

Abstract
Objective
This study investigates the relationship between anxiety symptoms and adaptive function in children with Chromosome 22q11.2 Deletion Syndrome (22q11.2DS).
Methods
Seventy-eight children ages 7-14 years with 22q11.2DS and 36 typically developing (TD) children without known genetic syndromes participated in a larger study of neurocognition. Parents completed questionnaires about their child’s anxiety symptoms (Behavior Assessment System for Children, 2nd ed.: BASC-2 and Spence Children’s Anxiety Scale: SCAS) and adaptive functioning (BASC-2 and Adaptive Behavior Assessment System, 2nd ed.: ABAS-II). Within the 22q11.2DS group, different DSM-IV anxiety domains were also analyzed using SCAS subscales.
Results
Based on parent report, 19% of children with 22q11.2DS had a prior diagnosis of an anxiety disorder vs. 58% with at least one elevated anxiety score (BASC-2 and/or SCAS). Mean BASC-2 anxiety scores were significantly higher in 22q11.2DS (55.6+12.5) than TD (48.3+10; p=0.003) and a greater percentage of children with 22q11.DS (37%) had elevated BASC-2 anxiety scores compared with TD (14%; p=0.01). Higher anxiety scores were related to lower adaptive function (r=−0.27, p=0.015) but there was no relationship between WISC-IV FSIQ and BASC-2 adaptive skills (r=−0.06, p=0.6) in the 22q11.2DS group. For the individual SCAS anxiety subscales, panic-agoraphobia (r=−0.38, p=0.03), physical injury (r=−0.34, p=0.05), and obsessive compulsive disorder (r=−0.47, p=0.005) were significantly negatively related to adaptive function in 22q11.2DS.
Conclusions
Despite known risk, anxiety is under-identified in children with 22q11.2DS. The presence of anxiety symptoms, but not intelligence levels, in children with 22q11.2DS is negatively correlated with adaptive function and impacts everyday living skills.
INTRODUCTION
The most common human microdeletion occurs at chromosome 22q11.2 with a prevalence of at least 1:4000 live births [1]. The resulting syndrome is commonly now referred to as chromosome 22q11.2 deletion syndrome (22q11.2DS), encompassing DiGeorge, Velocardiofacial and other syndrome labels. There is a wide spectrum of involvement, and children with 22q11.2DS face multiple challenges from co-morbid medical, developmental, and psychiatric symptoms. Medical conditions associated with 22q11.2DS include congenital heart disease, immune difficulties, and velopharyngeal dysfunction, to name a few. The neurocognitive impairments in individuals with 22q11.2DS include full scale IQ in the borderline to low average range [2] with verbal skills generally stronger than nonverbal abilities, although there is significant individual variability [3]. There is a higher prevalence of childhood mental health disorders such as anxiety and attention deficit hyperactivity disorder [4] and in late adolescence to early adulthood, up to 30% of individuals develop psychotic disorders such as schizophrenia and schizophreniform disorders [5]. While little is known about what early risk factors predict the later development of serious psychiatric illness in 22q11.2DS, one longitudinal study suggests that childhood anxiety disorders and declining verbal IQ precede the emergence of schizophrenia [6].
According to a recent review [4], approximately 40% of children with 22q11.2DS suffer from some type of anxiety disorder, with the prevalence spanning 4-61%. Specific phobias are most common, followed by Generalized Anxiety Disorder, Separation Anxiety, and Obsessive Compulsive Disorder [7]. Early negative experience has been shown to increase risk of anxiety and is associated with atypical development of the physiological stress response [8]. Thus, serious medical complications such as congenital heart disease, feeding difficulties, and often multiple surgeries or hospitalizations may also predispose some children with 22q11.2DS to anxiety disorders due to stressors associated with repeated medical procedures or poor sense of control over one’s body [9].
In addition to mental health difficulties, individuals with 22q11.2DS face cognitive challenges, with cognitive abilities in the borderline or mild Intellectual Disability (ID) range. ID is characterized by below-average cognitive functioning and impairments in adaptive behaviors that impact daily living [10]. While intelligence quotient (IQ) scores are often reported as an important outcome measure, IQ tends to represent acquired knowledge and test performance, rather than an individual’s real-world daily functioning (i.e. adaptive skills) [11] or the ability to cope with everyday stressors. Adaptive scores are a separate, but related, construct to IQ and are more ecologically valid metrics of development that reflect age-appropriate expectations of one’s ability to independently function and communicate in practical and social environments, such as at home, school, in the community or on the job [12]. Adaptive skills are necessary for becoming an independent, successful adult in society and are often measured by standardized assessments such as the Vineland Adaptive Behavior Scales (VABS-II) [13] or Adaptive Behavior Assessment System for Children (ABAS-II) [14]. Identifying factors that lead to better adaptive skills are useful targets for intervention to improve an individual’s real world functioning.
The interaction of anxiety and cognitive impairments can negatively affect development by reinforcing maladaptive behaviors. For example, cognitive challenges may be a source of stress and anxiety, leading to avoidance of academic and/or social situations. Avoidance decreases opportunities for learning, putting children at an even greater disadvantage. In addition, poor interpretation of environmental and social cues secondary to anxiety can also affect daily functioning and limit one’s ability to interact and learn from the environment. Furthermore, anxiety can cause physiological changes via cortisol and the stress response, which may have deleterious consequences on both brain and behavior with prolonged exposure. All of these factors may lead to an iterative cycle of events that could exacerbate the already increased risk for psychiatric disorders due to the 22q11.2 deletion [9].
What determines adaptive functioning in children with 22q11.2DS? Our clinical impression working with the school-aged 22q11.2DS population suggests that there is prominent anxiety, and children with more severe anxiety symptoms seem to be most impaired in their everyday functioning. While there is a robust relationship between IQ and adaptive function in typical [13] and other developmentally delayed [15] populations, this has not been investigated specifically in children with 22q11.2DS. Anxiety affects individuals regardless of IQ and may interfere with the relationship between IQ and adaptive functioning in children with 22q11.2DS. The purpose of this study was to empirically test these clinical impressions using standardized assessments. We hypothesized that:
A greater proportion of children with 22q11.2DS will have elevated anxiety scores compared with typically developing children.
In children with 22q11.2DS, those with higher anxiety symptoms will have lower adaptive scores.
In addition, we investigated in more detail the domains of anxiety that may affect adaptive scores, which could be useful for intervention and prevention.
METHODS
Participants
This cross-sectional study included seventy-eight children with 22q11.2DS (female = 36, male = 42) ages 7-15 years (mean age 10.6+2.2 years) who were part of a larger study of neurocognitive function that included neuroimaging. 22q11.2DS diagnosis was confirmed with FISH. Recruitment consisted mainly from postings on the Cognitive Analysis and Brain Imaging Laboratory webpage or the MIND Institute’s Volunteer Research Registry, and participants were not selected from clinical or subspecialty visits related to 22q11.2DS. Instead, almost all families contacted our team asking to participate. The comparison group consisted of 36 (21 girls and 15 boys; mean age 10.8+2.5 years) typically developing (TD), age-matched children from the local geographic area without 22q11.2DS or other known genetic disorders recruited from the MIND Institute’s Volunteer Research Registry available on-line. Inclusion criteria included English speakers and availability of a parent or legal guardian who could provide consent and complete standardized measures of the child’s behavior. Any children with contraindication to MRI (pacemaker, etc.) scanning were excluded due to the requirements for participation in the larger study. TD children were excluded if there were any known structural brain abnormalities or birth complications such as a history of prematurity or multiple births. Socio-economic status was measured with the Hollingshead Four Factor Index of Social Status. All procedures were approved by the Institutional Review Board at the University of California Davis.
Both anxiety measures (Behavior Assessment System for Children, 2nd edition and Spence Children’s Anxiety Scale; see below for description) are based on a mean score of 50 with a 10-point standard deviation. A sample size of 28 children in each group is needed to detect a difference of 3/4 standard deviation (7.5 points) with a power of 0.8 and α=0.05 (two-tailed). Sample size was calculated using STATA version 9.2 [16].
Measures
Study protocol included neuropsychological testing by a clinical psychologist and a developmental-behavioral pediatric evaluation including history of prior psychiatric diagnoses. Full-scale IQ was assessed using the Wechsler Intelligence Scale for Children, 4th edition [17]. Parents completed standardized questionnaires of their child’s behaviors and skills. Anxiety symptoms and adaptive skills were measured on two levels (1-general and 2-specific):
Analysis 1: General measures of anxiety and adaptive skills (22q11.2DS vs. TD)
The Parent Rating Scales of the Behavior Assessment System for Children, 2nd edition (BASC-2) [18], a 134-160 item questionnaire used to measure children’s internalizing and externalizing problems, adaptive skills, and behavioral symptoms, was obtained for all children as part of the protocol for the larger study on neurocognition. This analysis included general measures of anxiety and adaptive skills from the BASC-2, which is normed based on current U.S. census characteristics and includes a “clinical norm sample” of children referred for clinical conditions such as learning disability, developmental delay/intellectual disability, emotional /behavioral disturbance, ADHD, and other conditions. T-scores are normed with an average of 50 and a 10-point standard deviation, so anxiety scores > 60 and adaptive skills scores < 40 are considered problematic.
Analysis 2: Specific measures of anxiety and adaptive skills (22q11.DS subset)
Anxiety: The BASC-2 does not differentiate between specific anxiety domains, and due to our clinical impression of anxiety having a significant impact on children with the deletion, we started collecting more detailed measures of anxiety and adaptive measures (see Table II) prospectively for a subset of participants with 22q11.2DS, with complete data available for 33 (of the 78) 22q11.2DS children included in Analysis 1. The parent Spence Children’s Anxiety Scale (SCAS) [19] is a 38-item questionnaire that measures the severity of anxiety symptoms along the dimensions of the DSM-IV diagnostic criteria for anxiety disorders, including panic-agoraphobia, separation anxiety, physical injury, social phobia, obsessive compulsive disorder, and generalized anxiety disorder. A total anxiety score can also be calculated. Similar to the BASC-2, elevated SCAS subscale t-scores are those > 60. The SCAS correlates well with the internalizing subscale of the Child Behavior Checklist but has advantages over the CBCL by providing more detailed symptoms of anxiety along DSM-IV classifications and differentiating between children with anxiety disorders and normal controls [20].
Table II.
Specific measures of anxiety and adaptive functioning (n=33) [22q11.2DS only]
| Anxiety | Mean (±SD) | # with score ≥60 (%) |
|---|---|---|
| Parent SCAS subscales | ||
| total | 63.8 (±10) | 19 (58%) |
| panic-agoraphobia | 52.8 (±10.7) | 7 (21%) |
| separation anxiety | 62.8 (±13.8) | 20 (61%) |
| physical injury | 63.3 (±14.2) | 18 (55%) |
| social phobia (n=38) | 57.7 (±14) | 14 (42%) |
| obsessive compulsive (n=38) | 53.9 (±8.9) | 7 (21%) |
| generalized anxiety disorder (n=38) | 58.3 (±12.4) | 13 (39%) |
| Adaptive functioning | Mean (±SD) | # with score<70 (%) |
| ABAS-II | ||
| Global Adaptive Composite (GAC) | 75.5 (±16.5) | 15 (45%) |
Adaptive functioning: The Adaptive Behavior Assessment System, 2nd edition (ABAS-II) [14], a more comprehensive norm-referenced scale of daily living skills, was also collected from this subset. The ABAS-II General Adaptive Composite (GAC) is a standard score with a mean of 100 and a 15 point standard deviation. GAC scores < 70 are considered “Extremely Low” and indicate significant functional impairment. Norms based on ratings of more than 3,200 individuals in 31 age groups are stratified by sex, race/ethnicity, and level of education. In addition to typically developing participants, the standardization sample included 20 clinical groups, representing disorders such as autism, ADHD, and visual impairment [18].
Statistical Analyses
Two-tailed student’s t-tests were used to compare group means for continuous variables, such as age, FSIQ, BASC-2 anxiety and BASC-2 adaptive skills. In addition, gender ratios and the percentage of children scoring in the elevated range for anxiety (BASC-2) in the 22q11.2DS group were compared to the control group using chi-2 analysis. First, the relationship between anxiety and adaptive function were examined for the entire sample (22q11.2DS and TD combined) with multiple linear regression. Adaptive function (as measured by BASC-2 adaptive skills or ABAS-II GAC) was the dependent variable and anxiety (as measured by BASC-2 anxiety or individual SCAS domains) was the independent variable, with group as a covariate. Linear regression was also used for within group correlational analyses of anxiety and adaptive function and to characterize the relationship between FSIQ and adaptive function (BASC-2 adaptive skills) with gender and SES as covariates. All statistical analyses were calculated using STATA version 9.2 [16].
RESULTS
There were no significant differences in demographics such as age, gender, or SES between the 22q11.2DS and TD groups. Mean FSIQ was in the borderline range (76+12.9) for the 22q11.2DS group and average range (108.8+13) for the TD group (see Table I). Based on qualitative report from parents, 19% of the 22q11.2DS group had a prior diagnosis of an anxiety disorder from a medical or mental health professional. A far greater percentage (58%; n=46) of the children with 22q11.2DS had elevated (t-score > 60) BASC-2 or SCAS anxiety scores. FSIQ, BASC-2 anxiety, and BASC-2 adaptive skills were available for all 78 children with 22q11.2DS and 36 TD children in Study 1. We started collecting more detailed anxiety and adaptive measures (see Table II) prospectively for more recent participants with 22q11.2DS due to our clinical impression of anxiety having a significant impact on children with the deletion, with both (parent) SCAS and ABAS-II scores available for 33 (of 78) children with 22q11.2DS (Study 2). There were no significant differences between the larger 22q11.2DS group (n=78) and smaller subgroup for which SCAS scores (n=34) were available, with similar age (10.9 + 2.3 years; p=0.2), % male (55.3%; p=0.8), FSIQ (76.2 + 11.9; p=0.9), SES (50.8 + 9.8; p=0.4), and mean BASC-2 anxiety scores (57.7 + 12.5; p=0.2) in the smaller SCAS subgroup.
Table I.
Demographic characteristics
| 22q11.2DS | Typical (TD) | p-value | |
|---|---|---|---|
| Sample size | n=78 | n=36 | |
| Age in years | 10.6 (±2.2) | 10.8 (±2.5) | 0.74 |
| FSIQ* | 76.4 (±12.9) | 108.8 (±13) | <0.001 |
| SES | 49.7 (±10.4) | 50.4 (±9.4) | 0.77 |
| Male [n (%)] | 42 (54%) | 15 (42%) | 0.23 |
p<0.05
Age, FSIQ, and SES presented as mean +/− standard deviation
Analysis 1 (22q11.2DS [n=78] vs. TD [n=36]): Mean BASC-2 anxiety scores were significantly higher in the children with 22q11.2DS compared to TD children by 7.3 points, 55.6 +12.5 vs. 48.3 +10 (p=0.003). BASC-2 anxiety scores were in the average range for both groups, although a significantly greater portion of children with 22q11.2DS (29 of 78; 37%) had elevated (>60) BASC-2 anxiety scores compared to typical children (5 of 36; 14%; p=0.01). These prevalence rates are similar to those reported in the literature for both the 22q11.2DS (approximately 40%) [4] and the general population (approximately 10%) [21]. Mean BASC-2 adaptive skills scores were significantly higher in TD (54 +8.3) compared to 22q11.2DS (39.2 +9.8; p<0.001), with higher adaptive scores indicating better functioning. Forty-two (54%) children with 22q11.2DS had low (BASC-2 adaptive skills <40) adaptive scores, whereas only 2 (6%) TD children were in this range (p<0.001).
When the entire sample (i.e. both the 22q11.2DS and TD groups combined) was tested, higher anxiety scores were related to lower adaptive function (r=−0.42, p<0.001). A multiple regression model with group and BASC-2 anxiety as covariates predicted BASC-2 adaptive skills (adjusted R2=0.4, p<0.001). Both group (t=−6.76, p<0.001) and BASC-2 anxiety (t=−3.38, p<0.001) were statistically significant predictors, of adaptive function, so we then performed within group analysis to see if the relationship between BASC-2 adaptive skills and anxiety differed by group.
Within group analysis revealed a negative relationship between anxiety and adaptive function in both TD (r=−0.42, p=0.01) and 22q11.2DS (r=−0.27, p=0.015) using the BASC-2. As we hypothesized, higher anxiety scores were related to lower adaptive function in children with 22q11.2DS (Figure 1). This finding remained significant after adjusting for FSIQ, gender, and SES (r=−0.26, p=0.019). There was no relationship between WISC-IV FSIQ and BASC-2 adaptive skills (Figure 2) in children with 22q11.2DS, either with (r=−0.08, p=0.5) or without (r=−0.06, p=0.6) adjusting for the above covariates. By contrast, TD children in our study showed a strong positive correlation between FSIQ and adaptive function (unadjusted r=0.5, p=0.003; adjusted r=0.6, p=0.002) (Figure 2).
Figure 1.
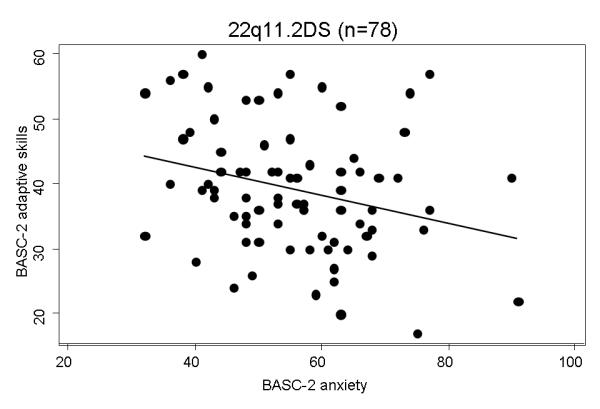
BASC-2 anxiety vs. BASC-2 adaptive skills in children with 22q11.2DS
Figure 2.
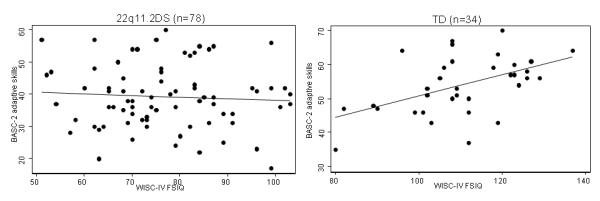
WISC-IV FSIQ vs. BASC-2 adaptive skills in children with 22q11.2DS (left) and TD (right)
There was no relationship between BASC-2 anxiety and FSIQ in the 22q11.2DS group (r=0.06, p=0.62).
Analysis 2 (22q11.2DS only [n=33]): Individual anxiety subscales of the SCAS are reported in Table II, along with ABAS-II scores. Total anxiety (r=−0.35, p=0.04), Panic-agoraphobia (r=−0.38, p=0.03), physical injury (r=−0.34, p=0.05), and obsessive compulsive disorder (r=−0.47, p=0.005) were significantly negatively related to the ABAS-II Global Adaptive Composite in children with 22q11.2DS. Separation anxiety (r=−0.32, p=0.07) trended towards significance. Social phobia (r=0.006, p=0.97) and generalized anxiety disorder (r=−0.05, p=0.78) were not related to ABAS-II GAC.
Similar to the results in Analysis 1, there was no relationship between ABAS-II GAC and WISC-IV FSIQ (r=−0.02, p=0.9).
DISCUSSION
Based on our study of children ages 7-14 years with 22q11.2DS, anxiety symptoms are quite common and negatively related to adaptive functioning. This has serious clinical implications because, from our sample, anxiety appears to be underidentified by health care professionals despite known elevated risk in this population [4, 22]. Only 19% of our participants had been given a prior diagnosis of an anxiety disorder, yet 58% of them demonstrated elevated BASC-2 or SCAS scores representing significant anxiety symptoms. Certain subtypes of anxiety were more frequent than others, with fear-based symptoms (i.e. separation anxiety and fear of physical injury) present in approximately 60% of children, compared to a 20% rate of obsessive compulsive or panic-agoraphobia symptoms. This discrepancy may provide insight for future study of the physiological mechanisms involved in these types of anxiety, along with targeted interventions.
Our initial study protocol addressed a global measure of anxiety from the BASC-2, with approximately 38% of children with 22q11.2DS scoring in the elevated range. While this was consistent with the prevalence of anxiety disorders reported in the literature for this population [4], this also seemed to underestimate the actual rate given our clinical impression of frequent anxiety symptoms causing significant impairment and was our motivation for our secondary analysis using the SCAS. The mean BASC-2 anxiety score in the 22q11.2DS group was in the average range, although it was significantly higher than the mean BASC-2 anxiety score in the typical group by 7 points. This may be related to the heavy loading of questions in the BASC-2 relating to generalized anxiety (mostly worries), which on the SCAS was present on only around 40% of children, and the inability of some children with 22q11.2DS to explicitly express or communicate anxiety symptoms due to verbal and intellectual impairments. Inadequate treatment of identified mental health conditions in children with 22q11.2DS has also been reported [22], and together with our findings that anxiety symptoms are common and often unidentified, there is a demonstrated need to address this pervasive problem that is a prime target for intervention.
We started collecting more detailed information on DSM-IV related anxiety subtypes using the SCAS to evaluate our hypothesis that the general nature of the BASC-2 was underestimating the prevalence of anxiety in children with 22q11.2DS. While mean scores on the different anxiety measures were mostly in the average range, there was a wide spread of scores, with at least 18% of the children with 22q11.2DS having elevated t-scores on any anxiety subscale and up to 60% with elevations for certain anxiety subtypes such as separation anxiety. Importantly, it was these children that had the greatest difficulty with everyday living skills, which highlights the need to treat anxiety in this population. The same pattern held also for the general measures from the BASC-2.
Specific subtypes of anxiety may predict lower adaptive functioning, including panic-agoraphobia, physical injury, and obsessive compulsive disorder. Separation anxiety, social phobia, and generalized anxiety disorder, while present in greater than 40% of our sample, do not seem to affect adaptive functioning and further study of what types of anxiety symptoms influence this outcome should be pursued.
Anxiety symptoms are common in other neurogenetic disorders, such as Down syndrome [23], fragile X syndrome [24], and the sex chromosome aneupoidies such as XXY [25] and Trisomy X [26]. Few studies have looked at the relationship between anxiety and adaptive function, with high anxiety related to lower IQ in typical populations [27], but this is not the case in some developmental disorders such as autism, where higher anxiety is found in those with high IQ [28]. Our findings indicate that in 22q11.2DS, anxiety may affect individuals across all levels of cognition, thereby suggesting other modulatory factors such as environmental demands. This may have broader applicability to other neurodevelopmental disorders and there is a need for further study of the relationship between anxiety and IQ across disorders.
Our findings highlight the importance of identifying and treating anxiety symptoms in children with 22q11.2DS. While intellectual potential is certainly an important outcome measure, there are other factors that influence long-term function. Anxiety interferes with the deployment of one’s cognitive potential to attain maximal adaptive functional skills, as evidenced by the lack of relationship between IQ and adaptive functioning in our 22q111.2DS sample. In our control group of typically developing children who had a low prevalence of anxiety, higher IQ scores were related to better adaptive functioning, consistent with what is reported in the literature for typical and many developmentally delayed populations. We postulate that this lack of correlation between IQ and adaptive functioning is related to anxiety, as anxiety may potentially alter one’s interaction with the environment through modulation of attention and fear conditioning [29-31] so that anxious children miss out on learning opportunities because relatively benign situations are perceived as threatening. Another possibility is that anxious children are less aware or engaged during routine learning environments because there is competition for their attentional resources that are instead focused on perceived threat. Interventions, both behavioral and pharmacologic, to reduce anxiety are available and may improve adaptive functioning and quality of life in the immediate future. Further, evidenced-based interventions targeting anxiety are more readily available than interventions geared towards improving cognition. Behavioral techniques that teach useful coping skills and encourage positive environmental interactions allow one to better perform to the maximum of his/her cognitive potential in order to encourage independent functioning and improve relationships.
It is also possible that early anxiety reduction and the attainment of coping skills could protect against the development of serious psychopathology later in life, which is particularly relevant to the 22q11.2DS population given these individuals’ elevated risk for schizophrenia. In our analysis, the obsessive compulsive and panic-agoraphobia subscales of the SCAS were more strongly related to adaptive function. In the general population, there is an increased risk of schizophrenia in individuals previously diagnosed with an anxiety disorder [32] and anxiety disorders and schizophrenia are often comorbid [33]. In schizophrenia, anxiety affects quality of life and may mediate social and functional impairment [33]. The only longitudinal study of which we are aware that examined this relationship in children with 22q11.2DS indicated that those with any anxiety, but particularly OCD, appeared be at higher risk for schizophrenia at follow-up 5 years later [6]. Mental health screening is particularly important in order to identify difficulties early and provide treatment.
In the context of early negative life events, ongoing cognitive and socioemotional challenges and a genetic diathesis, the contribution of stress from poor coping skills and high levels of anxiety may account for some of the elevated risk of schizophrenia in adolescents and young adults with 22q11.2DS [9]. Chronic anxiety and panic symptoms may contribute to poor developmental outcomes through prolonged activation of the physiological stress response, including chronically elevated glucocorticoid and catecholamine activation. Chronic glucocorticoid activation has been shown to have deleterious effects on a number of brain regions (including the prefrontal cortex and limbic regions) that could contribute to and also exacerbate emotional dysregulation in a reciprocal and iterative fashion [34].
As a result of these findings, we have begun to refer to children with high anxiety and low adaptive functioning scores as “strugglers” and those with the opposite pattern as “copers”. Since, in our sample, coper/struggler status is unrelated to intellectual functioning levels and may modulate risk or resilience with respect to psychiatric illness [9], we are starting to investigate the factors that contribute to being a “coper” or a “struggler” and how to intervene to convert the latter into the former with evidenced based therapies such as Cognitive Behavioral Therapies and/or SSRI medication and with newer emerging research based strategies [35].
Limitations of our study include a smaller sample size (n=34) with more specific measures of anxiety from the SCAS, although our sample size of 78 for general measures is greater than most of the studies on anxiety in 22q11.2DS in the literature, with subject numbers mostly in the 20’s [7, 36, 37]. Based on our power analysis calculations, our study may have been slightly underpowered to detect smaller differences in anxiety scores between groups, which would tend to underestimate our findings. However, given our significant results, our findings seem quite robust. Given the low rate of general anxiety on the BASC-2, we did not collect more detailed anxiety measures for the TD group, which is another limitation. While we employed the use of standardized behavioral measures such as the BASC-2, SCAS, and ABAS-II, these tools rely on parental report and may not truly represent the child’s internalizing symptoms. Child self-report scales are available, although we chose the parental scales due to the younger age of our population complicated by developmental/intellectual delay, which limits the validity of self-report because of conceptual, linguistic, and social limitations [38, 39]. In addition, there may be selection bias of families with children experiencing behavioral problems or academic difficulties being more likely to participate in our study because they are seeking help for these conditions, although it is surprising that very few had sought out care through their own medical or mental health care system. However, Young et al. [22] also note that children in their sample with 22q11.2DS and psychopathology were not receiving needed mental health services and our finding of the dissociation between FSIQ and adaptive function highlight the importance of intervention. One last limitation is the subjective nature of anxiety symptoms, and we did not collect physiological measures of arousal.
Strengths of our study include the inclusion of a typically developing control group and relatively large sample size. Data on adaptive function and anxiety were collected from children participating in a larger study of neurocognition in 22q11.2DS and participants were not recruited from a psychiatry clinic or study specifically focused on anxiety or behavior problems, which decreases ascertainment bias. We add to the literature by relating anxiety symptoms to adaptive functioning, which may be a more pragmatic outcome measure than IQ alone. Our findings suggest that treatment of anxiety symptoms may influence adaptive function and support independent life skills. This is important considering that interventions to decrease anxiety are more readily available than treatments focused on improving IQ.
In summary, anxiety symptoms are prevalent in children with 22q11.2DS and interfere with adaptive functioning. The often-observed relationship between IQ and adaptive functioning is not observed in children with 22q11.2DS, perhaps because of their significant anxiety symptoms. Validation of our findings that panic-agoraphobia and obsessive compulsive disorder more significantly impact daily functioning will be useful for future studies to help identify prognostic factors and implement targeted therapies.
Acknowledgements
We thank the families who participated in our study and appreciate the advice and efforts of Kristopher de Ga, Joel Stoddard, M.D., Xiaowei Yang , Ph.D, and Robin Hansen, M.D.
No pharmaceutical company has been directly involved in this study. NT is principal investigator on clinical trials for Seaside Therapeutics and KA is sub-investigator on clinical trials for Roche, Curemark, Forrest, Seaside Therapeutics, Novartis, and Johnson & Johnson. They have not taken any personal salary from any pharmaceutical company and defer to the editor for advice on whether or not to declare this as a conflict of interest. LI, EAB, EJ, and TJS have no conflicts of interest to declare.
Conflicts of Interest and Source of Funding: This work was supported by the National Institutes of Health R01042974, Children’s Miracle Network, the Dempster Family Foundation, the University Center for Excellence in Developmental Disabilities 90DD0670, and the UC Davis Clinical and Translational Science Center - UL1 RR024146 from the National Center for Research for Medical Research (NCRR).
Footnotes
Its contents are solely the responsibility of the authors and do not necessarily represent the official view of NCRR or NIH. Information on Re-engineering the Clinical Research Enterprise can be obtained from http://nihroadmap.nih.gov/clinicalresearch/overview-translational.asp. No pharmaceutical company has been directly involved in this study. NT is principal investigator on clinical trials for Seaside Therapeutics. KA is sub-investigator on clinical trials in autism and fragile X syndrome for Roche, Curemark, Forrest, Seaside Therapeutics, and Novartis. They have not taken any personal salary from any pharmaceutical company. For the remaining authors none were declared.
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Driscoll DA, Salvin J, Sellinger B, et al. Prevalence of 22q11 microdeletions in DiGeorge and velocardiofacial syndromes: implications for genetic counselling and prenatal diagnosis. Journal of Medical Genetics. 1993;30(10):813–7. doi: 10.1136/jmg.30.10.813. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Moss EM, Batshaw ML, Solot CB, et al. Psychoeducational profile of the 22q11. 2 microdeletion: Aa complex pattern. Journal of PediatricsJ Pediatr. 1999;134(2):193–198. doi: 10.1016/s0022-3476(99)70415-4. [DOI] [PubMed] [Google Scholar]
- 3.De Smedt B, Devriendt K, Fryns JP, et al. Intellectual abilities in a large sample of children with Velo-Cardio-Facial Syndrome: an update. J Intellect Disabil Res. 2007;51(Pt 9):666–70. doi: 10.1111/j.1365-2788.2007.00955.x. [DOI] [PubMed] [Google Scholar]
- 4.Jolin EM, Weller RA, Weller EB. Occurrence of affective disorders compared to other psychiatric disorders in children and adolescents with 22q11.2 deletion syndrome. J Affect Disord. 2011 doi: 10.1016/j.jad.2010.11.025. [DOI] [PubMed] [Google Scholar]
- 5.Murphy KC, Jones LA, Owen MJ. High rates of schizophrenia in adults with velo-cardiofacial syndrome. Arch Gen Psychiatry. 1999;56(10):940–5. doi: 10.1001/archpsyc.56.10.940. [DOI] [PubMed] [Google Scholar]
- 6.Gothelf D, Feinstein C, Thompson T, et al. Risk factors for the emergence of psychotic disorders in adolescents with 22q11.2 deletion syndrome. Am J Psychiatry. 2007;164(4):663–9. doi: 10.1176/ajp.2007.164.4.663. [DOI] [PubMed] [Google Scholar]
- 7.Feinstein C, Eliez S, Blasey C, et al. Psychiatric disorders and behavioral problems in children with velocardiofacial syndrome: usefulness as phenotypic indicators of schizophrenia risk. Biol Psychiatry. 2002;51(4):312–8. doi: 10.1016/s0006-3223(01)01231-8. [DOI] [PubMed] [Google Scholar]
- 8.Elzinga BM, Roelofs K, Tollenaar MS, et al. Diminished cortisol responses to psychosocial stress associated with lifetime adverse events: a study among healthy young subjects. Psychoneuroendocrinology. 2008;33:227–237. doi: 10.1016/j.psyneuen.2007.11.004. [DOI] [PubMed] [Google Scholar]
- 9.Beaton EA, Simon TJ. How might stress contribute to increased risk for schizophrenia in children with chromosome 22q11.2 deletion syndrome? J Neurodev Disord. 2011;3(1):68–75. doi: 10.1007/s11689-010-9069-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Schalock RL, Borthwick-Duffy SA, Bradley VJ, et al. Intellectual disability: Definition, classification, and systems of supports. American Association on Intellectual and Developmental Disabilities. 2010:259. doi: 10.1352/1944-7558-126.6.439. [DOI] [PubMed] [Google Scholar]
- 11.Meyers CE, Nihira K, Zetlin A. The measurement of adaptive behavior. Handbook of mental deficiency: Psychological theory and research. 1979;2:215–253. [Google Scholar]
- 12.Witt JC, Martens B. Adaptive behavior: Tests and assessment issues. School Psychology Review. 1984 [Google Scholar]
- 13.Sparrow SS, Balla DA, Cicchetti DV, et al. Vineland Adaptive Behavior Scales Interview Edition Expanded Form Manual. American Guidance Services, Inc.; Circle Pines, Minnesota: 1984. [Google Scholar]
- 14.Harrison P, Oakland T. Adaptive Behavior Assessment System-(ABAS–II) Psychological Corporation; San Antonio, TX: 2003. [Google Scholar]
- 15.Loveland KA, Kelley ML. Development of adaptive behavior in preschoolers with autism or Down syndrome. American Journal on Mental Retardation. 1991 [PubMed] [Google Scholar]
- 16.Statacorp, L. Intercooled Stata 9.2 for Windows. USA: 2005. [Google Scholar]
- 17.Wechsler D. Wechsler intelligence scale for children–Fourth edition (WISC-IV) The Psychological Corporation; San Antonio, TX: 2003. [Google Scholar]
- 18.Kamphaus R, Reynolds C. BASC-2 behavioral and emotional screening system. Pearson; Minneapolis, MN: 2007. [Google Scholar]
- 19.Nauta MH, Scholing A, Rapee RM, et al. A parent-report measure of children’s anxiety: Psychometric properties and comparison with child-report in a clinic and normal sample. Behaviour Research and Therapy. 2004;42(7):813–839. doi: 10.1016/S0005-7967(03)00200-6. [DOI] [PubMed] [Google Scholar]
- 20.Spence SH, Barrett PM, Turner CM. Psychometric properties of the Spence Children’s Anxiety Scale with young adolescents. J Anxiety Disord. 2003;17(6):605–625. doi: 10.1016/s0887-6185(02)00236-0. [DOI] [PubMed] [Google Scholar]
- 21.Verhulst FC. Community and epidemiological aspects of anxiety disorders in children. Cambridge University Press; New York: 2001. [Google Scholar]
- 22.Young AS, Shashi V, Schoch K, et al. Discordance in Diagnoses and Treatment of Psychiatric Disorders in Children and Adolescents with 22q11.2 Deletion Syndrome. Asian J Psychiatr. 2011;4(2):119–124. doi: 10.1016/j.ajp.2011.03.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Myers BA, Pueschel SM. Psychiatric disorders in persons with Down syndrome. J Nerv Ment Dis. 1991;179(10):609–13. doi: 10.1097/00005053-199110000-00004. [DOI] [PubMed] [Google Scholar]
- 24.Tranfaglia MR. The psychiatric presentation of fragile x: evolution of the diagnosis and treatment of the psychiatric comorbidities of fragile X syndrome. Dev Neurosci. 2011;33(5):337–48. doi: 10.1159/000329421. [DOI] [PubMed] [Google Scholar]
- 25.Visootsak J, Graham JM., Jr. Klinefelter syndrome and other sex chromosomal aneuploidies. Orphanet J Rare Dis. 2006;1:42. doi: 10.1186/1750-1172-1-42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Tartaglia NR, Howell S, Sutherland A, et al. A review of trisomy X (47,XXX) Orphanet J Rare Dis. 2010;5:8. doi: 10.1186/1750-1172-5-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Feldhusen JF, Klausmeier HJ. Anxiety, intelligence, and achievement in children of low, average, and high intelligence. Child Dev. 1962;33:403–9. [PubMed] [Google Scholar]
- 28.Niditch LA, Varela RE, Kamps JL, et al. Exploring the association between cognitive functioning and anxiety in children with autism spectrum disorders: the role of social understanding and aggression. J Clin Child Adolesc Psychol. 2012;41(2):127–37. doi: 10.1080/15374416.2012.651994. [DOI] [PubMed] [Google Scholar]
- 29.Krug MK, Carter CS. Adding fear to conflict: A general purpose cognitive control network is modulated by trait anxiety. Cognitive, Affective, & Behavioral Neuroscience. 2010;10(3):357–371. doi: 10.3758/CABN.10.3.357. [DOI] [PubMed] [Google Scholar]
- 30.Essex MJ, Shirtcliff EA, Burk LR, et al. Influence of early life stress on later hypothalamic-pituitary-adrenal axis functioning and its covariation with mental health symptoms: a study of the allostatic process from childhood into adolescence. Dev Psychopathol. 2011;23(4):1039–58. doi: 10.1017/S0954579411000484. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Roy AK, Vasa RA, Bruck M, et al. Attention bias toward threat in pediatric anxiety disorders. J Am Acad Child Adolesc Psychiatry. 2008;47(10):1189–96. doi: 10.1097/CHI.0b013e3181825ace. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Tien AY, Eaton WW. Psychopathologic precursors and sociodemographic risk factors for the schizophrenia syndrome. Arch Gen Psychiatry. 1992;49(1):37–46. doi: 10.1001/archpsyc.1992.01820010037005. [DOI] [PubMed] [Google Scholar]
- 33.Huppert JD, Smith TE. Anxiety and schizophrenia: the interaction of subtypes of anxiety and psychotic symptoms. CNS Spectr. 2005;10(9):721–31. doi: 10.1017/s1092852900019714. [DOI] [PubMed] [Google Scholar]
- 34.Arnsten AFT. Stress signalling pathways that impair prefrontal cortex structure and function. Nat Rev Neurosci. 2009;10(6):410–422. doi: 10.1038/nrn2648. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Pine DS. Integrating research on development and fear learning: a vision for clinical neuroscience? Depress Anxiety. 2009;26(9):775–9. doi: 10.1002/da.20595. [DOI] [PubMed] [Google Scholar]
- 36.Jolin EM, Weller RA, Weller EB. Psychosis in children with velocardiofacial syndrome (22q11.2 deletion syndrome) Curr Psychiatry Rep. 2009;11(2):99–105. doi: 10.1007/s11920-009-0016-y. [DOI] [PubMed] [Google Scholar]
- 37.Sobin C, Kiley-Brabeck K, Daniels S, et al. Neuropsychological characteristics of children with the 22q11 Deletion Syndrome: a descriptive analysis. Child Neuropsychol. 2005;11(1):39–53. doi: 10.1080/09297040590911167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Baker KD, Skuse DH. Adolescents and young adults with 22q11 deletion syndrome: psychopathology in an at-risk group. Br J Psychiatry. 2005;186:115–20. doi: 10.1192/bjp.186.2.115. [DOI] [PubMed] [Google Scholar]
- 39.Stoddard J, Niendam T, Hendren R, et al. Attenuated positive symptoms of psychosis in adolescents with chromosome 22q11.2 deletion syndrome. Schizophr Res. 2010;118(1-3):118–21. doi: 10.1016/j.schres.2009.12.011. [DOI] [PMC free article] [PubMed] [Google Scholar]