

Abstract
Introduction:
Youths with a minority sexual orientation (i.e., gay, lesbian, bisexual, and mostly heterosexual) are at high risk for cigarette smoking. We examined sexual-orientation disparities in smoking during adolescence and emerging adulthood and investigated the role of age at first smoking in contributing to smoking disparities.
Methods:
We used data from the Growing Up Today Study, a large longitudinal cohort of adolescents followed from ages 12 to 24 years (N = 13,913). Self-administered questionnaires filled out annually or biennially assessed age at first smoking, current smoking, frequency of smoking, number of cigarettes smoked daily, and nicotine dependence. Proportional hazards survival analysis and repeated measures regression estimated sexual-orientation differences in smoking.
Results:
Compared with completely heterosexuals, lesbian/gay, bisexual, and mostly heterosexual youths smoked their first cigarette at younger ages, were more likely to be current smokers, and had higher frequency of smoking. Among past-year smokers, sexual-minority females smoked more cigarettes daily and scored higher on nicotine dependence than completely heterosexual females. In some instances, gender and age modified relationships between sexual orientation and smoking, with relative risk accentuated in female sexual minorities and in sexual minorities during younger ages. Younger age of smoking onset contributed to elevated smoking in mostly heterosexuals and bisexuals, and to a lesser extent in lesbians, but not in gay males.
Conclusions:
Sexual-orientation minorities are at greater risk for smoking during adolescence and emerging adulthood than heterosexuals. Disparities are larger in females and evident in early adolescence. Prevention and cessation efforts should target this population, preferably beginning in early adolescence.
Introduction
Accumulating evidence has established that youths with minority sexual orientations (e.g., those who identify as lesbian, gay or bisexual [LGB] or experience same-sex attractions and/or relationships) are more likely than heterosexual youths to smoke cigarettes (J. G. Lee, Griffin, & Melvin, 2009) and that negative health effects, such as increased risk for acute respiratory infections, are apparent in young adulthood (Blosnich, Jarrett, & Horn, 2010). Although most studies investigating sexual-orientation disparities in youth smoking have relied on cross-sectional data, a few studies with longitudinal designs have been published with the advantage of being able to look at differences over time (Easton, Jackson, Mowery, Comeau, & Sell, 2008; Marshal, Friedman, Stall, & Thompson, 2009; Talley, Sher, & Littlefield, 2010). In one assessment using data from the first two waves of the school-based National Longitudinal Study of Adolescent Health (Add Health), Easton et al. (2008) found that adolescents reporting sexual attractions to or relationships with both males and females, but not same-sex-only attractions/relationships, were more likely than adolescents reporting only opposite-sex attractions/relationships to have smoked in the past month at the beginning of the study as well as to become smokers at follow-up 1 year later.
In another study using three waves of Add Health data spanning 8 years, sexual-minority youths had higher frequency of cigarette smoking at the beginning of the study and faster increases in smoking frequency over time, compared with heterosexuals (Marshal et al., 2009). Notable differences were observed by sexual-orientation subgroup. Mostly heterosexual and bisexual youths had higher smoking frequency initially, but similar increases in smoking frequency over time, when compared with heterosexual youths. Lesbian/gay youths were similar to heterosexual youths in their initial smoking frequency, but had a faster increase in smoking frequency over time. Similarly, findings from a longitudinal study of college students revealed that minority sexual orientation was associated with higher frequency of cigarette smoking at the beginning of the study (Talley et al., 2010). However, in contrast to Marshal and colleagues, heterosexual and sexual-minority participants had similar patterns of changes in smoking over time. This divergence may be attributable to study differences such as age (adolescence vs. emerging adulthood).
Despite advances in the use of longitudinal designs, additional research is necessary to identify sexual-minority subgroups that are most at risk for smoking. Gender has been identified as a modifier of the relationship between sexual orientation and substance use, with sexual-minority females displaying great or similar substance use compared with sexual-minority males (Corliss, Rosario, Wypij, Fisher, & Austin, 2008; Corliss et al., 2010; Hahm, Wong, Huang, Ozonoff, & Lee, 2008; Marshal et al., 2008). In contrast, studies with general youth samples typically find that males are more likely to smoke than females (Nelson et al., 2008). Some evidence suggests that age may also be an important modifier, with sexual-orientation disparities greater during adolescence compared with emerging adulthood (Corliss et al., 2010). However, not all studies have found larger disparities during adolescence. A study of Asian Americans and Pacific Islanders found sexual-orientation disparities in substance use appeared during emerging adulthood, but not in adolescence (Hahm et al., 2008).
An additional consideration is that prospective studies of adolescents have not examined sexual-orientation differences in age at first smoking or its contribution to disparities in subsequent cigarette use. Evidence from a cross-sectional high-school study suggests that sexual minorities begin smoking at younger ages (Garofalo, Wolf, Kessel, Palfrey, & DuRant, 1998). Because younger age at initiation is an important predictor of later smoking (Breslau & Peterson, 1996; Taioli & Wynder, 1991), nicotine dependence (Breslau, Fenn, & Peterson, 1993), and cigarette-associated morbidity (Hegmann et al., 1993), it is important to understand whether sexual minorities begin smoking at younger ages than heterosexuals and the extent that such differences contribute to disparities in smoking and smoking-related morbidity throughout the life course.
To improve understanding of how sexual orientation is related to smoking disparities during adolescence and emerging adulthood, we analyzed data from the Growing Up Today Study (GUTS), a large ongoing cohort that assessed participants’ sexual orientation and cigarette use on multiple waves of data collection. The current study builds on an earlier cross-sectional analysis of GUTS data that found that lesbian/bisexual and mostly heterosexual girls and mostly heterosexual boys were more likely to smoke than their same-sex heterosexual peers (Austin et al., 2004). Advantages of the present study are the ability to separate bisexuals from lesbian/gay respondents and to conduct a more detailed examination of how gender, developmental effects of adolescence versus emerging adulthood, and age at smoking initiation influence sexual-orientation disparities in longitudinal smoking patterns. Study objectives were to: estimate sexual-orientation differences in cigarette smoking occurring during adolescence and emerging adulthood (ages 12–24 years), examine how gender and age modify sexual-orientation disparities in smoking, and estimate the contribution of sexual-orientation differences in age at first smoking to sexual-orientation disparities in subsequent smoking.
Methods
Study Sample
The GUTS is a U.S. community-based longitudinal cohort of 9,039 females and 7,843 males begun in 1996 when participants were ages 9–14 years. Participants are children of Nurses’ Health Study II participants and 93% self-identified as non-Hispanic White. Because enrollment occurred through mothers, GUTS contains siblings. Since the study’s inception, participants have been assessed annually or biennially through self-administered pencil-and-paper or web-based questionnaires. More information about the study, including enrollment procedures, is elsewhere (Field et al., 1999). The Brigham and Women’s Hospital Institutional Review Board approved this study.
The current analysis is comprised of GUTS participants who provided information on sexual orientation and smoking in one or more assessments through 2005 (82.4% of the original cohort; 7,988 females and 5,925 males). Compared with participants included in the analysis, participants excluded from analysis were more likely to be male (24.5% males excluded vs. 11.6% females; p < .0001), to be from the Northeast (18.3% excluded; p = .0003), South (18.4%; p = .001), or the Midwest (17.8%; p = .002) compared with the West coast (14.6%); and to be older at baseline (mean age 11.8 vs. 11.5 years; p < .0001). No differences in race/ethnicity (p = .69) or baseline smoking status (p = .29) were found between those included and excluded from analysis.
Measures
Sexual Orientation
Sexual orientation was gathered through the question: “Which of the following best describes your feelings? (1) completely heterosexual (attracted to persons of the opposite sex), (2) mostly heterosexual, (3) bisexual (equally attracted to men and women), (4) mostly homosexual, (5) completely homosexual (gay/lesbian, attracted to persons of the same sex), (6) not sure.” The “mostly homosexual” and “completely homosexual” responses were collapsed into a lesbian/gay category because sample sizes in these categories were too small to keep separate. “Not sure” responses were excluded because of their small sample size and concentration at the younger ages. Sexual orientation was assessed in 1999, 2001, 2003, and 2005.
Smoking Outcomes
Four cigarette smoking behavior items adapted from the Massachusetts Youth Risk Behavior Survey (Massachusetts Department of Education, 1993) and the California Tobacco Control Program (Pierce et al., 1994) were used. To assess age at first smoking, participants were asked to indicate whether and at what age they first tried cigarettes. Response options ranged from younger than 8 years to the maximum age of participants at each wave; therefore, the variable ranged from 7 to 24 years. Repeated measures responses for the remaining four smoking variables were assessed on waves 1998, 1999, 2001, 2003, and 2005. Current smoking was defined as smoking in the past month (binary variable, yes vs. no). Average frequency of smoking in the past year was coded as an ordinal variable: never smoking (0), smoking less than monthly (1), smoking less than weekly, but greater than monthly (2), smoking weekly (3), or smoking daily (4). Number of cigarettes smoked daily was assessed with the question, “When you are smoking, how many cigarettes do you smoke in one day?” Response options were don’t smoke/<1, 1, 2–5, 6–10, 11–20, and 21 or more. In analyses, we assigned the value 0 to the lowest option, the midpoint value to response options with ranges (e.g., 3.5 for the 2–5 response option), and the value 21 to the “21 or more” option and treated this outcome as a continuous variable.
Nicotine dependence was assessed with a previously validated modified version of the Fagerström Tolerance Questionnaire (mFTQ) consisting of five questions: frequency of smoking more in the morning, frequency of smoking when sick, difficulty not smoking where it is forbidden, depth of inhalation, and time to first cigarette after waking (Rojas, Killen, Haydel, & Robinson, 1998). Responses were summed and scores ranged from 5 to 25. Good test–retest reliability and validity of the mFTQ has been established (Rojas et al., 1998). Cronbach’s alpha for the GUTS cohort ranged from 0.71 to 0.78 across waves.
Statistical Analyses
We conducted longitudinal descriptive analyses to investigate sexual-orientation patterns in cigarette smoking during adolescence and emerging adulthood. Statistical methods varied by outcome. For age at first smoking, we used proportional hazards survival analysis and the robust sandwich covariance matrix to adjust SEs to account for nonindependent sibling clusters to estimate hazard ratios (HR) and 95% CI (E. Lee, Wei, & Amato, 1992). In these models, we used the respondents’ last report of their sexual orientation. A sensitivity analysis showed that associations of sexual orientation with age at first smoking were similar whether first or last report of sexual orientation was used in statistical models.
For the other outcomes, we used generalized estimating equations to estimate the average effect size over the repeated measures and to account for the nonindependence of the repeated measures within an individual and the sibling clusters (Liang & Zeger, 1986). These analyses were restricted to responses occurring when participants were between the ages of 12 and 24 years. Sexual orientation and smoking outcomes were updated at each wave reported to allow for changes over time to be modeled. To model current smoking, we estimated risk ratios using the modified Poisson method (Zou, 2004). Ordinal logistic regression was used to estimate ORs for past-year frequency of smoking and linear regression was used to estimate beta coefficients for average number of cigarettes smoked daily and nicotine dependence. Because number of cigarettes smoked daily could be considered an ordered categorical variable, we conducted confirmatory analyses using ordinal logistic regression. As findings were comparable with the linear models, we present the linear regression results only. Models estimating number of cigarettes smoked daily and nicotine dependence were restricted to respondents who had smoked in the past year and age-standardized means were also calculated.
Statistical models adjusted for potential confounding by age, race/ethnicity (non-Hispanic White vs. other), region of residence, and the presence of a parent or sibling in the household who smoked. Completely heterosexuals served as the reference. Statistical significance was set at the p < .05 criterion. Because of the documented gender differences in smoking (Nelson et al., 2008), we stratified models on gender to estimate sexual orientation differences in smoking for each gender separately. To test formally whether gender was an effect modifier in the relationship between sexual orientation and smoking, we also constructed statistical models that included both genders and sexual-orientation-by-gender interaction terms. In gender-stratified models, we examined effect modification by age by including sexual-orientation-by-age interaction terms.
To examine if age at first smoking mediated relationships between sexual orientation and smoking, we compared sexual-orientation-specific estimates from models that included (mediation models) and excluded (base models) age at first smoking to assess for changes in model parameter estimates. We calculated the mediation proportion and its associated p value (Lin, Fleming, & De Gruttola, 1997) using the publicly available Mediate macro available at: http://www.hsph.harvard.edu/faculty/donna-spiegelman/software/mediate/index.html. The mediation proportion is the proportion of excess smoking by sexual minorities relative to same-gender heterosexuals attributable to sexual minorities’ younger age at first smoking. For these models, younger age at first smoking was categorized as occurring by age 15 years and analyses were restricted to responses at age 15 years or older to account for temporal ordering. Sensitivity analyses comparing findings using first smoking by ages 13 and 14 resulted in similar conclusions (data not shown).
Results
Among males, based on last report of sexual orientation, 92.5% (n = 5,473) were completely heterosexual, 5.0% (n = 297) were mostly heterosexual, 0.7% (n = 39) were bisexual, and 1.9% (n = 110) were gay. Among females, based on last report of sexual orientation, 85.8% (n = 6,839) were completely heterosexual, 11.1% (n = 887) were mostly heterosexual, 2.1% (n = 164) were bisexual, and 1.1% were lesbian (n = 84).
Age at First Smoking Cigarettes
Cumulative incidence plots of age at first smoking are shown in Figure 1. Among males, mostly heterosexual (HR = 1.35; 95% CI = 1.17–1.56), bisexual (HR = 1.84; 95% CI = 1.30–2.61), and gay (HR = 1.25; 95% CI = 1.01–1.54) participants reported smoking their first cigarette at younger ages than completely heterosexuals. Among females, mostly heterosexuals (HR = 1.79; 95% CI = 1.64–1.95), bisexuals (HR = 2.31; 95% CI = 1.95–2.75), and lesbians (HR = 1.53; 95% CI = 1.19–1.97) reported first smoking at younger ages compared with completely heterosexuals. In a model examining gender-by-sexual-orientation interactions, the overall Wald chi-square testing the interaction indicated that sexual-minority females had a significantly younger age at first smoking than completely heterosexual females relative to differences between sexual minority and completely heterosexual males (p = .002). Although the magnitude and direction of the gender-by-sexual-orientation parameter estimates were similar for all sexual-minority subgroups, statistically significant differences were found among mostly heterosexuals only (p = .0001).
Figure 1.
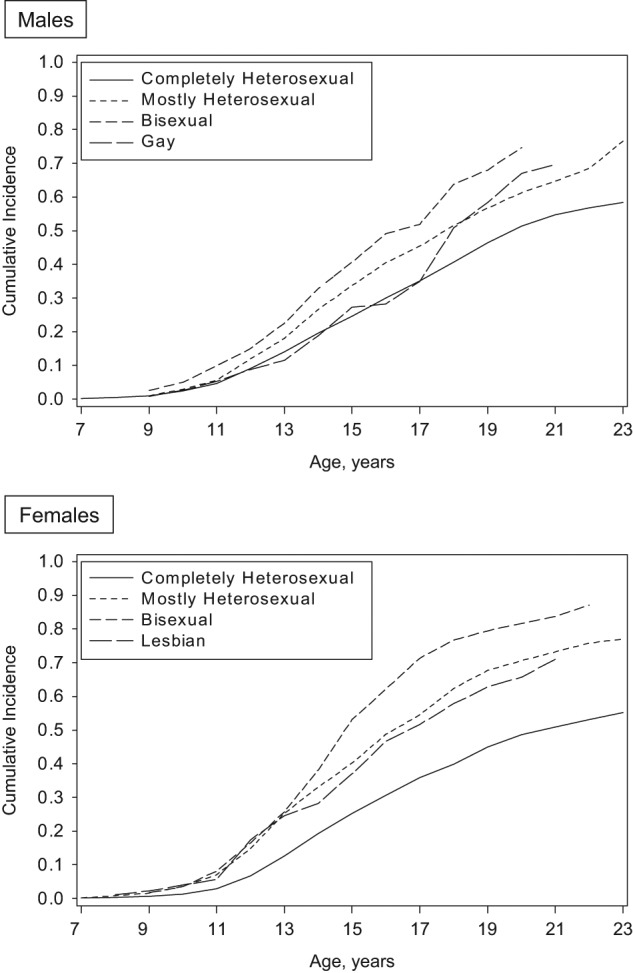
Cumulative incidence of age of first smoking cigarettes by sexual orientation among male and female participants in the Growing Up Today Study (1996–2005).
Current Smoking and Frequency of Smoking
The percent of the cohort reporting past-month smoking and daily smoking in the past year for each age group by gender and sexual orientation is shown in Figure 2. In statistical models accounting for confounding, sexual-minority males had approximately 60% greater risk and sexual-minority females had twice the risk of being a current smoker during adolescence and emerging adulthood than completely heterosexuals of the same gender (Table 1). Frequency of smoking was also higher among sexual-minority males and females (Table 1).
Figure 2.

Cigarette smoking by sexual orientation during adolescence and emerging adulthood among male and female participants in the Growing Up Today Study (1998–2005).
Table 1.
Comparisons of Sexual Minority Versus Completely Heterosexual Youths in Cigarette Smoking Outcomes by Gender Among Participants in the Growing Up Today Study During Ages 12 Through 24 Years (1998–2005): Results of Repeated Measures Regression
| Mostly heterosexual | Bisexual | Gay/lesbian | ||
| Smoking outcomes | No. of obs | |||
| Males | ||||
| Past-month smoking, RR (95% CI) | 19,468 | 1.64 (1.43, 1.88)** | 1.66 (1.22, 2.28)* | 1.57 (1.28, 1.94)** |
| Frequency of smoking, OR (95% CI) | 18,689 | 2.10 (1.75, 2.52)** | 2.57 (1.63, 4.06)** | 2.08 (1.49, 2.91)** |
| Number of cigarettes daily, β (95% CI)a | 3,903 | 0.40 (−0.24, 1.03) | 0.76 (−1.27, 2.79) | 0.04 (−1.14, 1.22) |
| Nicotine dependence score, β (95% CI)a | 3,894 | 0.34 (−0.04, 0.71) | 0.83 (−0.68, 2.34) | 0.03 (−0.68, 0.74) |
| Females | ||||
| Past-month smoking, RR (95% CI) | 30,281 | 1.96 (1.82, 2.12)** | 2.62 (2.31, 2.97)** | 2.12 (1.70, 2.64)** |
| Frequency of smoking, OR (95% CI) | 29,290 | 2.67 (2.39, 2.97)** | 5.23 (4.17, 6.58)** | 3.99 (2.68, 5.95)** |
| Number of cigarettes daily, β (95% CI)a | 7,036 | 0.96 (0.62, 1.31)** | 2.03 (1.24, 2.83)** | 2.04 (0.62, 3.45)** |
| Nicotine dependence score, β (95% CI)a | 6,994 | 0.77 (0.52, 1.01)** | 2.03 (1.47, 2.60)** | 1.30 (0.26, 2.34)** |
Note. aRestricted to past-year smokers.
RR = relative risk, β = parameter estimate. Repeated measures regression models adjusted for age, race/ethnicity, region of residence, and presence of a household family member who smokes. Referent group is completely heterosexual.
*p < .01. **p < .0001.
Models examining gender-by-sexual-orientation interactions revealed that prevalence of current smoking (Wald chi-square for interaction p = .04) and frequency of smoking (Wald chi-square for interaction p = .006) was accentuated in sexual-minority females. Bisexual females were much more likely than completely heterosexual females to be a current smoker (p = .01) and to smoke more frequently (p = .008) relative to differences between bisexual and completely heterosexual males. Compared with difference among gay and completely heterosexual males, lesbians had a higher frequency of smoking than completely heterosexual females (p = .04).
Gender-stratified models examining interactions of sexual orientation with age showed that risk of current smoking was amplified among younger sexual minorities compared with completely heterosexuals (Wald chi-square for interaction for both genders p < .0001) and that the frequency of smoking was amplified among younger sexual-minority females (Wald chi-square for interaction p = .002) and males, but the interaction for males was not statistically significant (p = .13). Sexual-orientation-by-age interactions for current smoking were significant for gay males (p = .0008) and lesbians (p = .005), mostly heterosexuals males (p = .001) and females (p < .0001), and bisexual females (p < .0001). Sexual-orientation-by-age interactions in frequency of smoking were significant for bisexual females (p = .003) and lesbians (p = .04).
Average Number of Cigarettes Smoked Daily and Nicotine Dependence Among Past-Year Smokers
Among females who reported smoking in the past year, lesbians (age-standardized mean = 2.1 cigarettes), bisexuals (2.8), and mostly heterosexuals (1.5) smoked more cigarettes daily than completely heterosexual females (0.6; Table 1). Lesbians (age-standardized mean = 8.9), bisexual (10.0), and mostly heterosexual females (8.7) also scored higher on nicotine dependence than completely heterosexual females (8.0; Table 1). Gay (age-standardized mean = 1.7 cigarettes; dependence score = 9.1), bisexual (1.6 cigarettes; dependence score = 9.0), and mostly heterosexual (1.3 cigarettes; dependence score = 8.7) males did not differ significantly from completely heterosexual males (0.7 cigarettes; dependence score = 8.5) in the number of cigarettes smoked daily or on nicotine dependence respectively (Table 1). Although difference between sexual-minority and completely heterosexual females on number of cigarettes smoked daily and nicotine dependence were larger than differences among sexual-minority and completely heterosexual males, sexual-orientation-by-gender interactions were not statistically significant. Age was not a statistically significant modifier of associations between sexual orientation and number of cigarettes smoked daily or nicotine dependence.
Influence of Younger Age at First Smoking Cigarettes on Sexual-Orientation Differences in Smoking
Analyses conducted to estimate the contribution of younger age at first smoking to sexual-orientation disparities in subsequent smoking showed evidence of mediation in some instances (Table 2). Among mostly heterosexual males, the estimated proportion of excess smoking attributable to younger age at first smoking ranged from 24% to 48% across the four smoking outcomes. Among bisexual males, the proportion of excess smoking due to younger age at first smoking was more modest (37% for current smoking and 20% for frequency of smoking). In contrast, younger age at first smoking did not mediate smoking disparities in gay males. Among mostly heterosexual females, the estimated proportion of excess smoking attributable to younger age at first smoking ranged from 20% to 36% across the four smoking outcomes. Among bisexual females, the proportion of excess smoking due to younger age at first smoking was larger for current smoking (37%) and frequency of smoking (25%) than for number of cigarettes smoked daily (10%) and nicotine dependence (7%). Among lesbians, younger age at first smoking significantly mediated current smoking (22%), but not the other smoking outcomes.
Table 2.
Results of Analyses Testing the Mediating Effects of Age at First Smoking Cigarettes on Differences Between Sexual Minority and Completely Heterosexual Youths in Smoking Outcomes by Gender Among Participants (≥age 15 years) in the Growing Up Today Study (1998–2005)
| Mostly heterosexual | Bisexual | Gay/lesbian | |||||||
| Smoking outcomes | Base model | Mediation model | Mediation % (p value) | Base model | Mediation model | Mediation % (p value) | Base model | Mediation model | Mediation % (p value) |
| Males | |||||||||
| Past-month smoking, OR (95% CI) | 1.56 (1.37, 1.78) | 1.39 (1.22, 1.58) | 26.2 (.0003) | 1.65 (1.21, 2.25) | 1.37 (1.01, 1.84) | 37.3 (.017) | 1.57 (1.27, 1.93) | 1.56 (1.23, 1.97) | 1.6 (.91) |
| Frequency of smoking, OR (95% CI) | 2.04 (1.25, 3.35) | 1.72 (1.42, 2.08) | 24.0 (.41) | 2.62 (1.82, 3.78) | 2.17 (1.37, 3.42) | 19.9 (.47) | 2.02 (1.81, 2.26) | 2.05 (1.46, 2.87) | NA |
| Number of cigarettes daily, β (95% CI)a | 0.37 (−0.30, 1.05) | 0.20 (−0.46, 0.86) | 47.5 (.29) | 0.75 (−1.40, 2.90) | 0.75 (−1.37, 2.87) | NA | −0.25 (−1.37, 0.87) | 0.03 (-1.08, 1.13) | NA |
| Nicotine dependence score, β (95% CI)a | 0.35 (−0.05, 0.74) | 0.25 (−0.14, 0.64) | 27.9 (.15) | 0.83 (−0.77, 2.44) | 0.84 (−0.72, 2.41) | NA | −0.15 (−0.83, 0.52) | 0.00 (-0.69, 0.70) | NA |
| Females | |||||||||
| Past-month smoking, OR (95% CI) | 1.94 (1.80, 2.09) | 1.53 (1.43, 1.64) | 35.5 (<.0001) | 2.50 (2.22, 2.83) | 1.78 (1.58, 2.00) | 37.2 (<.0001) | 2.14 (1.72, 2.66) | 1.80 (1.47, 2.20) | 22.3 (.007) |
| Frequency of smoking, OR (95% CI) | 2.73 (2.14, 3.48) | 2.03 (1.81, 2.27) | 29.6 (.002) | 5.23 (3.47, 7.89) | 3.43 (2.72, 4.34) | 25.4 (.026) | 4.03 (3.69, 4.42) | 3.73 (2.48, 5.61) | 5.7 (.71) |
| Number of cigarettes daily, β (95% CI)a | 0.96 (0.60, 1.32) | 0.76 (0.40, 1.11) | 21.2 (<.0001) | 2.08 (1.25, 2.90) | 1.87 (1.07, 2.68) | 10.0 (.006) | 2.10 (0.66, 3.53) | 1.99 (0.61, 3.37) | 5.0 (.37) |
| Nicotine dependence score, β (95% CI)a | 0.76 (0.51, 1.01) | 0.61 (0.36, 0.86) | 19.5 (<.0001) | 2.04 (1.46, 2.62) | 1.89 (1.33, 2.45) | 7.1 (.004) | 1.34 (0.28, 2.41) | 1.27 (0.23, 2.31) | 5.6 (.39) |
Note. aRestricted to past-year smokers.
Mediation % is the excess smoking attributable to younger age at first smoking. β = regression parameter estimate, NA indicates that mediation is not supported. Base models adjusted for age, race/ethnicity, region of residence, and presence of a household family member who smokes. Mediation models adjust for variables in the base model and age at first smoking cigarettes. Referent is completely heterosexual.
Discussion
Similar to prior longitudinal studies (Easton et al., 2008; Marshal et al., 2009; Talley et al., 2010), this prospective study found large disparities in cigarette smoking during adolescence and emerging adulthood among sexual-minority compared with completely heterosexual youths. Sexual minorities of both genders had elevated risk of being current smokers and elevated frequency of smoking. In analyses restricted to past-year smokers, females of all minority-sexual-orientation groups, but not males, smoked a greater number of cigarettes per day on average and scored higher on nicotine dependence than completely heterosexuals of their same gender.
In our study, age was an important modifier of relationships between sexual orientation and current smoking and smoking frequency. When age modified these relationships, sexual-orientation disparities were larger during younger ages. In support of these findings, a community sample of LGB youths (ages 14–21 years) found that younger participants were more likely to smoke than older ones (Rosario, Schrimshaw, & Hunter, 2010). Because younger adolescents have less developed coping skills than older youths, they may be especially vulnerable to adopting unhealthy coping methods, such as smoking, in attempts to handle life’s stressors (Rosario & Schrimshaw, in press). These findings underscore the importance of conducting research with younger sexual-minority adolescents, as vulnerability during this developmental period may be heightened. Because we had data from ages 12–24 years, we could examine age effects. This is an important contribution in light of the barriers to conducting studies with young sexual-minority adolescents (e.g., parental consent requirements; Mustanski, 2011).
Researchers have speculated that sexual minorities may be more likely than heterosexuals to smoke cigarettes in order to cope with negative feelings related to having a sexual orientation that is socially stigmatized. Studies with community samples of LGB adolescents and emerging adults have shown that rejection due to minority sexual orientation is associated with greater risk of smoking (Rosario, Schrimshaw, & Hunter, 2009), drug use, and substance problems (Ryan, Huebner, Diaz, & Sanchez, 2009). A qualitative study (modal age of 18–20 years) examining why LGB youths smoke identified stress, “fitting in,” and peer pressure as reasons (Remafedi, 2007). Participants emphasized that youth believed smoking reduces stress, facilitates bonding with peers, and distracts from problems. However, in another study of LGB youths (ages 14–21 years) smokers reported experiencing more stressful life events than nonsmokers, and smoking did not buffer (it actually amplified) relationships between stressful events and depressive or anxious distress (Rosario et al., 2010). This study also highlighted the important role of positive support from family and friends, as high levels of support reduced the magnitude of the association between smoking and distress.
As has been found in other studies examining sexual orientation and substance use in youth (Corliss et al., 2008; 2010; Hahm et al., 2008; Marshal et al., 2008), differences in smoking between sexual-minority and heterosexual females were larger than differences between sexual-minority and heterosexual males. Reasons why some sexual-minority females are especially vulnerable to substance use are currently speculative, and thus should be a focus of future research. Although all sexual-minority youths are at risk of experiencing stress due to their stigmatized sexual orientation, it is possible that females may attempt to cope with this stress in different ways than males and may be more likely to smoke cigarettes as a means to handle stress. It is also possible that factors associated with identity development as a sexual minority, such as gender expression, may contribute as some sexual-minority women may seek to express a masculine role presentation through smoking and other substance use behaviors (Hahm et al., 2008; Rosario, Schrimshaw, & Hunter, 2008). Future research should test these and other possible mechanisms in studies containing heterosexual and sexual-minority youths recruited through methodologically rigorous sampling strategies (Corliss, Cochran, & Mays, 2009).
Our data revealed that youths of all minority sexual orientations were more likely to smoke their first cigarette at younger ages than completely heterosexuals. Younger age at first smoking accounted for a significant proportion of disparities in subsequent smoking during the adolescent and emerging adulthood periods for mostly heterosexuals and bisexuals of both genders and to a lesser extent for lesbians, but not for gay males. These findings suggest that there may be heterogeneity across sexual-orientation subgroups and gender in the degree that age at initiation contributes to smoking disparities. These findings also indicate that factors other than age at smoking initiation may be more salient in explaining disparities among gay males and lesbians compared with bisexuals and mostly heterosexuals. One possible explanation is that gay men and lesbians may be more involved in the LGB community than bisexuals and mostly heterosexuals and thus have greater exposure to factors within the community that are conducive to smoking such as greater exposure to smokers and social settings where smoking occurs (e.g., pride events). Lesbians and gay males in GUTS reported greater involvement in the LGB community than bisexuals and mostly heterosexuals, and involvement in LGB social activities was associated with higher risk for drug use (Corliss, Rosario, Wypij, Frazier, & Austin, 2007). It is possible that the influence of identity development as a sexual minority (Rosario, Schrimshaw, & Hunter, 2004) on risk for smoking is larger in lesbian/gay compared with other sexual-minority subgroups.
Some limitations should be noted. GUTS is not a representative probability sample and is comprised of mostly non-Hispanic Whites whose mothers have nursing degrees. Thus, generalizability is limited and findings are likely more applicable to White youth from middle-class backgrounds. However, findings with respect to sexual orientation are less biased than findings from studies that recruit participants through the LGB community. A possible source of bias is that information is based on self-reports. If accuracy of reporting smoking is related to sexual orientation, then estimates may be biased; for example, if those disclosing a minority sexual orientation are also more likely to disclose other potentially stigmatizing information, such as smoking, then differences between sexual-minority and heterosexual youths may be inflated. Some analyses (e.g., those examining effect modification and restricted to past-year smokers) were limited by low power in some of the sexual-minority groups with fewer observations (e.g., bisexual males). A final consideration is that mediation analyses, like those conducted in this study, are difficult to operationalize when the main predictor (i.e., sexual orientation) is a marker of developmental processes and experiences that occur overtime (Cass, 1996; Troiden, 1993) because temporal ordering is unclear. In this study, we hypothesized that experiences associated with minority-sexual-orientation development influenced youths to try smoking at earlier ages and that this in turn influenced sexual-orientation disparities in subsequent smoking. Despite limitations, findings from this large study are based on multiple annual or biennial assessments collected prospectively during the critical ages when smoking initiation and the development of smoking behaviors typically occurs.
Additional research is necessary to improve understanding of risk and protective factors for smoking in sexual-minority youth. Research to understand how intersecting factors such as race and ethnicity influence smoking patterns is also limited (J. G. Lee, Griffin, & Melvin, 2009). A recent study found that smoking was more prevalent in racial/ethnic minority (i.e., Black, Asian, Hispanic, multiracial) LGB college students compare with their heterosexual counterparts and that Black and Asian, but not Hispanic and multiracial, LGB students had lower prevalence of smoking than White LGB students (Blosnich, Jarrett, & Horn, 2011).
Attention to sexual-minority subgroup differences is also needed. When research combines all sexual minorities into one group, important heterogeneity may be masked. While a growing body of research has identified health disparities among youths describing themselves as mostly heterosexual (Corliss, Austin, Roberts, & Molnar, 2009; Homma, Chen, Poon, & Saewyc, 2011; Marshal et al., 2009), factors contributing to their greater smoking and how they may be similar to or different from other sexual minorities are poorly understood. Mostly heterosexual youth differ from other youth in their behavioral experiences and identity development (Austin, Conron, Patel, & Freedner, 2007; Thompson & Morgan, 2008). Thus, their experiences are important to consider because it allows for a more detailed understanding of the spectrum of sexual orientation. In sum, greater understanding of risk and protective factors as well as the influence of intersecting sociodemographics can aid in the development of interventions and policies to reduce smoking disparities in sexual-minority youth.
Sexual-minority adolescents are a population at risk for smoking and should be a focus of prevention and cessation efforts. Our findings suggest that prevention efforts that begin early, preferably in early adolescence or before, may have the potential to be most effective because large sexual-orientation disparities have already emerged by early adolescence. In addition, efforts that are able to successfully delay smoking initiation among sexual minorities may reduce disparities in youth cigarette smoking. Such efforts, if successful, also have the potential to reduce risk for other substance use and associated harmful repercussions as evidence suggests that nicotine exposure increases risk for other substance use (Levine et al., 2011). Efforts to reduce sexual-orientation disparities in smoking should focus on identifying successful ways to assist these youth in adopting healthy strategies for coping with stress and to enhance social support from their family and friends.
Funding
The GUTS cohort has been funded by the Robert Wood Johnson Foundation; grants HD45763, DK46834, and HL03533 from the National Institutes of Health ; and grant RSGPB-04-009-01-CPPB from the American Cancer Society. Dr. Corliss is supported by career development award DA23610 from the National Institute on Drug Abuse. Drs. Corliss and Austin are also supported by the Leadership Education in Adolescent Health Project, Maternal and Child Health Bureau, Health Resources and Services Administration grant 6T71-MC00009.
Declaration of Interests
None.
Acknowledgments
The authors would like to thank the participants of the Growing Up Today Study and the members of the Growing Up Today Study research team whose dedication made this study possible.
References
- Austin SB, Conron K, Patel A, Freedner N. Making sense of sexual orientation measures: Findings from a cognitive processing study with adolescents on health survey questions. Journal of LGBT Health Research. 2007;3:55–65. doi: 10.1300/j463v03n01_07. doi:10.1300/J463v03n01_07. [DOI] [PubMed] [Google Scholar]
- Austin SB, Ziyadeh N, Fisher LB, Kahn JA, Colditz GA, Frazier AL. Sexual orientation and tobacco use in a cohort study of US adolescent girls and boys. Archives of Pediatrics & Adolescent Medicine. 2004;158:317–322. doi: 10.1001/archpedi.158.4.317. doi:10.1001/archpedi.158.4.317. [DOI] [PubMed] [Google Scholar]
- Blosnich J, Jarrett T, Horn K. Disparities in smoking and acute respiratory illnesses among sexual minority young adults. Lung. 2010;188:401–407. doi: 10.1007/s00408-010-9244-5. doi:10.1007/s00408-010-9244-5. [DOI] [PubMed] [Google Scholar]
- Blosnich JR, Jarrett T, Horn K. Racial and ethnic differences in current use of cigarettes, cigars, and hookahs among lesbian, gay, and bisexual young adults. Nicotine & Tobacco Research. 2011;13:487–491. doi: 10.1093/ntr/ntq261. doi:10.1093/ntr/ntq261. [DOI] [PubMed] [Google Scholar]
- Breslau N, Fenn N, Peterson EL. Early smoking initiation and nicotine dependence in a cohort of young adults. Drug and Alcohol Dependence. 1993;33:129–137. doi: 10.1016/0376-8716(93)90054-t. doi:10.1016/0376-8716(93)90054-T. [DOI] [PubMed] [Google Scholar]
- Breslau N, Peterson EL. Smoking cessation in young adults: Age at initiation of cigarette smoking and other suspected influences. American Journal of Public Health. 1996;86:214–220. doi: 10.2105/ajph.86.2.214. doi:10.2105/AJPH.86.2.214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cass V. Sexual orientation identity formation: A Western phenomenon. In: Cabaj RP, Stein TS, editors. Textbook of homosexuality and mental health. Washington, DC: American Psychiatric Press, Inc; 1996. pp. 227–251. [Google Scholar]
- Corliss HL, Austin SB, Roberts AL, Molnar BE. Sexual risk in “mostly heterosexual” young women: Influence of social support and caregiver mental health. Journal of Women's Health (Larchmt) 2009;18:2005–2010. doi: 10.1089/jwh.2009.1488. doi:10.1089/jwh.2009.1488. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Corliss HL, Cochran SD, Mays VM. Sampling approaches to studying mental health concerns in the lesbian, gay, and bisexual community. In: Meezan W, Martin JI, editors. Handbook of research with gay, lesbian, bisexual, and transgender populations. New York: Routledge; 2009. pp. 131–158. [Google Scholar]
- Corliss HL, Rosario M, Wypij D, Fisher LB, Austin SB. Sexual orientation disparities in longitudinal alcohol use patterns among adolescents: Findings from the Growing Up Today Study. Archives of Pediatrics & Adolescent Medicine. 2008;162:1071–1078. doi: 10.1001/archpedi.162.11.1071. doi:10.1001/archpedi.162.11.1071. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Corliss HL, Rosario M, Wypij D, Frazier AL, Austin SB. Drug use and sexual orientation in a cohort study of U.S. youth. 2007. Paper presented at the 135th Annual Meeting of the American Public Health Association, Washington DC. [Google Scholar]
- Corliss HL, Rosario M, Wypij D, Wylie SA, Frazier AL, Austin SB. Sexual orientation and drug use in a longitudinal cohort study of U.S. adolescents. Addictive Behaviors. 2010;35:517–521. doi: 10.1016/j.addbeh.2009.12.019. doi:10.1016/j.addbeh.2009.12.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Easton A, Jackson K, Mowery P, Comeau D, Sell R. Adolescent same-sex and both-sex romantic attractions and relationships: Implications for smoking. American Journal of Public Health. 2008;98:462–467. doi: 10.2105/AJPH.2006.097980. doi:10.2105/AJPH.2006.097980. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Field AE, Camargo CA, Jr, Taylor CB, Berkey CS, Frazier AL, Gillman MW, et al. Overweight, weight concerns, and bulimic behaviors among girls and boys. Journal of the American Academy of Child and Adolescent Psychiatry. 1999;38:754–760. doi: 10.1097/00004583-199906000-00024. doi:10.1097/00004583-199906000-00024. [DOI] [PubMed] [Google Scholar]
- Garofalo R, Wolf RC, Kessel S, Palfrey SJ, DuRant RH. The association between health risk behaviors and sexual orientation among a school-based sample of adolescents. Pediatrics. 1998;101:895–902. doi: 10.1542/peds.101.5.895. doi:10.1542/peds.101.5.895. [DOI] [PubMed] [Google Scholar]
- Hahm HC, Wong FY, Huang ZJ, Ozonoff A, Lee J. Substance use among Asian Americans and Pacific Islanders sexual minority adolescents: Findings from the National Longitudinal Study of Adolescent Health. Journal of Adolescent Health. 2008;42:275–283. doi: 10.1016/j.jadohealth.2007.08.021. doi:10.1016/j.jadohealth.2007.08.021. [DOI] [PubMed] [Google Scholar]
- Hegmann KT, Fraser AM, Keaney RP, Moser SE, Nilasena DS, Sedlars M, et al. The effect of age at smoking initiation on lung cancer risk. Epidemiology. 1993;4:444–448. doi: 10.1097/00001648-199309000-00010. [DOI] [PubMed] [Google Scholar]
- Homma Y, Chen W, Poon CS, Saewyc EM. Substance use and sexual orientation among East and Southeast Asian adolescents in Canada. Journal of Child & Adolescent Substance Abuse. 2011;21:32–50. doi: 10.1080/1067828X.2012.636687. doi:10.1080/1067828x.2012.636687. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee E, Wei L, Amato D. Cox-type regression analysis for large numbers of small groups of correlated failure time observations. In: Klein JP, Goel PK, editors. Survival Analysis: State of the Art. Vol. 211. Amsterdam, The Netherlands: Kluwer Academic Publishers; 1992. pp. 237–247. [Google Scholar]
- Lee JG, Griffin GK, Melvin CL. Tobacco use among sexual minorities in the USA, 1987 to May 2007: A systematic review. Tobacco Control. 2009;18:275–282. doi: 10.1136/tc.2008.028241. doi:10.1136/tc.2008.028241. [DOI] [PubMed] [Google Scholar]
- Levine A, Huang YY, Drisaldi B, Griffin EA, Pollak DD, Xu S, et al. Molecular mechanism for a gateway drug: Epigenetic changes initiated by nicotine prime gene expression by cocaine. Science Translational Medicine. 2011;3:107–109. doi: 10.1126/scitranslmed.3003062. doi:10.1126/scitranslmed.3003062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liang K.-Y., Zeger SL. Longitudinal data analysis using generalized linear models. Biometrika. 1986;73:13–22. doi:10.1093/biomet/73.1.13. [Google Scholar]
- Lin DY, Fleming TR, De Gruttola V. Estimating the proportion of treatment effect explained by a surrogate marker. Statistics in Medicine. 1997;16:1515–1527. doi: 10.1002/(sici)1097-0258(19970715)16:13<1515::aid-sim572>3.0.co;2-1. doi:10.1002/(SICI)1097-0258(19970715)16:13<1515::AID-SIM572>3.0.CO;2–1. [DOI] [PubMed] [Google Scholar]
- Marshal MP, Friedman MS, Stall R, King KM, Miles J, Gold MA, et al. Sexual orientation and adolescent substance use: A meta-analysis and methodological review. Addiction. 2008;103:546–556. doi: 10.1111/j.1360-0443.2008.02149.x. doi:10.1111/j.1360-0443.2008.02149.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marshal MP, Friedman MS, Stall R, Thompson AL. Individual trajectories of substance use in lesbian, gay and bisexual youth and heterosexual youth. Addiction. 2009;104:974–981. doi: 10.1111/j.1360-0443.2009.02531.x. doi:10.1111/j.1360-0443.2009.02531.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Massachusetts Department of Education/Bureau of Student Development and Health. 1992 Youth Risk Behavior Survey. Malden, MA: Massachusetts Department of Education; 1993. [Google Scholar]
- Mustanski B. Ethical and regulatory issues with conducting sexuality research with LGBT adolescents: A call to action for a scientifically informed approach. Archives of Sexual Behavior. 2011;40:673–686. doi: 10.1007/s10508-011-9745-1. doi:10.1007/s10508-011-9745-1. [DOI] [PubMed] [Google Scholar]
- Nelson DE, Mowery P, Asman K, Pederson LL, O’Malley PM, Malarcher A, et al. Long-term trends in adolescent and young adult smoking in the United States: Metapatterns and implications. American Journal of Public Health. 2008;98:905–915. doi: 10.2105/AJPH.2007.115931. doi:10.2105/ajph.2007.115931. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pierce JP, Evans N, Farkas AJ, Cavin SW, Berry C, Kramer M, et al. Tobacco use in California: An evaluation of the Tobacco Control Program, 1989–1993. 1994. A Report to the California Department of Health Services: UC San Francisco: Center for Tobacco Control Research and Education. [Google Scholar]
- Remafedi G. Lesbian, gay, bisexual, and transgender youths: Who smokes, and why? Nicotine & Tobacco Research. 2007;9(Suppl. 1):S65–S71. doi: 10.1080/14622200601083491. doi:10.1080/14622200601083491. [DOI] [PubMed] [Google Scholar]
- Rojas NL, Killen JD, Haydel KF, Robinson TN. Nicotine dependence among adolescent smokers. Archives of Pediatrics & Adolescent Medicine. 1998;152:151–156. doi: 10.1001/archpedi.152.2.151. [DOI] [PubMed] [Google Scholar]
- Rosario M, Schrimshaw EW. The sexual identity development and health of lesbian, gay, and bisexual adolescents: An ecological perspective. In: Patterson CJ, D’Augelli AR, editors. Handbook of psychology and sexual orientation. New York: Oxford; in press. [Google Scholar]
- Rosario M, Schrimshaw EW, Hunter J. Predictors of substance use over time among gay, lesbian, and bisexual youths: An examination of three hypotheses. Addictive Behaviors. 2004;29:1623–1631. doi: 10.1016/j.addbeh.2004.02.032. doi:10.1016/j.addbeh.2004.02.032. [DOI] [PubMed] [Google Scholar]
- Rosario M, Schrimshaw EW, Hunter J. Butch/femme differences in substance use and abuse among young lesbian and bisexual women: Examination and potential explanations. Substance Use & Misuse. 2008;43:1002–1015. doi: 10.1080/10826080801914402. doi:10.1080/10826080801914402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosario M, Schrimshaw EW, Hunter J. Disclosure of sexual orientation and subsequent substance use and abuse among lesbian, gay, and bisexual youths: Critical role of disclosure reactions. Psychology of Addictive Behaviors. 2009;23:175–184. doi: 10.1037/a0014284. doi:10.1037/a0014284. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosario M, Schrimshaw EW, Hunter J. Cigarette smoking as a coping strategy: Negative implications for subsequent psychological distress among lesbian, gay, and bisexual youths. Journal of Pediatric Psychology. 2010;36:731–742. doi: 10.1093/jpepsy/jsp141. doi:10.1093/jpepsy/jsp141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ryan C, Huebner D, Diaz RM, Sanchez J. Family rejection as a predictor of negative health outcomes in white and Latino lesbian, gay, and bisexual young adults. Pediatrics. 2009;123:346–352. doi: 10.1542/peds.2007-3524. doi:10.1542/peds.2007-3524. [DOI] [PubMed] [Google Scholar]
- Taioli E, Wynder EL. Effect of the age at which smoking begins on frequency of smoking in adulthood. New England Journal of Medicine. 1991;325:968–969. doi: 10.1056/NEJM199109263251318. doi:10.1056/NEJM199109263251318. [DOI] [PubMed] [Google Scholar]
- Talley AE, Sher KJ, Littlefield AK. Sexual orientation and substance use trajectories in emerging adulthood. Addiction. 2010;105:1235–1245. doi: 10.1111/j.1360-0443.2010.02953.x. doi:10.1111/j.1360-0443.2010.02953.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thompson EM, Morgan EM. “Mostly straight” young women: Variations in sexual behavior and identity development. Developmental Psychology. 2008;44:15–21. doi: 10.1037/0012-1649.44.1.15. doi:10.1037/0012-1649.44.1.15. [DOI] [PubMed] [Google Scholar]
- Troiden RR. The formation of homosexual identities. In: Garnets Linda D., Kimmel Douglas C., editors. Psychological perspectives on lesbian and gay male experiences. New York: Columbia University Press; 1993. pp. 191–217. [Google Scholar]
- Zou G. A modified Poisson regression approach to prospective studies with binary data. American Journal of Epidemiology. 2004;159:702–706. doi: 10.1093/aje/kwh090. doi:10.1093/aje/kwh090. [DOI] [PubMed] [Google Scholar]