

Abstract
Objectives:
To assess the practicability of a new algorithm in decreasing the rate of incorrect diagnoses and inappropriate antibiotic usage in pediatric Acute Respiratory Tract Infection (ARTI).
Materials and Methods:
Children between 1 month to15 years brought to outpatient clinics of a children's hospital with acute respiratory symptoms were managed according to the steps recommended in the algorithm.
Results:
Upper Respiratory Tract Infection, Lower Respiratory Tract Infection, and undifferentiated ARTI accounted for 82%, 14.5%, and 3.5% of 1 209 cases, respectively. Antibiotics were prescribed in 33%; for: Common cold, 4.1%; Sinusitis, 85.7%; Otitis media, 96.9%; Pharyngotonsillitis, 63.3%; Croup, 6.5%; Bronchitis, 15.6%; Pertussis-like syndrome, 82.1%; Bronchiolitis, 4.1%; and Pneumonia, 50%.
Conclusion:
Implementation of the ARTIs algorithm is practicable and can help to reduce diagnostic errors and rate of antibiotic prescription in children with ARTIs.
Keywords: Acute respiratory tract infection, algorithm, children
INTRODUCTION
Acute Respiratory Tract Infections (ARTIs) are the most common reasons for children visiting a physician, leading to increased utilization of health services including hospital admissions.[1] Furthermore, Lower Respiratory Tract Infections (LRTI) are major cause of morbidity and mortality (25%-50%) in developing countries.[2–4] Incidence rates of ARI in children of developing and developed countries are comparable, but cause-specific mortality rates from ARTIs are 10 to 50 times higher in underdeveloped countries.[5,6]
However, most childhood ARTIs have a viral etiology.[7,8] They are the principal reason for antibiotic prescriptions in the pediatric population (e.g., 46% in a Dutch study[9]) resulting in increasing bacterial resistance, adverse drug effects, and increased financial burden.
Facilities for identifying various organisms are totally lacking in underdeveloped societies, and limited in transitional countries. WHO has initiated a program for clinical management and control of ARTIs which has resulted in the reduction of ARTI mortality rates by 25% to 67%.[4,10,11] Some countries have programmed to recommend guidelines approach to ARITs.[12–14] We developed an algorithm for the diagnosis of ARTIs in children solely based on clinical manifestations, with minimal use of laboratory facilities and the main objective of this study was to assess the practicability of this algorithm, how much the ARITs and antibiotics usage are common and in comparison with other studies could it reduce the rate of incorrect diagnoses and inappropriate antibiotic usage.
MATERIALS AND METHODS
This prospective cross-sectional study was conducted from October 2007 to September 2008, on children aged between one month and 15 years with acute respiratory symptoms, cough, fever, hoarseness, and nasal discharge with or without tachypnea, in the outpatients clinics of a university-affiliated children's hospital in Tehran.
ARTI was defined as respiratory symptoms lasting < 3 weeks. All consecutive patients above the age of one month and below the age of 15 years with ARTIs symptoms brought to the outpatients clinics were included and patients with more than 3 weeks’ signs and symptoms, chronic lung or heart diseases, and primary or secondary immunodeficiency were excluded. Informed consent was obtained from the parents before inclusion in the study.
Demographic and clinical data were collected from the visit notes. Algorithm designed for this study was derived from clinical manifestations of ARTIs described in the Nelson Textbook of Pediatrics.[15] In this algorithm, the physician categorizes the patients into lower and upper ARTI according to respiratory rate and lung findings on auscultation [Figure 1].
Figure 1.
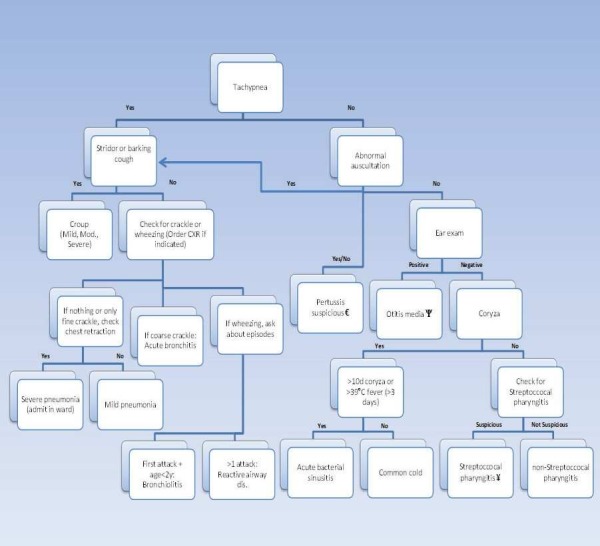
Acute Respiratory Tract Infection Algorithm; ψ presence of ≥2 following criteria: a) otic pain or irritability, b) redness of tympanic membrane, c) absence of tympanic membrane landmarks like incus, promontory, cone of light, d) bulging of tympanic membrane or perforated membrane; €presence of ≥2 following criteria: a) recent family history of cough ≥2 weeks, b) paroxysmal cough attacks with no sigh between them, c) post cough emesis, d) presence of whooping or apnea after cough attacks; ¥presence of ≥2 following criteria: age between 5 to 15 years old, b) exudative pharyngitis, c) tenderness of anterior neck adenitis, d) high-grade fever (tem ≥39°C)
Tachypnea was defined according to the standard reference charts set by the WHO for different age groups and fever as an axillary temperature of >38°C.
Trained physicians examined the patients and classified them according to the algorithm into nine primary diagnoses:
Upper Respiratory Tract Infections (URTIs): Common Cold, Sinusitis, Otitis media, and Pharyngotonsillitis.
Lower Respiratory Tract Infections (LRTIs): Croup, Bronchitis, Pertussis-like syndrome, Bronchiolitis, and Pneumonia.
All data were fed into the computer and analyzed by SSPS 11.5 software (Chicago, USA). The study variables were categorical and were summarized as frequency and percentages.
RESULTS
The algorithm was used for management of 1 209 patients, Male: female = 1.2: 1; and 44.8% were <2 years. URTI, LRTI, and Undifferentiated ARTI accounted for 996 (82%), 176 (14.5%), and 42 (3.5%) cases, respectively. Specific diagnoses are presented in [Figure 2].
Figure 2.
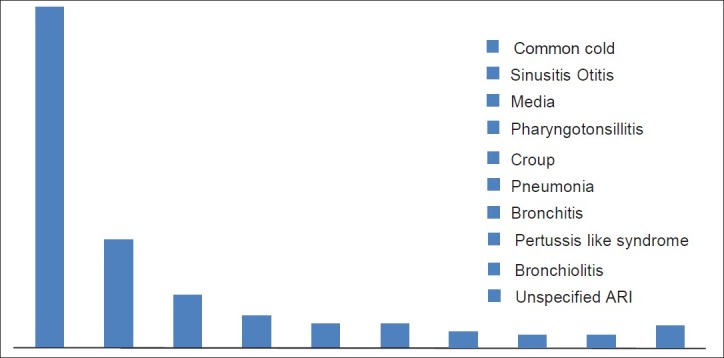
Acute Respiratory tract infection frequency
Antibiotics were prescribed in 33% of all visits; rates of antibiotic prescription in URTI were: Common cold, 4.1%; Sinusitis, 85.7%; Otitis media, 96.9%; and Pharyngotonsillitis, 63.3%. For LRTIs: Croup, 6.5%; Bronchitis, 15.6%; Pertussis- like syndrome, 82.1%; Bronchiolitis, 4.1%; and Pneumonia, 50% [Table 1]. Clinicians prescribed antibiotics in 33% of all visits. Most commonly used antibiotics were amoxicillin/ clavulanate (34.5%), amoxicillin (20.8%), azithromycin (17.5%), erythromycin (8.7%), and penicillin (8.5%).
Table 1.
Frequency of antibiotic usage in acute respiratory tract infections

DISCUSSION
By using the recommended algorithm, physicians prescribed antibiotics for approximately one-third of children with ARTI. These figures are in sharp contrast to another study in our center, which reported antibiotic prescription rate of >80% in children with ARTI.[16] ARTIs are the number one reason for antibiotic prescribing in the United States accounting for about 50% of all antibiotic prescription.[17] As reported from Scandinavia, prescribing patterns for ARTIs vary widely between physicians.[18] Antibiotic therapy in ARTIs is often guided by clinical manifestations as etiological pathogens may remain undiscovered in most cases even if all invasive diagnostic steps were taken.[19,20] Also, cultural factors such as prescribing practices, parents’ expectations, and structure of the healthcare system may result in differences in clinical practice and antibiotic consumption between countries.[21,22]
Some physicians prescribe antimicrobials for bronchitis if the child complains of productive cough, although controlled trials have failed to demonstrate the benefit of antibiotic treatment for acute bronchitis.[23] The belief that purulent nasal discharge is an indication for antibiotics seems to be common, despite evidence that purulence of nasal discharge does not indicate bacterial infection.[24,25]
Our research team had attempted to reduce antibiotic prescribing for respiratory tract infections by an educational intervention similar to some other studies.[26,27] Studies have shown the importance of parental demands for antibiotic treatment, and trials that included educational interventions for both parents and physicians had promising results, with Smabrekke et al. demonstrating a reduction in antibiotic prescriptions for acute otitis media, from 90% to 74%, and also a reduction in broad-spectrum antibiotic use.[28–30]
Our findings reveal that using the suggested algorithm is practicable, and may be effective in defining various forms of ARI more clearly, thereby improving antibiotic prescription patterns for these infections in children. The main limitation of our study is the lack of a control group that was managed without using the algorithm; however, as stated above, a previous study done in the same hospital, which investigated antibiotic usage in outpatients with acute respiratory infections, does show a very high rate of antibiotic prescription, prior to the use of the algorithm.[16] Further multi-central researches and control group are necessary.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Naghipour M, Cuevasb LE, Bakhshinejada T, Mansour-Ghanaei F, Noursalehi S, Alavy A, et al. Contribution of Viruses, Chlamydia spp. And Mycoplasma pneumoniae to Acute Respiratory Infections in Iranian Children. J Trop Pediatr. 2007;53:179–84. doi: 10.1093/tropej/fml089. [DOI] [PubMed] [Google Scholar]
- 2.Pio A, Leomski J, Ten Dam HG. The magnitude of the problem of acute respiratory infections. In: Douglas R, editor. Acute respiratory infections in children. Proceedings of an international workshop. Adelaide, Australia: University of Adelaide; 1985. pp. 3–16. [Google Scholar]
- 3.Garenn M, Ronsmans C, Campbell H. The magnitude of mortality from acute respiratory infection in children under 5 years in developing countries. World Health State Q. 1992;45:180–91. [PubMed] [Google Scholar]
- 4.World Health Organization. Clinical management of acute respiratory infection in children: A WHO memorandum. Bull WHO. 1981;59:707–16. [PMC free article] [PubMed] [Google Scholar]
- 5.World Health Organization. A programme for controlling acute respiratory infections in children. Memorandum from a WHO meeting. Bull World Health Organ. 1984;62:47–58. [PMC free article] [PubMed] [Google Scholar]
- 6.Mohs E. Acute respiratory infections in children: Possible control measures. Bull Pan Am Health Organ. 1985;19:82–7. [PubMed] [Google Scholar]
- 7.Van Gageldonk-Lafeber AB, Heijnen ML, Bartelds AI, Peters MF, Van der Plas SM, Wilbrink B. A case-control study of acute respiratory tract infection in general practice patients in the Netherlands. Clin Infect Dis. 2005;41:490–7. doi: 10.1086/431982. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Farha T, Thomson AH. The burden of pneumonia in children in the developed world. Paediatr Respir Rev. 2005;6:76–82. doi: 10.1016/j.prrv.2005.03.001. [DOI] [PubMed] [Google Scholar]
- 9.Akkerman AE, van der Wouden JC, Kuyvenhoven MM, Dieleman JP, Verheij TJ. Antibiotic prescribing for respiratory tract infection in Dutch primary care in relation to patient age and clinical entities. J Antimicrob Chemother. 2004;54:116–21. doi: 10.1093/jac/dkh480. [DOI] [PubMed] [Google Scholar]
- 10.Stansfield SK. Acute respiratory infection in the developing world: Strategies for prevention, treatment and control. Pediatr Infect Dis J. 1987;6:622–9. doi: 10.1097/00006454-198707000-00002. [DOI] [PubMed] [Google Scholar]
- 11.World Health Organization. A program for controlling acute respiratory infections in children: A WHO memorandum. Bull WHO. 1984;62:47–58. [PMC free article] [PubMed] [Google Scholar]
- 12.RJ Green, Zar HJ, Jeena PM, Madhi SA, Lewis H. South African guideline for the diagnosis, management and prevention of acute viral bronchiolitis in children. S Afr Med J. 2010;100:320, 322–5. doi: 10.7196/samj.4016. [DOI] [PubMed] [Google Scholar]
- 13.Regoli M, Chiappini E, Bonsignori F, Galli L, de Martino M. Update on the management of acute pharyngitis in children. Ital J Pediatr. 2011;37:10. doi: 10.1186/1824-7288-37-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Werner K, Deasy J. Acute respiratory tract infections: When are antibiotics indicated?. JAAPA. 2009;22:22–6. doi: 10.1097/01720610-200904000-00007. [DOI] [PubMed] [Google Scholar]
- 15.Kliegman RM, Stanton BF, St. Geme Joseph W, III, Schor NF, Behrman RE. 18th ed. Nelson Textbook of Pediatrics. Part 18 , section 2. [Google Scholar]
- 16.Shiva F, Eidikhani A, Padyab M. Prescription practices in acute pediatric infections. J Pediatr Infect Dis. 2006;1:25–8. [Google Scholar]
- 17.Steinman MA, Gonzales R, Linder JA, Landefeld CS. Changing use of antibiotics in community-based outpatient practice 1991-1999. Ann Intern Med. 2003;138:525–33. doi: 10.7326/0003-4819-138-7-200304010-00008. [DOI] [PubMed] [Google Scholar]
- 18.CDC: The CAUSE (careful antibiotic use to prevent resistance) [Last cited on 1997 Oct day]. Available from: http://www.cdc.gov/ncidod/dbmd/cause/oct97.htm .
- 19.Lidman C, Burman LG, Lagergren A, Ortqvist A. Limited value of routine microbiological diagnostics in patients hospitalized for community-acquired pneumonia. Scand J Infect Dis. 2002;34:873–9. doi: 10.1080/0036554021000026967. [DOI] [PubMed] [Google Scholar]
- 20.McKean MC. Evidence based medicine: Review of BTS guidelines for the management of community acquired pneumonia in adults. J Infect. 2002;45:213–8. doi: 10.1053/jinf.2002.1060. [DOI] [PubMed] [Google Scholar]
- 21.Christiaens T, De Backer D, Burgers J, Baerheim A. Guidelines, evidence, and cultural factors. Scand J Prim Health Care. 2004;22:141–5. doi: 10.1080/02813430410006521. [DOI] [PubMed] [Google Scholar]
- 22.Visvanathan V, Nix P. National UK survey of antibiotics prescribed for acute tonsillitis and peritonsillar abscess. J Laryngol Otol. 2010;124:420–3. doi: 10.1017/S0022215109991939. [DOI] [PubMed] [Google Scholar]
- 23.Orr PH, Scherer K, Macdonald A, Moffatt ME. Randomized placebocontrolled trials of antibiotics for acute bronchitis: A critical review of the literature. J Fam Pract. 1993;36:507–12. [PubMed] [Google Scholar]
- 24.Wald ER, Milmoe GJ, Bowen A, Ledesma-Medina J, Salamon N, Bluestone CD. Acute maxillary sinusitis in children. N Engl J Med. 1981;304:749–54. doi: 10.1056/NEJM198103263041302. [DOI] [PubMed] [Google Scholar]
- 25.Wald ER. Purulent nasal discharge. Pediatr Infect Dis J. 1991;10:329–33. doi: 10.1097/00006454-199104000-00013. [DOI] [PubMed] [Google Scholar]
- 26.Munck AP, Gahrn-Hansen B, Sogaard P, Søgaard J. Long lasting improvement in general practitioners’ prescribing of antibiotics by means of medical audit. Scand J Prim Health Care. 1999;7:185–90. doi: 10.1080/028134399750002629. [DOI] [PubMed] [Google Scholar]
- 27.Finkelstein JA, Stille C, Nordin J, Davis R, Raebel MA, Roblin D, et al. Reduction in antibiotic use among US children. Pediatrics. 2003;112:620–7. doi: 10.1542/peds.112.3.620. [DOI] [PubMed] [Google Scholar]
- 28.Smabrekke L, Berild D, Giaever A, Myrbakk T, Fuskevåg A, Ericson JU, et al. Educational intervention for parents and health care providers leads to reduced antibiotic use in acute otitis media. Scand J Infect Dis. 2002;34:657–9. doi: 10.1080/00365540210147651. [DOI] [PubMed] [Google Scholar]
- 29.Perz JF, Craig AS, Coffey CS, Jorgensen DM, Mitchel E, Hall S, et al. Changes in antibiotic prescribing for children after a community-wide campaign. JAMA. 2002;287:3103–9. doi: 10.1001/jama.287.23.3103. [DOI] [PubMed] [Google Scholar]
- 30.Panagakou SG, Spyridis N, Papaevangelou V, Theodoridou KM, Goutziana GP, Theodoridou MN, et al. Antibiotic use for upper respiratory tract infections in children: A cross-sectional survey of knowledge, attitudes, and practices (KAP) of parents in Greece. BMC Pediatr. 2011;5:1–10. doi: 10.1186/1471-2431-11-60. [DOI] [PMC free article] [PubMed] [Google Scholar]