

Abstract
We describe a patient with inflammatory pseudotumour of the lung. He was a young man who presented with haemotysis and the chest X-ray and computerized tomography were indicative of a nonbenign lesion in the right upper lobe. Excision biopsy confirmed the diagnosis of inflammatory myofibroblastic pseudotumour of the lung. This is a rare inflammatory nonneoplastic condition commonly affecting children and young adults.
1. Introduction
Inflammatory pseudotumour of the lung is a rare condition. It is an inflammatory, reactive, and nonneoplastic process characterized by unregulated growth of inflammatory cells. It occurs most commonly in children and young adults and is usually found incidentally. Inflammatory pseudotumour may mimic lung cancer and thereby pose a diagnostic dilemma for the clinician. We recently managed a case that we describe, as well as review the literature.
2. Case Presentation
A 28-year-old nonsmoking male was referred for diagnostic evaluation of recurrent mild haemoptysis associated with a right upper lobe solitary pulmonary nodule of 8 weeks duration. Chest radiograph revealed a 1.5 × 2 cm coin lesion in the posterior segment of the right upper lobe of the lung (Figure 1).
Figure 1.
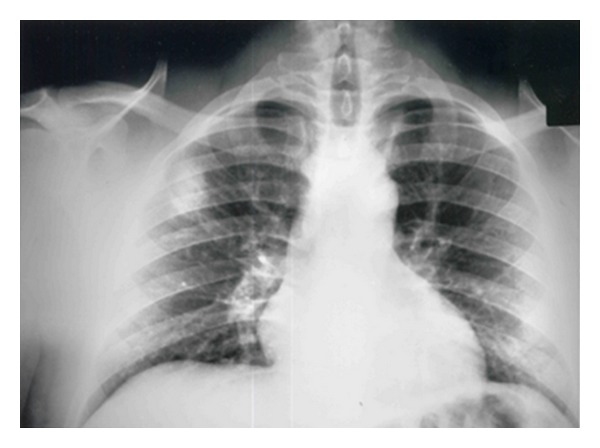
Chest X-ray revealing a rounded opacity in the right upper lobe.
The medical history was noncontributory. A computed tomographic (CT) scan of the chest confirmed the chest radiograph findings; a solid mass was noted in the posterior segment of the right upper lobe of the lung with an area of central lucency (Figure 2).
Figure 2.
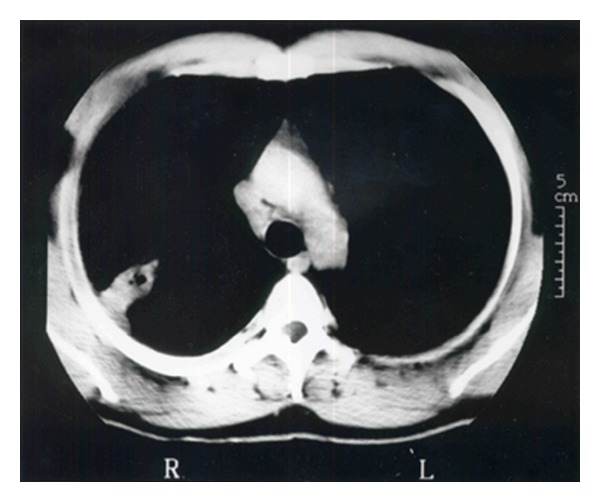
CT scan of the chest demonstrating the lesion in the posterior segment of the right upper lobe with central lucency.
There was no hilar lymphadenopathy. Sputum microscopy, culture, and cytological examination were noncontributory. The ESR was 14, the haemoglobin 14.6 g/dL, and the leukocyte count of 8.8 × 109/L. The other serum haematological and biochemical results were normal.
In view of the patient's ongoing haemoptysis and lack of response to antibiotics he was subjected to an exploratory thoracotomy and wedge resection of the lesion in the right upper lobe. A solid mass in the posterior segment of the right upper lobe was noted and it was excised. No associated lymphadenopathy was noted. Frozen section of the mass revealed no evidence of carcinoma or tuberculosis. The patient developed a right upper lobe lung abscess postoperatively, and underwent a complete right upper lobe lobectomy.
Macroscopically, a well-circumscribed tan-coloured nodule measuring 35 × 15 mm was present. The cut surfaces of the tumour revealed a haemorrhagic necrotic centre. Microscopically, the mass consisted of a heavy inflammatory cell infiltrate composed predominantly of lymphocytes, with plasma cells and histiocytes. Foamy histiocytes with macrophages were also seen, as well as occasional eosinophils and neutrophils. Focal areas of micro-abscess formation with necrosis were also noted. A marked degree of fibrosis of the interstitial tissue was present with proliferating myofibroblasts. The histological characteristics were compatible with an inflammatory myofibroblastic pseudotumour (organising pneumonia-like type; Figure 3).
Figure 3.
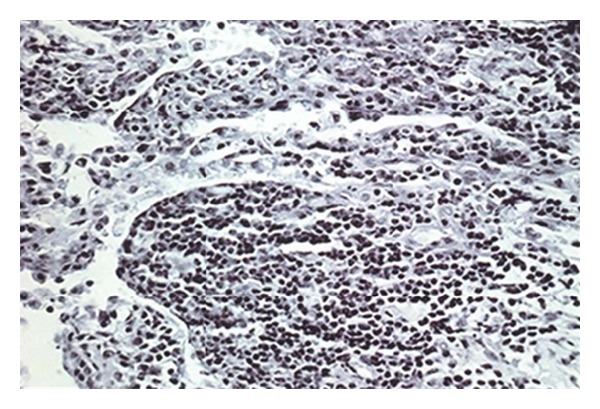
Photomicrograph demonstrating intra-alveolar myofibroblastic proliferation (organising pneumonia-like type).
The postoperative course was uneventful, the patient was discharged from the hospital one week later, and three years after surgical resection the patient remains well and free of disease.
3. Discussion
Inflammatory pseudotumours of the lung are rare and were first described in the lung in 1939 [1]. They are not limited to the lung and can grow in any organ such as the brain, liver, spleen, lymph nodes, salivary glands, breast, soft tissues and skin [2]. Although inflammatory pseudotumours are regarded as inflammatory or reactive lesions rather than neoplasms, they may have features such as local invasion or recurrence, distant metastases, and cytogenetic clonal changes [3–6]. They have an increased predilection to develop in children [7, 8]. The aetiology and pathogenesis remain uncertain. There are several theories, most of which postulate an unchecked or exaggerated immunologic response to a viral or foreign antigen-antibody reaction [9]. Inflammatory pseudotumours typically consists of variable amounts of stromal and cellular elements, with the myofibroblast, a cell involved in tissue repair, recognized as the principal cell-type [3, 10–12]. Depending on the major histopathologic features, inflammatory pseudotumours are divided into the following types: fibrous histiocytoma, lymphoplasmacytic, and organising pneumonia. Because of their variable histology, these masses have several synonyms, including plasma cell granuloma, myofibroblastic tumour, xanthoma, xanthogranuloma, xanthomatous pseudotumour, and plasma cell histiocytoma [2, 4, 9].
Inflammatory pseudotumours are usually considered to be benign tumours, principally occurring in younger patients. They are the most common isolated primary tumour of the lung in children younger than 16 years [8]. More than half of patients are less than 40 years of age [1, 2, 6]. Such lesions account for less than 1% of all lung tumors with no gender or race preponderance [1, 3, 4]. Many patients are asymptomatic, with inflammatory pseudotumours discovered incidentally on examination of chest radiographs. Weight loss, fever, and fatigue have been also described [1]. If the patients are symptomatic, cough, fever, weight loss, fatigue, haemoptysis, dyspnoea, clubbing, chest pain, and arthralgias may be noted [1–4, 13]. No specific findings on physical or laboratory examinations exist.
Radiological examination usually demonstrates a solitary peripheral nodule or mass of 1 to 10 cm in diameter and the lesions are typically peripheral and in the lower lobes [6]. Multiple lung masses, pneumonic consolidation, atelectasis, hilar or mediastinal masses, pleural effusion, and cavitation are unusual [4–6]. Radiographic images and invasive diagnostic procedures, including bronchoscopy and percutaneous fine needle aspiration biopsy, are considered insufficient for diagnosis. Consequently, surgery is crucial for both diagnostic and therapeutic reasons and frozen section histological examination is also subject to errors [1, 3, 9, 13–15].
Macroscopically, inflammatory pseudotumours are well-circumscribed, non-encapsulated, firm, usually yellow-white masses containing variable inflammation, haemorrhage, calcification, and rarely cavitation. Most are parenchymal but some are endobronchial and may cause airway obstruction. Less than 5% invade the mediastinum and/or chest wall. Local recurrence is attributed to incomplete resection of the primary lesion. Metastasis of the tumor to mediastinum or the brain even many years after complete resection has been described. Rarely, simultaneous intra- and extrathoracic locations may occur. Association with other malignancies in sporadic cases has been reported [3, 4, 13].
Microscopically, the lesions consist of variable mixtures of fibroblasts and granulation tissue, fibrous tissue, and inflammatory cells including lymphocytes, histiocytes, giant cells, macrophages, neutrophils, eosinophils, and typically large numbers of plasma cells [1, 3, 4]. Immunohistochemistry has demonstrated the polyclonal nature of plasma cells with immunoglobulin G predominance [16]. Frozen sections performed at the time of operation are often indeterminate [1, 2, 13]. The differential diagnosis includes lymphoma, sarcoma, and fibrosis [3, 4, 12]. Usually the pathologist is able to eliminate a neoplastic process. If uncertainty remains on frozen section and if the mass can be safely removed, complete resection is recommended.
Complete surgical resection of the inflammatory pseudotumour remains the best treatment, to exclude malignancy and to achieve cure [3, 4, 9, 13–15]. Wedge resection is adequate treatment if removal is complete. Lobectomy should be performed if it is required for complete resection and if the patient's pulmonary reserve is adequate. Non-surgical treatment modalities including radiotherapy, chemotherapy, and corticosteroids may have a place in the setting of incomplete surgical resection, multifocal disease, postoperative tumour recurrence, or contra-indications to lung resection [3, 4, 13, 16–20]. Although spontaneous regression may occur, local expansion may cause significant morbidity and occasional death. The prognosis of these rare tumours is excellent after complete surgical excision. There is a low incidence of recurrence with long-term follow-up after complete removal of the mass [3, 4, 13, 17, 21]. Patients with recurrent disease should undergo re-resection [1, 4, 14, 17].
4. Conclusion
Although inflammatory pseudotumours of the lung are rare and the most common clinical picture is one of an asymptomatic, well-circumscribed lung mass that mimics cancer, clinicians need to bear in mind the diverse clinical presentations. Surgical excision is usually indicated to reach a firm diagnosis and cure. As preoperative investigation is not diagnostic, excision of the mass is imperative in order to exclude malignancy. Complete resection, when possible, is safe and leads to excellent survival and remains the key to prevent recurrence.
References
- 1.Copin MC, Gosselin BH, Ribet ME. Plasma cell granuloma of the lung: difficulties in diagnosis and prognosis. Annals of Thoracic Surgery. 1996;61(5):1477–1482. doi: 10.1016/0003-4975(96)00081-1. [DOI] [PubMed] [Google Scholar]
- 2.Anthony PP. Inflammatory pseudotumour (plasma cell granuloma) of lung, liver and other organs. Histopathology. 1993;23(5):501–503. doi: 10.1111/j.1365-2559.1993.tb00508.x. [DOI] [PubMed] [Google Scholar]
- 3.Bahadori M, Liebow AA. Plasma cell granulomas of the lung. Cancer. 1973;31(1):191–208. doi: 10.1002/1097-0142(197301)31:1<191::aid-cncr2820310127>3.0.co;2-d. [DOI] [PubMed] [Google Scholar]
- 4.Matsubara O, Tan-Liu NS, Kenney RM, Mark EJ. Inflammatory pseudotumors of the lung: progression from organizing pneumonia to fibrous histiocytoma or to plasma cell granuloma in 32 cases. Human Pathology. 1988;19(7):807–814. doi: 10.1016/s0046-8177(88)80264-8. [DOI] [PubMed] [Google Scholar]
- 5.Batsakis JG, Luna MA, El-Naggar AK, Goepfert H. ‘Inflammatory pseudotumor’: what is it? How does it behave? Annals of Otology, Rhinology and Laryngology. 1995;104(4):329–331. doi: 10.1177/000348949510400415. [DOI] [PubMed] [Google Scholar]
- 6.Snyder CS, Dell'Aquila M, Haghighi P, Baergen RN, Suh YK, Yi ES. Clonal changes in inflammatory pseudotumor of the lung: a case report. Cancer. 1995;76:1545–1549. doi: 10.1002/1097-0142(19951101)76:9<1545::aid-cncr2820760908>3.0.co;2-h. [DOI] [PubMed] [Google Scholar]
- 7.Agrons GA, Rosado-de-Christenson ML, Kirejczyk WM, Conran RM, Stocker JT. Pulmonary inflammatory pseudotumor: radiologic features. Radiology. 1998;206(2):511–518. doi: 10.1148/radiology.206.2.9457206. [DOI] [PubMed] [Google Scholar]
- 8.Cohen MC, Kaschula RO. Primary pulmonary tumors in childhood: a review of 31 years’ experience and the literature. Pediatric Pulmonology. 1992;14(4):222–232. doi: 10.1002/ppul.1950140405. [DOI] [PubMed] [Google Scholar]
- 9.Gal AA, Koss MN, McCarthy WF, Hochholzer L. Prognostic factors in pulmonary fibrohistiocytic lesions. Cancer. 1994;73(7):1817–1824. doi: 10.1002/1097-0142(19940401)73:7<1817::aid-cncr2820730708>3.0.co;2-k. [DOI] [PubMed] [Google Scholar]
- 10.Coffin CM, Dehner LP, Meis-Kindblom JM. Inflammatory myofibroblastic tumor, inflammatory fibrosarcoma, and related lesions: an historical review with differential diagnostic considerations. Seminars in Diagnostic Pathology. 1998;15(2):102–110. [PubMed] [Google Scholar]
- 11.Dehner LP. The enigmatic inflammatory pseudotumours: the current state of our understanding, or misunderstanding. The Journal of Pathology. 2000;192:277–279. doi: 10.1002/1096-9896(200011)192:3<277::AID-PATH749>3.0.CO;2-E. [DOI] [PubMed] [Google Scholar]
- 12.Bakhos R, Wojcik EM, Olson MC. Transthoracic fine-needle aspiration cytology of inflammatory pseudotumor, fibrohistiocytic type: a case report with immunohistochemical studies. Diagnostic Cytopathology. 1998;19:216–220. doi: 10.1002/(sici)1097-0339(199809)19:3<216::aid-dc13>3.0.co;2-h. [DOI] [PubMed] [Google Scholar]
- 13.Ishida T, Oka T, Nishino T, Tateishi M, Mitsudomi T, Sugimachi K. Inflammatory pseudotumor of the lung in adults: radiographic and clinicopathological analysis. Annals of Thoracic Surgery. 1989;48(1):90–95. doi: 10.1016/0003-4975(89)90187-2. [DOI] [PubMed] [Google Scholar]
- 14.Cerfolio RJ, Allen MS, Nascimento AG, et al. Inflammatory pseudotumors of the lung. Annals of Thoracic Surgery. 1999;67(4):933–936. doi: 10.1016/s0003-4975(99)00155-1. [DOI] [PubMed] [Google Scholar]
- 15.Mandelbaum I, Brashear RE, Hull MT. Surgical treatment and course of pulmonary pseudotumor (plasma cell granuloma) Journal of Thoracic and Cardiovascular Surgery. 1981;82(1):77–82. [PubMed] [Google Scholar]
- 16.Berardi RS, Lee SS, Chen HP, Stines GJ. Inflammatory pseudotumors of the lung. Surgery Gynecology and Obstetrics. 1983;156(1):89–96. [PubMed] [Google Scholar]
- 17.Alexiou C, Obuszko Z, Beggs D, Morgan WE. Inflammatory pseudotumors of the lung. Annals of Thoracic Surgery. 1998;66(3):948–950. doi: 10.1016/s0003-4975(98)00565-7. [DOI] [PubMed] [Google Scholar]
- 18.Hoover SV, Granston AS, Koch DF, Hudson TR. Plasma cell granuloma of the lung, response to radiation therapy: report of a single case. Cancer. 1977;39(1):123–125. doi: 10.1002/1097-0142(197701)39:1<123::aid-cncr2820390121>3.0.co;2-h. [DOI] [PubMed] [Google Scholar]
- 19.Boman F, Champigneulle J, Boccon-Gibod L, et al. Endobronchial, aggressive, multifocal, recurrent pulmonary inflammatory myofibroblastic tumor. Annales de Pathologie. 1995;15(3):207–210. [PubMed] [Google Scholar]
- 20.Fornell-Pérez R, Santana-Montesdeoca JM, García-Villar C, Camacho-García MC. Two types of presentation of pulmonary inflammatory pseudotumors. Archivos de Bronconeumología. 2012;48:296–299. doi: 10.1016/j.arbres.2011.09.001. [DOI] [PubMed] [Google Scholar]
- 21.Huellner MW, Schwizer B, Burger I, et al. Inflammatory pseudotumor of the lung with high FDG uptake. Clinical Nuclear Medicine. 2010;35(9):722–723. doi: 10.1097/RLU.0b013e3181ea33d0. [DOI] [PubMed] [Google Scholar]