending cholangitis, pancreatitis and rupture of the cyst are usually seen. Biliary cirrhosis and portal hypertension are the most common long term complications if CC was left untreated. When we consider the nature of disease and the advances in laparoscopic surgery and antenatal diagnosis, we need to revise our policy of treatment in CC. In our series, even we have four patients with antenatal diagnosis; one of them has experienced preoperative complications. And no one of the patients had postoperative complication. Therefore, we suggest that surgical treatment of CC with antenatal diagnosis should be performed as early as possible.
By the means of early surgery some authors perform either open or laparoscopic approach during neonatal period. It has been thought that neonatal surgery on a thin-walled choledochal cyst can be technically difficult and may lead to further anastomotic complications such as bile leakage or stricture.[9,17] However, it has been proposed as safe and effective by others.[2,11–14] We have only one patient who underwent laparoscopic approach in the 12 days of her life. Though, the operative time (185 minutes), the length of hospital stay (6 days) and time to bowel recovery (1 day) of that patient was favorable. Although, neonatal laparoscopic surgery for CC is thought to be technically difficult and has potential risks (Liu), we suggest that it is as safe as open surgery and has favorable outcomes after adequate experience have been achieved in laparoscopic CC excision.
Not only the results but also the technique of Roux-en-Y anastomosis under laparoscopy has been a matter of discussion. Although, some authors suggested using an EndoGIA, it is not feasible in children.[15] Le et al performed jejuno-jejunostomy intracorporeally and found that fully laparoscopic approach is exceedingly challenging and time consuming. Therefore, exteriorization of small bowel from the umbilcal trocar incision is commonly used to perform an extrabdominal Roux-en-Y anastomosis.
In a largest series of laparoscopic CC resections, it has been postulated that laparoscopic surgery provides excellent visualization, less blood loss and short duration of hospital stay. The rate of bile leakage and wound infection did not show any difference. However, duration of laparoscopic surgery is significantly longer. Le et al[3] demonstrated a relatively short operative time and hospital stay compared to the literature. In our series, we found similar results with the literature for operative time. In addition, preoperative and postoperative complication rates, time to bowel recovery did not show significant difference between two groups. The mean follow up period of our patients in laparoscopy group is shorter than open surgery group, because of the changed policy of management in CC. Most of our patients were operated by conventional approach before 2005. Since then, laparoscopic surgery become the initial choice of treatment. The complications of surgery for CC consist of bile leakage, anastomotic failure, cholangitis, pancreatitis, adhesive bowel obstruction and wound infection. It has been reported that adhesive intestinal obstruction rate after cyst excision is up to 4%.[15] Moreover, type of surgical intervention, either open or laparoscopic approach, has not shown differences in bowel adhesion rate after surgery.[11] Since, we have small number of patients; it is not possible for us to have a conclusion about the complications rate after laparoscopic surgery. Larger series of patients with long follow up are needed to evaluate decreasing risk of bowel adhesions after laparoscopic approach.
In conclusion, surgical treatment of CC antenatally diagnosed, either with open or laparoscopic approach, should be performed as early as possible to avoid preoperative complications. Although there is a risk of complications and technical difficulties, neonatal intervention should be also performed before the case become symptomatic. According to our results, we can suggest that midterm results of laparoscopic surgery in children for CC are similar to conventional open surgery. Long follow up is necessary to determine the advantage of laparoscopic approach in long term, especially in decreasing the number of bowel adhesions.
ACKNOWLEDGEMENT
This study will be presented at the 10th Congress of European Pediatric Surgeons Association (EUPSA) in 2-6 June, 2010, Bern, Switzerland.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Ohtsuka Y, Yoshida H, Matsunaga T, Kouchi K, Okada T, Ohnuma N. Strategy of management for congenital biliary dilatation in early infancy. J Pediatr Surg. 2002;37:1173–6. doi: 10.1053/jpsu.2002.34466. [DOI] [PubMed] [Google Scholar]
- 2.Okada T, Sasaki F, Ueki S, Hirokata G, Okuyama K, Cho K, et al. Postnatal management for prenatally diagnosed choledochal cysts. J Pediatr Surg. 2004;39:1055–8. doi: 10.1016/j.jpedsurg.2004.03.054. [DOI] [PubMed] [Google Scholar]
- 3.Le DM, Woo RK, Sylvester K, Krummel TM, Albanese CT. Laparoscopic resection of type 1 choledochal cysts in pediatric patients. Surg Endosc. 2006;20:249–51. doi: 10.1007/s00464-005-0151-4. [DOI] [PubMed] [Google Scholar]
- 4.Todani T, Watanabe T, Narusue Y, Tabuchi K, Okajima K. Congenital bile duct cysts: Classification, operative procedures, and review of thirty-seven cases including cancer arising from choledochal cyst. Am J Surg. 1977;134:263–9. doi: 10.1016/0002-9610(77)90359-2. [DOI] [PubMed] [Google Scholar]
- 5.Chowbey PK, Katrak MP, Sharma A, Khullar R, Soni V, Baijal M, et al. Complete laparoscopic management of choledochal cyst: Report of two cases. J Laparoendosc Adv Surg Tech A. 2002;12:217–21. doi: 10.1089/10926420260188146. [DOI] [PubMed] [Google Scholar]
- 6.Farello GA, Cerofolini A, Rebonato M, Bergamaschi G, Ferrari C, Chiappetta A. Congenital Choledochal cyst: Video-guided laparoscopic treatment. Surg Laparosc Endosc. 1995;5:354–8. [PubMed] [Google Scholar]
- 7.Dewbury KC, Alwihare AP, Birch SJ, Freeman NV. Case reports: Prenatal ultrasound demonstration of a Choledochal cyst. Br J Radiol. 1980;53:906–7. doi: 10.1259/0007-1285-53-633-906. [DOI] [PubMed] [Google Scholar]
- 8.Mackenzie TC, Howell LJ, Flake AW, Adzick NS. The management of prenatally diagnosed choledochal cysts. J Pediatr Surg. 2001;36:1241–3. doi: 10.1053/jpsu.2001.25784. [DOI] [PubMed] [Google Scholar]
- 9.Redkar R, Davenport M, Howard ER. Antenatal diagnosis of congenital anomalies of the biliary tract. J Pediatr Surg. 1998;33:700–4. doi: 10.1016/s0022-3468(98)90190-7. [DOI] [PubMed] [Google Scholar]
- 10.Lugo-Vicente HL. Prenatally diagnosed choledochal cysts: Observation or early surgery? J Pediatr Surg. 1995;30:1288–90. doi: 10.1016/0022-3468(95)90486-7. [DOI] [PubMed] [Google Scholar]
- 11.Liu SL, Li L, Hou WY, Zhang J, Huang LM, Li X, et al. laparoscopic excision of choledochal cyst and Roux-en -Y hepaticojejunostomy in symptomatic neonates. J Pediatr Surg. 2009;44:508–11. doi: 10.1016/j.jpedsurg.2008.08.006. [DOI] [PubMed] [Google Scholar]
- 12.Li L, Liu SL, Hou WY, Cui L, Liu XL, Jun Z, et al. Laparoscopic correction of biliary duct stenosis in choledochal cyst. J Pediatr Surg. 2008;43:644–6. doi: 10.1016/j.jpedsurg.2007.10.064. [DOI] [PubMed] [Google Scholar]
- 13.Ure BM, Schier F, Schmidt AI, Nustede R, Petersen C, Jesch NK. Laparoscopic resection of congenital Choledochal cyst, choledochojejunostomy, and extraabdominal Roux-en-Y anastomosis. Surg Endosc. 2005;19:1055–7. doi: 10.1007/s00464-004-2191-6. [DOI] [PubMed] [Google Scholar]
- 14.Li L, Feng W, Jing-Bo F, Qi-Zhi Y, Gang L, Liu-Ming H, et al. Laparoscopic assisted total cyst excision of choledochal cyst and Roux-en-Y hepatoenterostomy. J Pediatr Surg. 2004;39:1663–6. doi: 10.1016/j.jpedsurg.2004.07.012. [DOI] [PubMed] [Google Scholar]
- 15.Shimura H, Tanaka M, Shimizu S, Mizumoto K. Laparoscopic treatment of congenital choledochal cyst. Surg Endosc. 1998;12:1268–71. doi: 10.1007/s004649900834. [DOI] [PubMed] [Google Scholar]
- 16.Bonnard A, Seguier-lipszyc E, Liguory C, Benkerrou M, Garel C, Malbezin S, et al. Laparoscopic approach as primary treatment of common bile duct stones in children. J Pediatr Surg. 2005;40:1459–63. doi: 10.1016/j.jpedsurg.2005.05.046. [DOI] [PubMed] [Google Scholar]
- 17.Liu SL, Li L, Hou WY, Zhang J, Huang LM, Li X, et al. Laparoscopic excision of choledochal cyst and Roux-en -Y hepaticojejunostomy in symptomatic neonates. J Pediatr Surg. 2009;44:508–11. doi: 10.1016/j.jpedsurg.2008.08.006. [DOI] [PubMed] [Google Scholar]