

Abstract
Objective: To demonstrate how the core characteristics of both evidence-based medicine (EBM) and evidence-based health care (EBHC) can be adapted to health sciences librarianship.
Method: Narrative review essay involving development of a conceptual framework. The author describes the central features of EBM and EBHC. Following each description of a central feature, the author then suggests ways that this feature applies to health sciences librarianship.
Results: First, the decision-making processes of EBM and EBHC are compatible with health sciences librarianship. Second, the EBM and EBHC values of favoring rigorously produced scientific evidence in decision making are congruent with the core values of librarianship. Third, the hierarchical levels of evidence can be applied to librarianship with some modifications. Library researchers currently favor descriptive-survey and case-study methods over systematic reviews, randomized controlled trials, or other higher levels of evidence. The library literature nevertheless contains diverse examples of randomized controlled trials, controlled-comparison studies, and cohort studies conducted by health sciences librarians.
Conclusions: Health sciences librarians are confronted with making many practical decisions. Evidence-based librarianship offers a decision-making framework, which integrates the best available research evidence. By employing this framework and the higher levels of research evidence it promotes, health sciences librarians can lay the foundation for more collaborative and scientific endeavors.
The evidence-based movement has emerged in the past few years in response to changes in the health care arena [1, 2]. Signaling this new orientation, many diverse disciplines and specialties have begun to attach the term evidence-based to their titles: cardiology, pediatrics, surgery, nursing, gastroenterology, diagnostic radiology, disease management, pathology, midwifery, complementary or alternative medicine, and health policy. The two principal evidence-based movement journals, ACP Journal Club and Evidence-Based Medicine, are quickly gaining recognition as core journals in clinical medicine [3–14]. Other specialties [15–17] have also formed their own journals.
The movement originated as evidence-based medicine (EBM) and recently has been eclipsed somewhat by a much broader movement, referred to as evidence-based health care (EBHC). EBM still retains considerable methodological rigor whereas EBHC seems to offer greater flexibility and adaptability to disciplines outside clinical medicine. At this stage, EBM has been more clearly and comprehensively articulated by its advocates than has EBHC. The new book Narrative Based Medicine [18] suggests that there may even be the formation of at least one splinter movement. After a decade of intense activity and increased acceptance as a framework for decision making, both the EBM and EBHC movements represent a major directional change rather than another passing fad in the health care arena.
The proliferation of so many evidence-based specialties appears to bode well for health sciences librarians. After all, librarians have positioned themselves as the experts at searching for the evidence needed for each of these elements in the larger EBHC movement [19–32]. Health sciences librarians apparently even played a role in attempts [33] to implement aspects of EBM during the 1920s. The EBHC movement nevertheless expects each area in health care to supply the necessary evidence to support its ongoing activities and operations. Cardiologists must have the evidence at hand to support their decisions to employ procedures, such as a catherization. Librarians similarly are called upon with increasing frequency to provide the requested evidence to continue provision of their collections, operations, or services. No wonder, then, that MLA President J. Michael Homan has identified the need to “foster evidence-based librarianship” as a major goal [34].
Evidence-based librarianship (EBL) adapts its core characteristics from the EBM and EBHC movements. EBM, in particular, offers some of the most powerful research designs available, such as randomized controlled trials and a decision-making framework that have been largely untapped by health sciences librarians. In clinical medicine, these research methods are intended to establish causal relationships while minimizing systematic or human biases. Until recently, health sciences librarianship has been largely influenced by research designs developed in the social, behavioral, and management sciences. Theoretical approaches developed in humanities disciplines, such as history or philosophy, have also influenced the field. EBL now seeks to adapt rigorously tested research designs from the health sciences, particularly clinical medicine.
To adapt core characteristics from EBM does not imply that EBL imitates EBM, or even EBHC, blindly. EBM focuses upon a disease-based model of decision making, whereas EBHC has a different type of appeal to health sciences librarians due to its flexibility in choice of methods and its similar service models. EBL incorporates the decision-making framework, the basic process, and many of the same research methods as EBM as a means to improve library practices [35–37]. EBL employs the best available evidence based upon library science research to arrive at sound decisions about solving practical problems in librarianship. EBL also enables health sciences librarians to practice the broad goal of continual, lifelong, self-directed learning while improving their practices. Unique circumstances in librarianship lead to a few intentional variations from the standard EBM approaches [38–41].
This article describes how the core characteristics of EBM and EBHC can be adapted to EBL. The author makes no claim to offer the definitive statement of what EBL should mean. This proposed framework remains largely speculative at this stage in its development. Only a continuous dialogue within the profession will produce such a consensus. The concept of EBL [42–46] preceded coinage of the actual term “evidence-based librarianship” [47] by several years, just as the concept of EBM preceded the published term “evidence-based medicine” [48–50]. In other words, both EBL and EBM are dynamic and evolving approaches to integrating research into practice. This article offers a conceptual framework to stimulate a dialogue; EBM and EBHC core characteristics and approaches are briefly reviewed and then followed by illustrations of how these approaches apply to health sciences librarianship. Because most health sciences librarians are already familiar with many of the core characteristics of EBM and EBHC, this article will avoid detailed explanations of either EBM and EBHC. The author has made sufficient references to original EBM and EBHC documents to lead the curious reader to in-depth explanations of these core characteristics.
DEFINITION
Evidence-based librarianship seeks to reintegrate the “science” back into library science. Davidoff writes:
Science is cognitive, involving accurate observation and clear description, hypothesis generation, data gathering and interpretation, and the creation of theory. But science is also a state of mind: skeptical, open, balanced, respectful of evidence, thorough, always on the alert for bias. [51]
Library science cannot be conceived of as a remote, ivory tower endeavor [52]. Librarians operate their libraries in the real world context of providing services and collections through managing budgets and other resources. Thus, EBL constitutes an applied rather than theoretical science. EBL merges scientific research with the pressing need to solve practical problems. And, like the scientific method, EBL provides a framework for self-correction as new information becomes available that suggests new directions or methods.
EVIDENCE-BASED MEDICINE (EBM) AND EVIDENCE-BASED HEALTH CARE (EBHC) CORE CONCEPTS
Evidence-based medicine shares with librarianship the goal of applying the best scientific research toward the immediate, practical need to provide efficient, compassionate medical services to patients. No succinct definition for EBM has yet to be universally agreed upon. EBM is continuously reinvented. One frequently cited definition states that:
Evidence-based medicine is the conscientious, explicit, and judicious use of current best evidence in making decisions about the care of individual patients. The practice of evidence-based medicine means integrating individual clinical expertise with the best available external clinical evidence from systematic research. [53]
The Evidence-Based Medicine Working Group offers a slightly different definition for EBM:
Evidence-based medicine de-emphasizes intuition, unsystematic clinical experience, and pathophysiologic rationale as sufficient grounds for clinical decision making and stresses the examination of evidence from clinical research … and the application of formal rules of evidence [for] evaluating the clinical literature. [54]
Other EBM advocates indicate that “expert opinion” and “standard practice” are insufficient bases for clinical decision making, because both of these traditional elements in medical practice often lag far behind the current best evidence [55]. EBM emphasizes the need to develop pragmatic clinical skills, but only when those skills are replenished with evidence systematically gleaned from rigorously conducted research. This goal of lifelong, continual learning has implications for undergraduate, graduate, and continuing medical education. EBM tries to reduce reliance upon the traditional medical model of expert authority, based upon the belief in the validity of cumulative clinical experience. EBM seeks to replace this authority-based model with a scientifically based, pragmatic model for medicine [56–59]. EBM relies upon scientific generalization but still emphasizes the importance of the individual patient's “characteristics, situations, and preferences” [60].
Evidence-based health care shares most of the same definitional characteristics as EBM, except it offers more inclusive approaches and a greater diversity of research methods, reflecting the broader array of problems and opportunities found across the continuum of all health care disciplines. EBHC recognizes the strength of the EBM approach and adapts it to diverse health care disciplines outside of clinical medicine. EBHC also emphasizes service models with relevance to librarianship.
A PRELIMINARY CONCEPTUAL FRAMEWORK FOR EVIDENCE-BASED LIBRARIANSHIP (EBL)
The author proposes the following seven-part conceptual framework of EBL:
EBL seeks to improve library practice by utilizing the best-available evidence combined with a pragmatic perspective developed from working experiences in librarianship;
EBL applies the best-available evidence, whether based upon either quantitative or qualitative research methods;
EBL encourages the pursuit of increasingly rigorous research strategies to support decisions affecting library practice;
EBL values research in all its diverse forms and encourages its communication, preferably through peer-reviewed or other forms of authoritative dissemination;
EBL represents a global approach to information seeking and knowledge development, involving research but not restricted to research alone;
EBL supports the adoption of practice guidelines and standards developed by expert committees based upon the best-available evidence, but not as an endorsement of adhering to rigid protocols; and
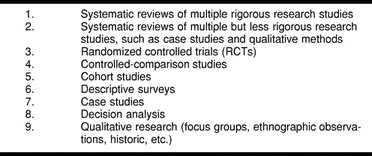
In the absence of compelling reasons to pursue another course, EBL adheres to the hierarchy (or levels) in Table 2 (below) for using the best-available evidence, lending priority to higher levels of evidence from the research.
Table 2 Levels of EBL evidence
The remaining sections of this article will further clarify the meanings of this seven-part conceptual framework of EBL.
THE EBL PROCESS
The EBL process enables health sciences librarians to integrate research findings into their daily practice by focusing upon a specific problem in need of immediate attention. The EBL process consists of formulating a practical question, searching for the evidence needed to answer the question, and systematically evaluating the gathered evidence for its usefulness and validity for answering the initial question. The specific EBL process outlined in Table 1 attempts to combine the scientific rigor of the EBM process with the flexibility found in the EBHC process to address the unique circumstances of health sciences librarianship.
Table 1 The EBL process

THE EBM AND EBHC PROCESSES
The Evidence-Based Care Resources Group in Canada developed the first version of the EBM process, which included five steps: formulate an important question that can be answered; critically review the best available evidence; estimate the expected benefits, harms, and costs for each alternative; judge the relative value of the expected benefits, harms, and costs; and (optional) develop clinical practice guidelines to efficiently guide similar decisions in the future [61]. Subsequent versions have simply clarified and slightly modified this original articulation of the EBM process. Sackett and Rosenberg emphasize searching prowess and methodological rigor in their steps: convert clinical information needs into answerable questions; track down, with maximum efficiency, the best evidence with which to answer them (whether from the clinical examination, diagnostic laboratory, published literature, or other sources); critically appraise that evidence for its validity and clinical usefulness; apply the results of this appraisal in clinical practice; and evaluate performance. Silagy and Haines offer a nearly identical version of the process, except they emphasize the importance of applying the evidence to treating a specific patient. Hebert and Tugwell emphasize the literature search and its evaluation [62–64]. The EBHC process largely resembles the EBM process. At this early stage in its development, EBHC differs from EBM mostly in its emphasis upon weighing the costs and benefits of any course of action in its process. EBHC also seems to view this process as a more iterative, less linear activity [65, 66].
FORMULATING EBL QUESTIONS
Questions drive the entire EBL process. EBL assigns highest priority to questions with greatest relevance to library practice. The wording and content of the questions determine what kinds of research designs are needed to secure answers. These questions may relate to librarians' individual specialties, their specific libraries, their type of libraries (e.g., hospital), or their entire profession. EBL question formulation deserves an entire article to describe it fully. Two points require emphasis here. First, precision, in terms of clarity and scope of the question, leads to a more efficient search for the needed evidence. As Oxman and Guyatt note, “Fuzzy questions tend to lead to fuzzy answers” [67]. Second, because so many initial questions lead to other questions, the question formulation process needs to be viewed as an iterative activity. Effective question formulation in step one of the EBL process leads to efficient searching for the needed evidence [68].
LEVELS OF EVIDENCE
Table 2 offers an EBL hierarchy for evaluating the comparative validity of different forms of evidence. These levels acknowledge the inherent validity of many quantitative and qualitative research methods while establishing the relative reliability and validity of results produced by each method. This hierarchy follows the EBM levels closely due to the sound theoretical bases for the levels that apply to any discipline, whether clinical medicine or librarianship. The EBL levels of evidence in Table 2 take into account the types of management methods needed in library practice that exists on the periphery of clinical medicine. The EBL levels also allow for the flexible integration of other research designs from areas such as the social sciences in possible future revisions. In addition, these levels recognize the current lack of research evidence to support ideal forms of methodological rigor, such as meta-analysis and randomized controlled trials (RCTs), that are found in some areas of clinical medicine. Most importantly, the nine EBL levels of evidence primarily are intended to alert librarians to the inherent human and systematic biases more frequently found and more difficult to control for in the lower levels of evidence.
Aside from the theoretical and methodological advantages, there are also practical reasons for considering use of levels of evidence for librarianship that resemble the levels in EBM. First, any research using these methods for library science situations will have inherently greater credibility to decision makers and possible allies in the broader health sciences arena. Second, using the same methods allows for the greater integration of health sciences librarianship into the larger research domain of health sciences. Finally, by using methods familiar to colleagues outside of librarianship, librarians can open doors to future multidisciplinary collaboration [69]. The methodological soundness for these levels of evidence, specifically the ability of higher levels of evidence to minimize bias, should drive any decision to employ the EBL levels of evidence. Figure 1 presents a tool for reconciling the two key variables in EBL: relevance versus rigor. EBL pursues the dual goals of encouraging research that exhibits both methodological rigor and relevance to practical situations in librarianship. EBL does favor relevance over rigor when evidence from more methodologically valid methods simply is not available. EBL generally lends preference to the higher levels of evidence when evidence from both higher- and lower-level methods are available. EBL requires lending greatest priority, as mentioned above, to the most relevant questions.
Figure 1.
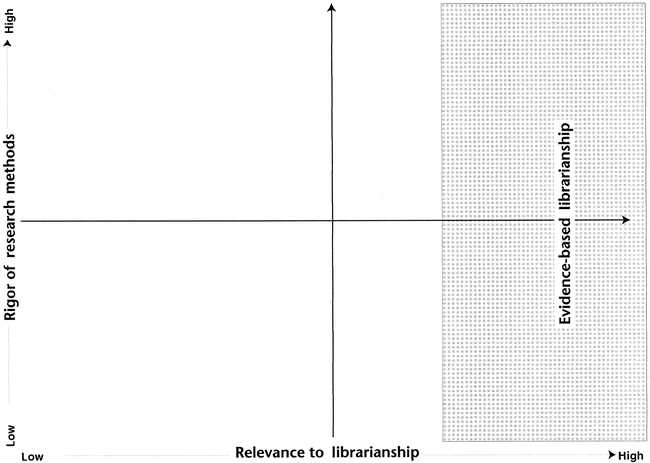
Evidence-based librarianship. EBL emphasizes evidence with the greatest relevance to librarianship, while encouraging use of higher levels of research evidence whenever possible.
EBM LEVELS OF EVIDENCE
The historic influence of clinical epidemiology on the evidence-based movement can be observed most strongly in its attention to EBM levels of evidence. Prior to the first published use of the term “Evidence-Based Medicine” [70] in 1991, clinical epidemiologists established the conceptual foundations for what later would become EBM. The Canadian Task Force on the Periodic Health Examination established the first known levels of research evidence for clinical practice in 1979. The highest level of evidence at that time involved at least one RCT. The second highest level involved well-designed cohort or case-control studies; the next level was based on comparisons of outcomes between different times and places, such as where penicillin had been introduced compared to where it had not been introduced. The lowest level consisted of “Opinions of respected authorities, based on clinical experience, descriptive studies or reports of expert committees” [71]. These levels resemble the rankings of experimental, observational, and descriptive research designs in epidemiology.
By 1992, the levels of EBM evidence had become more rigorous with “meta-analysis of randomized controlled trials” occupying the highest level in a clinical guidelines document prepared by the U.S. Agency for Health Care Policy and Research [72]. The next levels in this 1992 hierarchy resembled the Canadian levels of evidence, reflecting a reliance on time-tested standards for determining comparative methodological rigor. In 1994, the U.S. Preventive Services Task Force [73] outlined levels of evidence that largely resembled the Canadian levels of evidence. The Center for Evidence-Based Medicine (CEBM) at Oxford University in the United Kingdom has posted its latest version of the levels of evidence on its Website [74]. These levels of evidence, while more elaborate, reflected the basic logic found in the previously recommended levels of evidence of minimizing bias while ascending the hierarchy. EBHC levels of evidence [75] consisted of the same methodological hierarchy except that its own hierarchy directed more attention to decision analysis, surveys, and the many forms of qualitative research developed by the social sciences.
EBL LEVELS OF EVIDENCE
The EBL levels of evidence incorporate both the rigor and flexibility of methods offered by the EBM and EBHC levels of evidence, respectively. Much library practice uses methods such as surveys, focus groups, and other qualitative research modalities that the standard EBM levels of evidence typically would not consider. This diversity of methods enables EBL to address some research questions not easily handled by EBM. EBL approaches and methods are intended to be inherently useful in making everyday library decisions. Decision makers in the health care arena may be more likely to be persuaded by the validity and reliability of the higher levels of evidence. The rigor of the higher EBM levels of evidence still should be a goal for health sciences librarians, given the years it has taken to develop an understanding of the potential biases and relative scientific strength of each of these levels of evidence.
The levels of evidence in Table 2 are not rigid criteria for weighing the relative merits of research reports. Rather, they serve as basic guidelines for comparing different forms of evidence in search of a practical decision in librarianship. Within any level of evidence, there inevitably will be research reports that vary in their adherence to scientific methodological standards [76]. Some lower levels of EBL evidence may contain studies with higher-quality designs or methodological rigor than study designs ranked at the higher levels of EBL evidence. In this connection, a well-designed descriptive survey could have greater validity than a poorly designed or procedurally compromised randomized controlled trial. In addition, some research designs incorporate multiple research methods. For example, a cohort study may include a descriptive survey, or a decision analysis may be based upon quantitative results from randomized controlled trials.
The following sections describe the methods of the nine levels of EBL evidence. The first five levels are described in greater detail, because they are probably less well known to readers than are the lower levels of evidence. A number of studies have analyzed the research literature of library science in the United States [77–84]. These studies have been supplemented on an international scale, including studies in Asia and Africa [85–88]. Several other studies have focused on patterns in the health sciences libraries literature [89–94]. Most of these studies reveal that library research relies primarily upon three levels of evidence: descriptive surveys, case studies, and qualitative methods. Because of the familiarity of these methods to most readers, the author will only review these levels of evidence briefly. The nine levels of evidence are arranged hierarchically by the comparative rigor of each research method. Black has observed that the highest levels of evidence in EBM are neither possible nor desirable in all clinical research [95]. Sackett and Wennberg [96] have made similar points. These observations must be kept in mind for library practice when reviewing the nine levels of EBL evidence.
Systematic reviews
On Table 2, systematic reviews occupy the two highest levels of EBL evidence. Systematic reviews seek to answer important although narrowly defined questions pertaining to library practice. Systematic reviews employ explicitly stated methods for thoroughly searching a relevant literature, then carefully weighing the evidence found in that literature. As with other forms of rigorous scientific activity, systematic reviews are intended to reduce bias [97–101]. Systematic reviews may include, but are not restricted to, meta-analyses. Gray offers a checklist for critically appraising review articles that readers may find useful [102]. Systematic reviews sometimes are utilized to produce clinical guidelines and recommendations for expert panels in clinical medicine [103]. Physicians who use systematic reviews do appear to modify their practice [104]. Systematic reviews differ significantly from the still commonly found narrative review in the clinical medicine literature [105]. Narrative reviews often answer broad, rather than specific questions posed by authors. In the medical literature, narrative reviews still form the basis for many textbook chapters and literature reviews. Narrative reviews lack descriptions of the literature search methods employed by the authors and synthesize the literature in ways that may introduce the authors' biases [106, 107].
No meta-analysis currently exists for health sciences librarianship at this highest level. At this time, meta-analysis generally cannot even be considered a viable method for resolving discrepancies between research studies in librarianship. Saxton's recent attempt to conduct a meta-analysis on general reference-evaluation studies, which yielded limited results, drives home this point [108]. The attention paid by health sciences librarians to increasingly rigorous research methodologies suggests that a well-designed meta-analysis in our area of librarianship could develop within the next three to five years. The absence of such a productive meta-analysis does not negate the strength of this type of research method for making sound decisions. Thus, this method should still occupy the highest level in the hierarchy.
Readers may want to consult Light and Pillemer's book Summing Up for some creative ideas about how to conduct level-2 evidence research involving systematic reviews [109]. Slavin also has developed an alternative to meta-analysis [110, 111], although a common fallacy when combining small numbers of studies has to be avoided [112]. Booth and his colleagues in the United Kingdom have been exploring the use of systematic reviews to address practical library decision-making situations [113, 114]. Two physicians conducted a systematic review on the efficacy of physician database searching, which has high relevance for librarians [115].
Randomized controlled trials (RCTs)
Randomized controlled trials (also called “randomized clinical trials”) represent the most rigorous form of single research study. RCTs incorporate three elements: (1) subjects, usually patients in clinical medicine research studies, who are assigned to one of two or more groups that may be subjected to different interventions or simply the lack of an intervention such as a placebo; (2) researchers assign each subject to a particular group based solely upon chance; and (3) all subjects in the different groups are studied to measure the effects, if any, of the intervention [116]. The experimental group, which receives the intervention, must resemble the control groups in every appropriate way to maintain validity of an RCT. Only by controlling all relevant variables can the researchers detect any outcomes of the intervention [117]. RCTs employ prospective approaches, meaning that their designs call for the researchers to follow the participants from one point in time forward [118]. There are many time, resource, compliance, and ethical challenges to conducting RCTs [119–122]. As one example, would it be ethical to deny some users access to a needed library intervention (such as the use of an online catalog or references services) simply to create a control group? The typical methodological rigor of RCTs nevertheless positions them to be the “Gold Standard” for decision making in evidence-based practice.
RCTs in librarianship are difficult to identify because librarians usually do not label their research in these terms. Part of the problem may be due to insufficient statistical reporting methods [123]. Three prominent studies illustrate the power of RCTs in librarianship, however. Marshall and Neufeld conducted an RCT in 1981 that studied the quality of information-seeking skills in health care professionals who were either exposed or not exposed to an intervention (a clinical librarian). This RCT found that the intervention of a clinical librarian increased use of health sciences libraries [124]. Haynes, Ramsden, McKibbon, and Walker used the RCT method to determine the effect of MEDLINE fees on user access [125]. This study discovered that user fees did not affect the quality of online searches by non-librarians. This study did reveal, though, that those searchers who were charged a fee searched significantly less than those searchers who were not charged a fee. In a third RCT, medical students were randomly assigned either to receive or not receive a three-hour database-searching instructional intervention. Medical students who received the instructional intervention performed significantly better database searches than the students in the control group [126].
Controlled-comparison studies
A form of comparison study in medicine, known as the case-control study, looks at outcomes and tries to trace them to previous defining circumstances. Lichtenstein, Mulrow, and Elwood describe the process of a case-control study: “persons with a particular condition are identified (cases), a series of persons without the condition selected (controls) and the existing or prior exposures or characteristics of the two groups compared” [127]. Researchers in clinical medicine typically study the members' health histories in each group in search of a putative cause for disease in the first group [128]. Because of the risk of bias in these studies, researchers gravitate toward collecting more objective forms of data found in medical records rather than primarily relying upon patients' personal accounts of their health histories. Case-control studies are designed to establish possible causes for a condition. For example, a case-control study may look at how certain patients with lung cancer (cases) differ from another group (controls) who otherwise resemble these patients. This study could determine that all or most of the lung cancer patients are smokers (a possible cause), whereas few controls are smokers. This difference may explain the cases with lung cancer. Case-control studies in medicine normally take a retrospective approach, meaning that they examine a present condition by looking back at past events to identify causative factors for disease [129]. There are numerous strategies for reducing bias in case-control studies [130–132].
The author knows of no study in health sciences librarianship that precisely duplicates a case-control study design in medicine. Yet, a similar application in librarianship would substitute a disease condition with a non-pathologic outcome in a library environment. For example, one could study different end-user physician or medical-student searchers. One could examine the backgrounds of searchers classified as highly proficient (cases) and then compare them to far less proficient searchers (controls) who otherwise resemble the proficient searchers. This approach may turn up differences between the groups of searchers that explains why some searchers are more proficient than others. Similarly, another case-control study could examine the possible reasons why some students are more frequent library users (cases) than other students (controls).
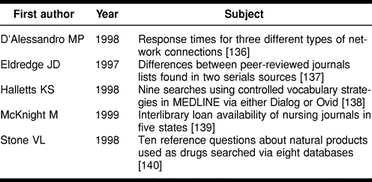
Controlled-comparison studies in librarianship may be thought of as a specific subtype of comparison study, which resemble case-control studies in medicine in some ways. General comparison studies in librarianship examine all sorts of different groupings and analyze their differences, often in a descriptive manner. Controlled-comparison studies are distinguished from mainstream comparison studies in their attempt to match cases and controls in most, or all, relevant ways. The controlled-comparison study draws its strength from matching cases and controls to minimize the alternative explanations for the different outcomes. The cases and controls are not randomized, however. In this way, they may be thought of as “non-randomized controlled trials” (NRCT) applied in circumstances in which RCTs are impractical or unethical. The sequence of observed events normally differs as well: cases and controls are identified at the beginning of the study in EBL rather than as outcomes as seen in EBM. These designs potentially use a more flexible research design than their counterparts in medicine, because library research generally does not focus primarily upon negative [133] or pathophysiological conditions such as disease. Controlled-comparison studies in librarianship can employ either prospective or retrospective strategies as long as groups of cases and controls are legitimately matched. Conceivably, some benchmarking projects could be loosely defined as forms of controlled-comparison study [134, 135]. Table 3 offers examples of controlled-comparison studies, based upon a reading of the methods sections found in these articles.
Table 3 Examples of controlled comparison studies
Cohort design studies
In clinical medicine, cohort studies normally study a group of people who potentially share one or more characteristics such as common experiences or conditions [141]. These common experiences may include their age, sex, geographic locale, exposure to a disease or substance, or an intervention. Cohort studies seek to describe possible causal links and pose probabilities of risk. The Framingham Study of coronary heart disease has been one of the largest and well-known cohort studies in the United States [142]. Cohort studies collect data with either concurrent or historic approaches, depending upon the sequence in which researchers begin to study the cohort. Prospective cohort studies (sometimes called “concurrent cohort studies”), such as the Framingham Study, normally begin to measure relevant indicators of variables prior to an exposure or incidence of disease. These measurements continue throughout the study until a certain endpoint. Retrospective cohort studies (sometimes called “historic cohort studies”) identify the cohort, their exposure, and outcomes afterward, as a follow-up study [143]. Regardless of data-collection approach, all cohort studies infer causality between a condition during an earlier period to a condition at a later period. An epidemiologic cohort study must include members of a population that has been exposed to a factor of interest that will be compared to members of the same (or similar) population, which has not been exposed to a factor of interest. Outcomes between the two (or more) groups are then compared in the analysis.
Although EBL emphasizes adaptations from EBM or EBHC research designs, cohort studies are quite prevalent in other disciplines. The social and behavioral sciences have employed cohort studies to understand better phenomena as diverse as childhood development, political participation, childlessness, substance abuse, prenatal or early childhood exposures leading to mental illness in later life, characteristics of the digital generation, and psychological stress in the workplace. The biological and earth sciences have employed cohort studies to understand better elements as diverse as Atlantic cod, evergreen trees, dogs, seals, and even fossilized extinct species [144].
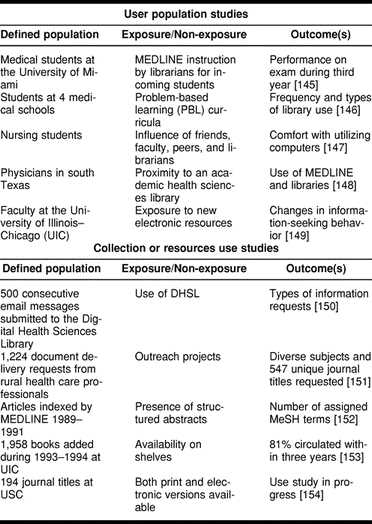
Cohort studies in librarianship are fairly popular. Cohort studies in both medicine and librarianship describe possible causal relationships of variables across time involving designated groupings. Instead of centering on probable risk as in medicine, though, cohort studies in librarianship focus on probabilities of outcomes. Interestingly, librarians rarely identify these projects as cohort studies. There are two major types of cohort-study design in librarianship: (1) user-population cohort designs and (2) collections or resources use cohort-study designs. Table 4 offers a representative sample of the diverse applications of the cohort-study design in health sciences librarianship. Table 4 should not be considered to be a comprehensive inventory, because it does not include numerous other examples from librarianship of either major type of cohort study.
Table 4 Diverse examples of cohort study designs in EBL
Descriptive surveys
As already noted, descriptive surveys are one of the most popular modes of conducting library science research. Surveys can be employed for higher levels of EBL research to describe the opinions, characteristics, or experiences of a group. For example, a descriptive survey may be employed in combination with a cohort study. Probably the most famous and well-conducted survey in health sciences librarianship is the Rochester Study, which shows the importance of libraries to medical outcomes [155]. The library literature offers many excellent examples of other well-designed and well-conducted descriptive surveys. Less formal surveys also may answer practical questions [156]. Even citation analysis can be considered a form of descriptive survey. Yet, surveys often are far more complex enterprises than they appear on the surface. The author recommends the Survey Kit series, published by Sage [157], as a source of practical advice on conducting surveys, which are more likely to be both valid and reliable.
Decision analysis
Although the seventh level of EBL evidence has rarely been employed in health sciences librarianship, decision analysis has been utilized in academic librarianship [158]. In health management and public policy analysis, however, decision analysis has been quite popular for resolving conflicting information [159]. The most popular vehicle for decision analysis has been the “decision tree” model, which enables decision makers to follow the probabilities and outcomes of a particular course of action. An article by Richardson and Detsky offers a clear introduction to decision trees [160]. This method has proved useful in handling complex decisions involving immunization policies [161] or navigating the ethical uncertainties of physician-assisted suicide [162].
Case studies
Case studies are one of the most popular descriptive research methods employed by librarians, as observed above. Case studies use opportunities that occur frequently in librarianship and require only observational skills rather than expensive or elaborate measurement techniques, just as case reports in medicine allow physicians to integrate valuable observations into everyday practice [163]. Case studies therefore enable librarians to circumnavigate many of the time and cost constraints of other research designs. Case studies describe with varying degrees of detail and objectivity a series of experiences in a library or a library program. They also vary greatly in rigor and degree of quantification. Case studies containing greater quantification tend to be easier for third parties to evaluate with greater objectivity.
Many issues of the Bulletin of the Medical Library Association, Health Libraries Review, Medical Reference Services Quarterly, or Bibliotheca Medica Canadiana contain at least one case study. One of the major drawbacks of case studies in librarianship is their overwhelming positive-outcome bias. To place this eighth level of evidence in perspective, the reader most likely cannot recall ever reading about a library or a library program that is described as a major failure. Line has criticized this deficiency to the case study method in the broader literature [164]. While some librarians may want to review case studies to learn about what types of programs have been successful, the absence of less successful programs as described in the library literature has the inadvertent effect of not alerting librarians to the educational lessons learned from others' failures. This omission consequently can lead some librarians to repeat failures experienced elsewhere. Case studies commonly have exploratory, descriptive, or explanatory purposes. There are many forms of bias when conducting case studies, a detracting aspect that offsets many of the conveniences with researching at this level of evidence [165].
Qualitative research
Health sciences librarians have explored the use of at least three forms of qualitative methods: ethnographic, focus group, and historic. These qualitative methods are most helpful for developing hypotheses or testing hypotheses in circumstances where higher levels of evidence are difficult to apply [166]. Qualitative research has not really been explored to the same extent in EBM. Many of the pioneering studies in other fields, such as psychology, were qualitative studies involving small numbers of subjects. Piaget's work in child development is only one noteworthy example of the significant contributions of these research types of designs.
Qualitative research has attracted great interest in librarianship, although these methods have not been explored extensively. Some focus group experiences have been documented [167–169]. McKnight and Peet moreover have synthesized the ethnographic studies about information-seeking behaviors [170]. Qualitative methods can yield many benefits for librarians in developing hypotheses or in studying unique circumstances in which quantifiable methods would be inappropriate [171]. Some librarians object to the relative positioning of qualitative methods in this ranking of evidence. This ranking stems not from any fault or skill limitations of researchers in applying qualitative techniques. Instead, these designs invite possible biases that are often difficult for third parties to detect. As qualitative research methods continue to reduce both systematic and human bias, this grouping of research designs will assume a higher position in the nine levels of EBL evidence.
IMPLEMENTING THE NINE LEVELS OF EBL EVIDENCE
Most librarians can appreciate the need to adhere to the levels of evidence due to the demonstrated relative strengths of each method. These comparative evaluations of the risks of different research methods in introducing human or systematic bias and the relative strength of each in determining causal relationships are familiar to past students in research courses. Thus, there has been little debate about this issue. It may seem discouraging, however, that librarianship does not offer a better representation of the more rigorous methods at the higher levels of evidence. There are three points to keep in mind on this issue. First, the Canadian Task Force on the Periodic Health Examination noted, in 1979, the “lack of strong experimental evidence for or against most of the measures that we have considered.” The task force further noted that “Even evidence from cohort studies and case-control studies was infrequently found” [172]. Secondly, there are still many current health care practices that lack sufficient evidence [173] to justify their continuation with enough confidence, although that number has been shrinking as the result of the EBM movement [174]. In some specialties—such as ear, nose, and throat surgery; anesthesiology; burns management; surgery; or emergency medicine [175–182]—researchers have concluded that an insufficient evidence base exists in those specialties for a variety of reasons. Yet, some of these researchers suggest that their respective evidence bases can be improved in spite of the current situation. Finally, librarianship may now have a plausible strategic framework through EBL to catch up quickly to the rigorous levels of EBM.
CONCLUSION
Every day health sciences librarians, like their colleagues in other health care specialties, make numerous decisions. These decisions range from the critical to the mundane. Upon reflection, readers may be reminded of some of these decisions: With what vendor should the library contract large sums of money for book, journal, or database services? Which staff-training program should the library employ? What library resources or services should be emphasized? What are the essential factors in deciding between print and electronic media? To what journals should the library subscribe? Which books should be bought? What tools best answer reference questions?
EBL offers a possible framework for making these decisions under conditions of uncertainty by providing a system for evaluating different forms of research evidence. By employing these methods that are familiar to many colleagues in other areas of health care, librarians also increase understanding about their unique challenges and invite collaboration from outside librarianship. The roads to EBM and EBHC in other areas of health care were full of obstacles, conceptual dead ends, and setbacks. By adapting the evolved core characteristics of EBM and EBHC that seem most applicable to librarians' circumstances, EBL can advance the mission of librarianship faster and more effectively. The foundations of EBL preceded the actual term, and health sciences librarians already are using most of the levels of evidence as outlined in this article. As EBL continues to evolve, librarians undoubtedly will find an increasing number of research projects conducted at the higher levels of evidence that are capable of facilitating practical decisions. Research studies are essential ingredients in making critical decisions. Although EBL provides a framework for focused thinking about decisions, it still requires librarians to think about their decisions. As Dauten states: “Just because we increase the speed of information, doesn't mean we can increase the speed of decisions. Pondering, reflecting and ruminating are undervalued skills” [183].
Acknowledgments
The author appreciates the encouragement of the MLA Continuing Education Committee, particularly Amelia Butros, to develop the course that became the springboard for this article. He also thanks the students in the MLA course (#753) on EBL, who offered many helpful comments. Finally, the author appreciates the assistance of Thomas Becker, Andrew Booth, Anne Brice, Ana Cleveland, Ph.D., Molly Harris, Bruce Madge, Ann McKibbon, and Kristine Tollestrup for their encouragement or constructive criticism.
REFERENCES
- Sackett DL, Richardson WS, Rosenberg W, and Haynes RB. Evidence-based medicine: how to practice and teach EBM. New York, NY: Churchill Livingstone. 1997 16. [Google Scholar]
- Gray JAM. Evidence-based healthcare. Edinburgh, U.K.: Churchill Livingstone. 1997 4. [Google Scholar]
- Yusuf S, Cairns JA, Camm AJ, Fallen FL, and Gersh BJ. eds. . Evidence based cardiology. London, U.K.: BMJ Books. 1998 [Google Scholar]
- Elliott EJ, Moyer VA. Evidence-based paediatrics. J Paediatr Child Health. 1998 Feb. 34(1):14–7. [DOI] [PubMed] [Google Scholar]
- Rodarte JR. Evidence-based surgery. Mayo Clin Proc. 1998 Jun. 73(6):603. [DOI] [PubMed] [Google Scholar]
- Cullum N, DiCenso A, and Ciliska D. Evidence-based nursing: an introduction. Evid Based Nurs. 1997 Nov. (Novpilot issue)::iv. [DOI] [PubMed] [Google Scholar]
- Schoenfeld P, Cook D, Hamilton F, Laine L, Morgan D, and Peterson W. An evidence-based approach to gastroenterology therapy. Gastroenterology. 1998 Jun. 114(6):1318–25. [DOI] [PubMed] [Google Scholar]
- Dixon AK. Evidence-based diagnostic radiology. Lancet. 1997 Aug 16. 350(9076):509–12. [DOI] [PubMed] [Google Scholar]
- Ellrodt G, Cook DJ, Lee J, Cho M, Hunt D, and Weingarten S. Evidence-based disease management. JAMA. 1997 Nov 26. 278(20):1687–92. [PubMed] [Google Scholar]
- Fleming KA. Evidence-based pathology. Evid Based Med. 1997 Sept/Oct. 2(5):132–3. [Google Scholar]
- American College of Nurse-Midwives. Evidence-based health care. Washington, DC: The College. 1999. [Google Scholar]
- Spencer JW, Jacobs JJ. eds. . Complementary/alternative medicine: an evidence-based approach. St Louis, MO: Mosby. 1999 [Google Scholar]
- Gray JAM.. Evidence-based health care. Evid Based Health Pol Manage. 1997;1(1):6–7. [Google Scholar]
- Hill DR. Brandon/Hill selected list of books and journals for the small medical library. Bull Med Libr Assoc. 1999 Apr. 87(2):145–69. [PMC free article] [PubMed] [Google Scholar]
- Yusuf S, Kitching AD. Evidence-based cardiovascular medicine: why another journal? Evid Based Cardiovasc Med. 1997 Apr. 1(1):1. [DOI] [PubMed] [Google Scholar]
- Evidence-based mental health. London, U.K.: BMJ Publishing Group. [Google Scholar]
- Evidence-based eye care. Philadelphia, PA: Lippincott Williams & Wilkins. [Google Scholar]
- Greenhalgh T, Hurwitz B. eds. . Narrative based medicine: dialogue and discourse in clinical practice. London, U.K.: BMJ Books. 1998 [Google Scholar]
- McKibbon A. PDQ: Evidence-based principles and practice. Hamilton, Ontario: BC Decker. 1999 [Google Scholar]
- Gorman PN, Ash J, and Wykoff L. Can primary care physicians' questions be answered using the medical journal literature? Bull Med Libr Assoc. 1994 Apr. 82(2):140–6. [PMC free article] [PubMed] [Google Scholar]
- Haines M.. Evidence-based practice: new opportunities for librarians [editorial] Health Libs Rev. 1994;11:221–5. [Google Scholar]
- McKibbon KA, Wilczynski N, Hayward RS, Walker-Dilks CJ, and Haynes RB. The medical literature as a resource for health care practice. J Am Soc Info Sci. 1995 Dec. 46(10):737–42. [Google Scholar]
- McCarthy LH. Evidence-based medicine: an opportunity for health sciences librarians. Med Ref Serv Q. 1996 Winter. 15(4):63–71. [DOI] [PubMed] [Google Scholar]
- Michaud GC, McGowan JL, van derJagt RH, Dugan AK, and Tugwell P. The introduction of evidence-based medicine as a component of daily practice. Bull Med Libr Assoc. 1996 Oct. 84(4):478–81. [PMC free article] [PubMed] [Google Scholar]
- Cumbers BJ, Donald A. Using biomedical databases in everyday clinical practice: the Front-Line Evidence-Based Medicine project in North Thames. Health Libs Rev. 1998 Dec. 15(4):255–65. [DOI] [PubMed] [Google Scholar]
- Rose S. Challenges and strategies in getting evidence-based practice into primary health care—what role the information professional? Health Libs Rev. 1998 Sept. 15(3):165–74. [DOI] [PubMed] [Google Scholar]
- Tsafrir J, Grinberg M. Who needs evidence-based health care? Bull Med Libr Assoc. 1998 Jan. 86(1):40–5. [PMC free article] [PubMed] [Google Scholar]
- Harrison J. Designing a search strategy to identify and retrieve articles on evidence-based health care using MEDLINE. Health Libr Rev. 1997 Mar. 14(1):33–42. [PubMed] [Google Scholar]
- Kolner SJ, Dalrymple PW, and Christiansen R. Teaching skills in medical information retrieval to medical students. J Med Educ. 1986 Nov. 61(11):906–10. [DOI] [PubMed] [Google Scholar]
- MacDougall J, Brittain JM. Health services information. In: Line M, ed. Librarianship and information work worldwide 1998. London, U.K.: Bowker Saur. 1998 171–99. [Google Scholar]
- Buckingham J. Evidence-based medicine quality filters in MEDLINE records: theory, practice and practical reality. Bibl Medica Can. 1998 Fall. 20(1):7–11. [Google Scholar]
- Palmer J.. Schooling and skilling health librarians for an evidence-based culture. Adv Librarianship. 2000;23:145–67. [Google Scholar]
- Alleman A.. Foreward. Med Interpreter. 1928;(1):i–ii. [Google Scholar]
- Homan JM. 2000/2001 priorities. MLA News. 2000 Apr. (325):27. [Google Scholar]
- Eldredge J. Evidence-based librarianship. Hypothesis. 1997 Fall. 11(3):4–7.(Available from: http://gain.mercer.edu/mla/research/hypothesis.html.). [Google Scholar]
- Eldredge JE. Evidence-based librarianship. [Continuing education course #753]. Chicago, IL: Medical Library Association. 1999 [Google Scholar]
- Bradley J, Marshall JG. Using scientific evidence to improve information practice. Health Libr Rev. 1995 Sep. 12(3):147–57. [DOI] [PubMed] [Google Scholar]
- Schneider E, Mankin CJ, and Bastille JD. Practical library research: a tool for effective library management. Bull Med Libr Assoc. 1995 Jan. 83(1):22–6. [PMC free article] [PubMed] [Google Scholar]
- Medical Library Association, Research Task Force. Using scientific evidence to improve information practice: the research policy statement of the Medical Library Association. [Web Document]. Chicago, IL: The Association. [cited 1999 Feb 12]. <http://www.mlanet.org/research/science1.html>. [Google Scholar]
- Special Libraries Association, Board of Directors. Competencies for special librarians of the 21st century. Standard 2.10. Washington, D.C.: The Association. 1997 [Google Scholar]
- Byrd GD. Evidence-based librarianship [letter]. Hypothesis. 1998 Spring. 12(1):5–12. [Google Scholar]
- Roddham M. Responding to the reforms—are we meeting the need? Health Libr Rev. 1995 Jun. 12(2):101–14. [DOI] [PubMed] [Google Scholar]
- Booth A. In search of the evidence: informing effective practice. J Clin Effect. 1996 Apr. 1(1):25–9. [Google Scholar]
- Anderson RK. Inaugural address. Bull Med Libr Assoc. 1998 Jan. 86(1):137–9. [Google Scholar]
- Medical Library Association, Research Task Force. Using scientific evidence to improve information practice: the research policy statement of the Medical Library Association. [Web Document]. Chicago, IL: The Association. [cited 1999 Feb 12]. <http://www.mlanet.org/research/science1.html>. [Google Scholar]
- Bradley J, Marshall JG. Using scientific evidence to improve information practice. Health Libr Rev. 1995 Sep. 12(3):147–57. [DOI] [PubMed] [Google Scholar]
- Eldredge J. Evidence-based librarianship. Hypothesis. 1997 Fall. 11(3):4–7.(Available from: http://gain.mercer.edu/mla/research/hypothesis.html.). [Google Scholar]
- Sackett DL, Richardson WS, Rosenberg W, and Haynes RB. Evidence-based medicine: how to practice and teach EBM. New York, NY: Churchill Livingstone. 1997 16. [Google Scholar]
- Tsafir J, Grinberg M. Who needs evidence-based health care? Bull Med Libr Assoc. 1998 Jan. 86(1):40–5. [PMC free article] [PubMed] [Google Scholar]
- Guyatt GH. Evidence-based medicine. ACP J Club. 1991 Mar/Apr. 114(supp 2):A–16. [PubMed] [Google Scholar]
- Davidoff F. The future of Annals. Ann Intern Med. 1995 Mar 1. 122(5):375–6. [DOI] [PubMed] [Google Scholar]
- Booth A. Testing the lore of research. Libr Assoc Rec. 1998 Dec. 100(12):654. [Google Scholar]
- Sackett DL. Evidence-based medicine: what it is and what it isn't. BMJ. 1996 Jan 13. 312(7023):71–2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Evidence-Based Medicine Working Group. Evidence-based medicine: a new approach to teaching the practice of medicine. JAMA. 1992 Nov 4. 268(17):2420–5. [DOI] [PubMed] [Google Scholar]
- Oxman AD, Sackett DL, and Guyatt GH. Users' guide to the medical literature. 1. how to get started. JAMA. 1993 Nov 3. 270(17):2093–5. [PubMed] [Google Scholar]
- Mulrow C, Cook D. eds. . Systematic reviews: synthesis of best evidence for health care decisions. Philadelphia, PA: American College of Physicians. 1998 [DOI] [PubMed] [Google Scholar]
- Waeckerle JF. Evidence-based emergency medicine: integrating research into practice. Ann Emerg Med. 1997 Nov. 30(5):626–8. [DOI] [PubMed] [Google Scholar]
- Evidence-Based Care Resource Group. Evidence-based care: 5. lifelong learning: how can we learn to be more effective? Can Med Assoc J. 1994 Jun 15. 150(12):1971–3. [PMC free article] [PubMed] [Google Scholar]
- Davidoff F. The future of Annals. Ann Intern Med. 1995 Mar 1. 122(5):375–6. [DOI] [PubMed] [Google Scholar]
- McKibbon KA. Evidence-based practice. Bull Med Libr Assoc. 1998 Jul. 86(3):396–401. [PMC free article] [PubMed] [Google Scholar]
- Evidence-Based Care Resources Group. Evidence-based care: 2. setting guidelines: how should we manage this problem? Can Med Assoc J. 1994 May 1. 150(9):1417–23. [PMC free article] [PubMed] [Google Scholar]
- Sackett DL, Rosenberg WMC. The need for evidence-based medicine. J R Soc Med. 1995 Nov. 88(11):620–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Silagy C, Haines A. eds. . Evidence-based practice in primary care. London, U.K.: BMJ Books,. 1998 6. [Google Scholar]
- Hebert PC, Tugwell PX. A reader's guide to the medical literature–an introduction. Postgrad Med J. 1996 Jan. 72(843):1–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gray JAM. Evidence-based healthcare. Edinburgh, U.K.: Churchill Livingstone. 1997 4. [Google Scholar]
- Reerink E, Walshe K.. Evidence-based healthcare: a critical appraisal. J R Soc Med. 1998;91(supp 35):1. doi: 10.1177/014107689809135s01. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oxman AD, Guyatt GH. Guidelines for reading literature reviews. Can Med Assoc J. 1988 Apr 15. 138(8):697–703. [PMC free article] [PubMed] [Google Scholar]
- Eldredge JD. Evidence-based librarianship: searching for the needed EBL evidence. Med Ref Serv Q. 2000 Summer. 19(2). in press. [DOI] [PubMed] [Google Scholar]
- Humphreys BL. Librarians and collaborative research: toward a better scientific base for information practice. Bull Med Libr Assoc. 1996 Jul. 84(3):433–6. [PMC free article] [PubMed] [Google Scholar]
- Guyatt GH. Evidence-based medicine. ACP J Club. 1991 Mar/Apr. 114(supp 2):A–16. [PubMed] [Google Scholar]
- Canadian Task Force on the Periodic Health Examination. The periodic health exam. Can Med Assoc J. 1979 Nov 3. 121:1193–254. [PMC free article] [PubMed] [Google Scholar]
- Agency for Health Care Policy and Research. Acute pain management: operative or medical procedures and trauma. Rockville, MD: U.S. Department of Health and Human Services. 1992. 107. [Google Scholar]
- U. S. Preventive Services Task Force. Guide to clinical preventive services. 2d ed. Baltimore: Williams & Wilkins. 1994 [Google Scholar]
- Centre for Evidence-Based Medicine. Levels of evidence and grades of recommendations. [Web document]. Oxford, U.K.: Oxford University. [cited 1999 Apr 4]. <http://cebm.jr2.ox.ac.uk/docs/levels.html>. [Google Scholar]
- Gray JAM.. Evidence-based health care. Evid Based Health Pol Manage. 1997:6–7. [Google Scholar]
- Wilson MC, Hayward RSA, Tunis SR, Bass EB, and Guyatt G. Users' guide to the medical literature. VIII. how to use clinical practice guidelines. B. what are the recommendations and will they help you in caring for your patients? JAMA. 1995 Nov 22/29. 274(20):1630–2. [DOI] [PubMed] [Google Scholar]
- Atkins SE. Subject trends in library and information science research, 1975–1984. Libr Trends. 1988 Spring. 36(4):633–58. [Google Scholar]
- Peritz BC.. The methods of library science research: some results from a bibliometric survey. Libr Res. 1980–81;2:251–68. [Google Scholar]
- Nour MM.. A quantitative analysis of the research articles published in the core library journals of 1980. Libr Inf Sci Res. 1985;7(3):261–73. [Google Scholar]
- Feehan PE, Gragg WL, Havener WM, Kester DD.. Library and information science research: an analysis of the 1984 journal literature. Libr Inf Sci Res. 1987;9(3):173–85. [Google Scholar]
- Enger KB, Quirk G, Stewart JA.. Statistical methods used by authors of library and information science journal articles. Libr Inf Sci Res. 1989;11(1):37–46. [Google Scholar]
- Jarvelin K, Vakkari P.. Content analysis of research articles in library and information science. Libr Inf Sci Res. 1990;12(4):395–421. [Google Scholar]
- Buttlar L. Analyzing the library periodical literature: content and authorship. Coll Res Libr. 1991 Jan. 52(1):38–53. [Google Scholar]
- Crawford GA. The research literature of academic librarianship: a comparison of College & Research Libraries and Journal of Academic Librarianship. Coll Res Libr. 1999 May. 60(3):224–30. [Google Scholar]
- Rochester M, Vakkari P.. International LIS research: a comparison of national trends. IFLA J. 1998;24(3):166–75. [Google Scholar]
- Cheng H.. A bibliometric study of library and information research in China. Asian Libr. 1996;5(2):30–45. [Google Scholar]
- Nkereuwem EE.. Accrediting knowledge: the ranking of library and information science journals. Asian Libr. 1997;6(1/2):71–6. [Google Scholar]
- Olorunisola R, Akinboro EO.. Bibliographic analysis of articles: a study of African Journal of Library, Archives and Information Science, 1991–1997. Afri J Libr Arch & Inf Sci. 1998;8(2):151–54. [Google Scholar]
- Dimitroff A. Research in health sciences library and information science: a quantitative analysis. Bull Med Libr Assoc. 1992 Oct. 80(4):340–6. [PMC free article] [PubMed] [Google Scholar]
- Burdick AJ, Doms CA, Doty CC, and Kinzie LA. Research activities among health sciences librarians: a survey. Bull Med Libr Assoc. 1990 Oct. 78(4):400–2. [PMC free article] [PubMed] [Google Scholar]
- Haiqi Z. Analysing the research articles published in three periodicals of medical librarianship. Intl Inf Libr Rev. 1995 Sep. 27:237–48. [Google Scholar]
- Haiqi Z.. A bibliometric study on articles of medical librarianship. Inf Process Manage. 1995;31(4):499–510. [Google Scholar]
- Haiqi Z. Author characteristics in three medical library periodicals. Bull Med Libr Assoc. 1996 Jul. 84(3):423–6. [PMC free article] [PubMed] [Google Scholar]
- Mularski CA, Bradigan PS. Academic health sciences librarians' publications patterns. Bull Med Libr Assoc. 1991 Apr. 79(2):168–77. [PMC free article] [PubMed] [Google Scholar]
- Black N. Why we need observational studies to evaluate the effectiveness of health care. BMJ. 1996 May 11. 312(7040):1215–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sackett DL, Wennberg JE. Choosing the best research design for each question. BMJ. 1997 Dec 20–27. 315(7123):1636. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guyatt GH. Evidence-based emergency medicine. Ann Emerg Med. 1997 Nov. 30(5):675–6. [DOI] [PubMed] [Google Scholar]
- Oxman AD, Guyatt GH.. Validation of an index of the quality of review articles. J Clin Epidemiol. 1991;44(11):1271–8. doi: 10.1016/0895-4356(91)90160-b. [DOI] [PubMed] [Google Scholar]
- Hunt DL, McKibbon KA. Locating and appraising systematic reviews. Ann Intern Med. 1997 Apr 1. 126(7):532–8. [DOI] [PubMed] [Google Scholar]
- Greenhalgh T. Papers that summarize other papers (systematic reviews and meta-analyses). BMJ. 1997 Sep 13. 315(7109):672–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oxman AD, Cook DJ, and Guyatt GH. Users' guides to the medical literature. VI. how to use an overview. JAMA. 1994 Nov 2. 272(17):1367–71. [DOI] [PubMed] [Google Scholar]
- Gray JAM.. Evidence-based health care. Evid Based Health Pol Manage. 1997:74–5. [Google Scholar]
- Cook DJ, Greengold NL, Ellrodt AG, and Weingarten SR. The relation between systematic reviews and practice guidelines. In: Mulrow C, Cook D, eds. Systematic reviews: synthesis of best evidence for health care decisions. Philadelphia, PA: American College of Physicians. 1998 55–65. [DOI] [PubMed] [Google Scholar]
- Jordens CFC, Hawe P, Irwig LM, Henderson-Smart DJ, Ryan M, Donoghue DA, Gabb RG, and Fraser IS. Use of systematic reviews of randomized trials by Australian neonatologists and obstetricians. Med J Aust. 1998 Mar 16. 168(6):267–70. [DOI] [PubMed] [Google Scholar]
- Forgacs I. How to write a review. In: Hall GM, ed. How to write a paper. 2d ed. London, U.K.: BMJ Books. 1998 77–82. [Google Scholar]
- Cook DJ, Mulrow CD, and Haynes RB. Synthesis of best evidence for clinical decisions. In: Mulrow C, Cook D, eds. Systematic reviews: synthesis of best evidence for health care decisions. Philadelphia, PA: American College of Physicians. 1998 5–12. [DOI] [PubMed] [Google Scholar]
- McAlister FA, Clark HD, vanWalraven C, Straus SE, Lawson FME, Moher D, and Mulrow CD. The medical review article revisited: has the science improved? Ann Intern Med. 1999 Dec 21. 131(12):947–51. [DOI] [PubMed] [Google Scholar]
- Saxton ML. Reference service evaluation and meta-analysis: findings and methodological issues. Libr Q. 1997 Jul. 67(3):267–89. [Google Scholar]
- Light RJ, Pillemer DB. Summing up: the science of reviewing research. Cambridge, MA: Harvard University Press. 1984 [Google Scholar]
- Slavin RE. Best-evidence synthesis: an alternative to meta-analytic and traditional reviews. Educ Res. 1986 Nov. 15(9):5–11. [Google Scholar]
- Slavin RE. Best-evidence synthesis: why less is more. Educ Res. 1987 May. 16(4):15–6. [Google Scholar]
- Tversky A, Kahneman D.. Belief in the law of small numbers. Psychol Bull. 1971;76(2):105–10. [Google Scholar]
- Farmer J, Booth A, Madge B, and Forsythe E. What is the Health Libraries Group doing about research? Health Libr Rev. 1998 Jun. 15(2):139–41. [Google Scholar]
- Booth A, Haines M. Room for a review? Libr Assoc Rec. 1998 Aug. 100(8):411–2. [Google Scholar]
- Hersh WR, Hickam DH. How well do physicians use electronic information retrieval systems: a framework for investigation and systematic review. JAMA. 1998 Oct 21. 280(115):1347–52. [DOI] [PubMed] [Google Scholar]
- Rothman KJ, Greenland S. Modern epidemiology. 2d ed. Philadelphia, PA: Lippincott-Raven. 1998 524. [Google Scholar]
- Fletcher RH, Fletcher SW, and Wagner EH. Clinical epidemiology: the essentials. 3d ed. Baltimore: Williams & Wilkins. 1996 138–52. [Google Scholar]
- Friedman LM, Furberg CD, and DeMets DL. Fundamentals of clinical trials. 3d ed. St Louis, MO: Mosby. 1996 2. [Google Scholar]
- Friedman LM, Furberg CD, and DeMets DL. Fundamentals of clinical trials. 3d ed. St Louis, MO: Mosby. 1996 152–8. [Google Scholar]
- Cook TD, Campbell DT. Quasi-experimentation: design and analysis issues for field settings. Boston, MA: Houghton Mifflin. 1979 341–86. [Google Scholar]
- Riegelman RK, Hirsch RP. Studying a study and testing a test. 3d ed. Boston, Little Brown. 1996 69–91. [Google Scholar]
- Anonymous. Cross design synthesis: a new strategy for studying medical outcomes? Lancet. 1992 Oct 17. 340(8825):944–6. [DOI] [PubMed] [Google Scholar]
- Bailar JC, Mosteller F. Guidelines for statistical reporting in articles for medical journals: amplifications and explanantions. Ann Intern Med. 1988 Feb. 108(2):266–73. [DOI] [PubMed] [Google Scholar]
- Marshall JG, Neufeld VR. A randomized trial of librarian educational participation in clinical settings. J Med Educ. 1981 May. 56(5):409–16. [DOI] [PubMed] [Google Scholar]
- Haynes RB, Ramsden MF, McKibbon KA, and Walker CJ. Online access to MEDLINE in clinical settings: impact of user fees. Bull Med Libr Assoc. 1991 Oct. 79(4):377–81. [PMC free article] [PubMed] [Google Scholar]
- Rosenberg WMC, Deeks J, Lusher A, Snowball R, Dooley G, and Sackett D. Improving searching skills and evidence retrieval. JR Coll Physicians Lond. 1998 Nov–Dec. 32(6):557–63. [PMC free article] [PubMed] [Google Scholar]
- Lichtenstein MJ, Mulrow CD, Elwood PC.. Guidelines for reading case-control studies. J Chronic Dis. 1987;40(9):893–903. doi: 10.1016/0021-9681(87)90190-1. [DOI] [PubMed] [Google Scholar]
- Fletcher RH, Fletcher SW, and Wagner EH. Clinical epidemiology: the essentials. 3d ed. Baltimore: Williams & Wilkins. 1996 212–27. [Google Scholar]
- Gehlbach SH. Interpreting the medical literature. 3d ed. New York, NY: McGraw-Hill. 1993 34–54. [Google Scholar]
- Rothman KJ, Greenland S. Modern epidemiology. 2d ed. Philadelphia, PA: Lippincott-Raven. 1998 93–114. [Google Scholar]
- Buehler JW, Dicker RC. Designing studies in the field. In: Gregg MB, ed. Field epidemiology. New York, NY: Oxford University Press. 1996 81–91. [Google Scholar]
- Young TK. Population health: concepts and methods. New York, NY: Oxford University Press. 1998 173–88. [Google Scholar]
- Line MB.. Critical issues facing LIS journals: a readers' view. IFLA J. 1999;25(1):12–5. [Google Scholar]
- Buchanan HS, Marshall JG. Benchmarking reference services: step-by-step. Med Ref Serv Q. 1996 Spring. 15(1):1–13. [DOI] [PubMed] [Google Scholar]
- Marshall JG, Buchanan HS. Benchmarking reference services: an introduction. Med Ref Serv Q. 1995 Fall. 14(3):59–73. [DOI] [PubMed] [Google Scholar]
- D'Alessandro MP, D'Alessandro DM, Kash JB, Jurca DA, Wakefield DS, Schallau SJ, Galvin JR, and Erkonen WE. A performance comparison of communication links between rural hospitals and a digital health sciences library. Bull Med Libr Assoc. 1998 Oct. 86(4):564–8. [PMC free article] [PubMed] [Google Scholar]
- Eldredge JD. Identifying peer-reviewed journals in clinical medicine. Bull Med Libr Assoc. 1997 Oct. 85(4):418–22. [PMC free article] [PubMed] [Google Scholar]
- Hallett KS. Separate but equal? a system comparison study of MEDLINE's controlled vocabulary MeSH. Bull Med Libr Assoc. 1998 Oct. 86(4):491–5. [PMC free article] [PubMed] [Google Scholar]
- McKnight M. Interlibrary loan availability of nursing journals through DOCLINE and OCLC: a five-state survey. Bull Med Libr Assoc. 2000 Jul. 88(3):254–5. [PMC free article] [PubMed] [Google Scholar]
- Stone VL, Fishman DL, and Frese DB. Searching online and Web-based resources for information on natural products used as drugs. Bull Med Libr Assoc. 1998 Oct. 86(4):523–7. [PMC free article] [PubMed] [Google Scholar]
- Rothman KJ, Greenland S. Modern epidemiology. 2d ed. Philadelphia, PA: Lippincott-Raven. 1998 524. [Google Scholar]
- Dawber TR. The Framingham Study: the epidemiology of atherosclerotic disease. Cambridge, MA: Harvard University Press. 1980 [Google Scholar]
- Rothman KJ, Greenland S. Modern epidemiology. 2d ed. Philadelphia, PA: Lippincott-Raven. 1998 524. [Google Scholar]
- Clark DL. Extinction of conodonts. J Paleontol. 1983 Jul. 57(4):652–61. [Google Scholar]
- Burrows SC, Tylman V. Evaluating medical student searches of MEDLINE for evidence-based information: process and application of results. Bull Med Libr Assoc. 1999 Oct. 87(4):471–6. [PMC free article] [PubMed] [Google Scholar]
- Rankin JA. Problem-based medical education: effect on library use. Bull Med Libr Assoc. 1992 Jan. 80(1):36–43. [PMC free article] [PubMed] [Google Scholar]
- Noesgaard C, Bayley L, Blythe J, Dzugan R, Lunyk-Child O, and Royle JA. et al. Nursing students' use and comfort with computer technology. Bibl Med Can. 1999 Fall. 21(1):231–8. [Google Scholar]
- Bowden VM, Kromer ME, and Tobia RC. Assessment of physicians' information needs in five Texas counties. Bull Med Libr Assoc. 1994 Apr. 82(2):189–96. [PMC free article] [PubMed] [Google Scholar]
- Curtis KL, Weller AC, and Hurd JM. Information-seeking behavior of health sciences faculty: the impact of new information technologies. Bull Med Libr Assoc. 1997 Oct. 85(4):402–10. [PMC free article] [PubMed] [Google Scholar]
- D'Alessandro DM, Qian F, D'Alessandro MP, Ostrem SF, Choi TA, Erkonen WE, and Galvin JR. Performing continuous quality improvement for a digital health sciences library through an electronic mail analysis. Bull Med Libr Assoc. 1998 Oct. 86(4):594–601. [PMC free article] [PubMed] [Google Scholar]
- Dorsch JL, Pifalo V. Information needs of rural health professionals: a retrospective use study. Bull Med Libr Assoc. 1997 Oct. 85(4):341–7. [PMC free article] [PubMed] [Google Scholar]
- Harbourt AM, Knecht LS, and Humphreys BL. Structured abstracts in MEDLINE, 1989–1991. Bull Med Libr Assoc. 1995 Apr. 83(2):190–5. [PMC free article] [PubMed] [Google Scholar]
- Blecic DD. Monograph use at an academic health sciences library: the first three years of shelf life. Bull Med Libr Assoc. 2000 Apr. 88(2):145–51. [PMC free article] [PubMed] [Google Scholar]
- Morse DH, Clintworth WA. Comparing patterns of print and electronic journal usage in an academic health science library. Contributed paper presented at: The Annual Joint Meeting of the Medical Library Group of Southern California and Arizona and the Northern California and Nevada Medical Library Group. 2000 Feb 11 San Diego, CA. [Google Scholar]
- Marshall JG. The impact of the hospital library on clinical decision making: the Rochester study. Bull Med Libr Assoc. 1992 Apr. 80(2):169–78. [PMC free article] [PubMed] [Google Scholar]
- Prior T. Comparing and justifying paid MEDLINE subscription services versus free MEDLINE. Bibl Medica Can. 1999 Summer. 20(4):189–91. [Google Scholar]
- Fink A, Bourque LB, Fiedler EP, Frey JH, Oishi SM, and Litwin MS. The survey kit (9 vols). Thousand Oaks, CA: Sage Publications. 1995 [Google Scholar]
- Silverstein C, Shieber SM.. Predicting individual book use for off-site storage using decision trees. Libr Q. 1996;66(3):266–93. [Google Scholar]
- Stokey E, Zeckhauser R. A primer for policy analysis. New York, NY: Norton. 1978 202–54. [Google Scholar]
- Richardson WS, Detsky AS. Users' guides to the medical literature. VII. how to use a clinical decision analysis. JAMA. 1995 May 24/31. 273(20):1610–3. [DOI] [PubMed] [Google Scholar]
- Tucker AW, Haddix AC, Bresee JS, Holman RC, Parashar UD, and Glass RI. Cost-effectiveness analysis of a rotavirus immunization program for the United States. JAMA. 1998 May 6. 279(17):1371–6. [DOI] [PubMed] [Google Scholar]
- Emanuel LL. Facing requests for physician-assisted suicide. JAMA. 1998 Aug 19. 280(7):643–7. [DOI] [PubMed] [Google Scholar]
- Benitez-Bribiesca L. Are case reports obsolete? Arch Med Res. 1998 Summer. 29(2):105–7. [PubMed] [Google Scholar]
- Line MB.. Critical issues facing LIS journals: a readers' view. IFLA J. 1999;25(1):12–5. [Google Scholar]
- Yin RK. Case study research: design and methods. Rev. ed. Newbury Park, CA: Sage Publications. 1989 [Google Scholar]
- Bradley J. Methodological issues and practices in qualitative research. Libr Q. 1993 Oct. 63(4):431–49. [Google Scholar]
- Robbins K, Holst R. Hospital library evaluation using focus group interviews. Bull Med Libr Assoc. 1990 Jul. 78(3):311–3. [PMC free article] [PubMed] [Google Scholar]
- Mullaly-Quijas P, Ward DH, and Woelfl N. Using focus groups to discover health professionals' information needs: a regional marketing study. Bull Med Libr Assoc. 1994 Jul. 82(3):305–11. [PMC free article] [PubMed] [Google Scholar]
- Glitz B. The focus group technique in library research: an introduction. Bull Med Libr Assoc. 1997 Oct. 85(4):385–90. [PMC free article] [PubMed] [Google Scholar]
- McKnight M, Peet M. Information seeking behavior of doctors, nurses, and other healthcare providers: what we know from recent research. Med Ref Serv Q. Accepted for publication. [Google Scholar]
- Boulton M, Fitzpatrick R. Evaluating qualitative research. Evid Based Health Pol Manage. 1997 Dec. 1(4):83–5. [Google Scholar]
- Canadian Task Force on the Periodic Health Examination. The periodic health exam. Can Med Assoc J. 1979 Nov 3. 121:1193–254. [PMC free article] [PubMed] [Google Scholar]
- Marriott R. Providing library support for the development of clinical guidelines. Health Libr Rev. 1999 Jun. 16(2):132–4. [DOI] [PubMed] [Google Scholar]
- Singer AJ, Homan CS, Stark MJ, Werblud MC, Thode HC, and Hollander JE. Comparison of types of research articles published in emergency medicine and non-emergency medicine journals. Acad Emerg Med. 1997 Dec. 4(12):1153–8. [DOI] [PubMed] [Google Scholar]
- Maran AGD, Molony NC, Armstrong MWJ, and Ah-See K. Is there an evidence base for the practice of ENT surgery? Clin Otolaryngol. 1997 Apr. 22(2):152–7. [DOI] [PubMed] [Google Scholar]
- Ah-See KW, Molony NC. A qualitative assessment of randomized controlled trials in Otolaryngology. J Laryngol Otol. 1998 May. 112(2):460–3. [DOI] [PubMed] [Google Scholar]
- Horan BF. Evidence-based medicine and anesthesia: uneasy bedfellows? Anaesth Intensive Care. 1997 Dec. 25(6):679–85. [DOI] [PubMed] [Google Scholar]
- Childs C. Is there an evidence-based practice for burns? Burns. 1998 Feb. 24(1):29–33. [DOI] [PubMed] [Google Scholar]
- Solomon MJ, Laxaman A, Devore L, and McLeod RS. Randomized controlled trials in surgery. Surgery. 1994 Jun. 115(6):707–12. [PubMed] [Google Scholar]
- Solomon MJ, McLeod RS. Surgery and the randomized controlled trial: past, present and future. Med J Aust. 1998 Oct 5. 169(7):380–3. [DOI] [PubMed] [Google Scholar]
- Brazier H, Murphy AW, Lynch C, and Bury G. Searching for the evidence in pre-hospital care: a review of randomized controlled trials. J Accid Emerg Med. 1999 Jan. 16(1):18–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Callaham M. Quantifying the scanty science of prehospital emergency care. Ann Emerg Med. 1997 Dec. 30(6):785–90. [DOI] [PubMed] [Google Scholar]
- Dauten D. Management by joking around. Albuquerque Journal. 1999 Jul 7 Sect. D:1. [Google Scholar]