

Abstract
Introduction: Primary access libraries serve as the foundation of the National Network of Libraries of Medicine (NN/LM) interlibrary loan (ILL) hierarchy, yet few published reports directly address the important role these libraries play in the ILL system. This may reflect the traditional view that small, primary access libraries are largely users of ILL, rather than important contributors to the effectiveness and efficiency of the national ILL system.
Objective: This study was undertaken to test several commonly held beliefs regarding ILL system use by primary access libraries.
Hypotheses: Three hypotheses were developed. H1: Colorado and Wyoming primary access libraries comply with the recommended ILL guideline of adhering to a hierarchical structure, emphasizing local borrowing. H2: The closures of two Colorado Council of Medical Librarians (CCML) primary access libraries in 1996 resulted in twenty-three Colorado primary access libraries' borrowing more from their state resource library in 1997. H3: The number of subscriptions held by Colorado and Wyoming primary access libraries is positively correlated with the number of items they loan and negatively correlated with the number of items they borrow.
Methods: The hypotheses were tested using the 1992 and 1997 DOCLINE and OCLC data of fifty-four health sciences libraries, including fifty primary access libraries, two state resource libraries, and two general academic libraries in Colorado and Wyoming. The ILL data were obtained electronically and analyzed using Microsoft Word 98, Microsoft Excel 98, and JMP 3.2.2.
Results: CCML primary access libraries comply with the recommended guideline to emphasize local borrowing by supplying each other with the majority of their ILLs, instead of overburdening libraries located at higher levels in the ILL hierarchy (H1). The closures of two CCML primary access libraries appear to have affected the entire ILL system, resulting in a greater volume of ILL activity for the state resource library and other DOCLINE libraries higher up in the ILL hierarchy and highlighting the contribution made by CCML primary access libraries (H2). CCML primary access libraries borrow and lend in amounts that are proportional to their collection size, rather than overtaxing libraries at higher levels in the ILL hierarchy with large numbers of requests (H3).
Limitations: The main limitations of this study were the small sample size and the use of data collected for another purpose, the CCML ILL survey.
Conclusions: The findings suggest that there is little evidence to support several commonly held beliefs regarding ILL system use by primary access libraries. In addition to validating the important contributions made by primary access libraries to the national ILL system, baseline data that can be used to benchmark current practice performance are provided.
INTRODUCTION
A fact of library management is that no library can own everything required by a varied clientele. Interlibrary loan (ILL), the exchange of resources between libraries, provides access to other library collections. In the mid-1970s, automated borrowing and lending systems were developed to enable libraries to meet more quickly and efficiently the needs of their clientele for remote resources.
The library literature contains numerous reports of borrowing and lending among large academic libraries, including academic health sciences libraries; however, relatively few studies of ILL in primary access libraries have been reported. Primary access libraries serve as the foundation of the National Network of Libraries of Medicine (NN/LM) hierarchical borrowing and lending structure. Subsequent tiers of the structure consist of state and regional resource libraries, typically academic health sciences libraries, with the National Library of Medicine (NLM) alone in the top tier [1]. According to NLM, there are approximately 4,500 primary access libraries in the United States [2].
The Colorado Council of Medical Librarians (CCML) membership represents multi-type libraries from health care, industry, and academia as well as information brokers and vendors. CCML defines primary access libraries as non-academic, either hospital-based or other small health sciences–related libraries, including libraries in professional associations, research organizations, outpatient facilities, and businesses that serve the information needs of the health professionals associated with the library or its institution. CCML has a long history of promoting efficient ILL use by its members. In 1977, what would become an ongoing series of ILL surveys was initiated to provide a mechanism for promoting balanced ILL activity among member libraries. The fourth and fifth CCML ILL surveys, used in this study, included fifty primary access libraries, as well as two state resource libraries and two general academic libraries in Colorado and Wyoming.
PURPOSE OF THE STUDY
After completing the 1997 CCML ILL survey and making recommendations to the membership for improving ILL procedures [3], the CCML ILL task force members wanted to explore several commonly held beliefs about ILL use in primary access libraries. The following questions, based on the traditional view of ILL in primary access libraries, were identified:
Are small, primary access libraries a burden to the ILL system, borrowing primarily from larger libraries and contributing comparatively little to the system?
When a primary access library closes, are the majority of ILLs that would have been supplied by that library filled by its peer libraries, or must they be referred to larger libraries to be filled? If so, are large resource libraries burdened by this influx of additional requests?
Do small, primary access libraries with fewer journal subscriptions borrow more and lend less, proportionately, than larger libraries? If small libraries purchased more journals, would they borrow significantly less from larger libraries?
LITERATURE REVIEW
Studies of ILL borrowing and lending statistics have been reported for the United States [4, 5], for NLM [6, 7], and for academic and research libraries [8–13]. A relatively small number of studies of ILL in health sciences libraries, particularly primary access libraries, has been reported in the literature.
Two studies of ILL in primary access libraries examined ILL requests at the journal title or article level. In 1975, Morton [14] analyzed borrowing requests made by hospital libraries in central and western Massachusetts. Each hospital library supplied the journal titles and years of publication for articles requested during 1975. Similar to a national study published by Lacroix in 1994 [15], this study concluded that a large number of journals were required to fill ILL requests. This study also determined that most ILL requests were for recently published items, and that the collections of primary access and regional libraries were adequate to fill most hospital library ILL requests.
In 1976, Clevesy and Inglis [16] analyzed ILL data from member libraries of the Consortium for Information Resources (CIR), including eleven community hospital primary access libraries in the West Suburban Hospital Association of Greater Boston. This report indicated that 72% of requested journal articles were published during the most recent five years, and that approximately 91% of requested journal titles were requested five or fewer than 5 times during the six-year survey period.
In the early 1970s, NLM curtailed reimbursement to resource libraries for supplying ILLs to smaller libraries and encouraged primary access libraries to form consortia to meet more of their own needs for biomedical information and to decrease their dependence on larger resource libraries. Several papers examined the effect of this strategy on primary access libraries' borrowing patterns. In a 1976 paper in Hospital Libraries, Monroe [17] reviewed lending data for academic health sciences libraries and primary access libraries located in Kentucky, Ohio, and Michigan. From 1973 to 1974, total lending by the primary access libraries significantly increased, while total lending by the nine academic libraries decreased moderately.
In 1978, Mundt [18] described the impact of joining the Illinois Health Libraries Consortium on the ILL activity of the library of the Health and Hospitals Governing Commission (HHGC) in Chicago. Data showed that, after one year of participation in the consortium, the HHGC library had significantly increased borrowing from other consortium members and decreased borrowing from local resource libraries.
The development of the Twin Cities Biomedical Consortium in metropolitan Minneapolis, in the early 1970s, resulted in its twenty-eight primary access library members' borrowing more from each other and less from larger academic and resource libraries. In a 1975 study, Bailey and Tibbetts [19] reviewed consortium ILL data for a six-month period. From May to October 1974, total loans filled by consortium libraries increased 217%, while total loans filled by nonmember resource libraries increased only 0.8%. The authors extrapolated that by December 1974, the membership would fill more than 50% of their ILL requests.
Only one study was found that quantified primary access libraries' borrowing from each other in comparison to their borrowing from larger resource libraries. A 1966 study of the Metropolitan Detroit Biomedical Network [20] examined ILL data for twenty-nine network member libraries, including twenty-five hospital-based primary access libraries and the state resource library, for the six-month period, January to June 1966. Four percent of their total ILLs were supplied by primary access network member libraries, and 58% were supplied by Wayne State University Medical Library (now Shiffman Medical Library), the Michigan state resource library. An additional 10% of ILLs were supplied by nonnetwork institutions located in the Detroit metropolitan area. NLM supplied 6% of the requested items.
A recent paper by Felber et al. [21] described SouthEastern Network on DOCLINE (SEND), a group of eighty-seven primary access libraries, who are members of the Southern Chapter of the Medical Library Association. This reciprocal ILL network was established to maximize the lending potential of its members' basic health sciences collections, by using structured DOCLINE routing tables to promote balanced ILL traffic.
This review of the literature confirmed that the questions regarding primary access libraries and ILL had not been adequately addressed. In addition, the small number of identified ILL surveys of primary access health sciences libraries suggested a need for more research into the role that primary access libraries play in the national ILL system.
HYPOTHESES
H1: Colorado and Wyoming primary access libraries comply with the recommended interlibrary loan (ILL) guideline of adhering to a hierarchical structure, emphasizing local borrowing
H2: The closures of two Colorado Council of Medical Librarians (CCML) libraries in 1996 resulted in twenty-three Colorado primary access libraries' borrowing more from their state resource library in 1997
H3: The number of subscriptions held by Colorado and Wyoming primary access libraries is positively correlated with the number of items they loan and negatively correlated with the number of items they borrow
METHODOLOGY
The CCML ILL surveys have never been limited to CCML members but have attempted to include all health sciences libraries in the state of Colorado and, in 1997, Wyoming. To identify potential survey participants for the 1997 CCML ILL survey, the NLM Document Delivery User (DOCUSER) database was searched, yielding 166 records for libraries in Colorado and Wyoming. DOCUSER—NLM's online database of directory, ILL, and network membership data—supports DOCLINE routing by providing profile information for participating libraries [22]. CCML had a membership in 1997 representing sixty-seven institutions and businesses, not all of which were DOCLINE users. DOCUSER was searched to identify potential survey participants who were not listed in the CCML membership directory and to exclude CCML members who did not use DOCLINE. The survey used only figures collected electronically from DOCLINE with no self-reported statistics.
Of the Colorado and Wyoming libraries identified in DOCUSER, there were eighty-nine non-active DOCLINE user libraries and seventy-seven active users. Because maintenance of the DOCUSER database was done by the participating libraries, the active or non-active status was often inaccurate. Also, official CCML membership changed every year due to nonpayment of dues. The seventy-seven active users were analyzed; four libraries were known to have ceased operation; and nine others, all located in Wyoming, were reported to have ceased operation, leaving sixty-four. Eight other active libraries, although still in existence, were identified by the CCML ILL Task Force as non-DOCLINE users, even though they were listed as active, leaving a pool of fifty-six potential participants, forty-three of which were represented by CCML members.
In November 1997, letters soliciting survey participants were mailed to these fifty-six libraries. Libraries were asked to supply information such as their institution type and number of subscriptions as well as DOCLINE and OCLC login IDs and passwords. Table 1 lists the characteristics of the study group of libraries. DOCLINE is NLM's automated document request and referral system. Online Computer Library Center (OCLC) is a nonprofit electronic network that provides an ILL subsystem for participating libraries to borrow and lend materials.
Table 1 Characteristics of the 1997 CCML study group of fifty primary access libraries
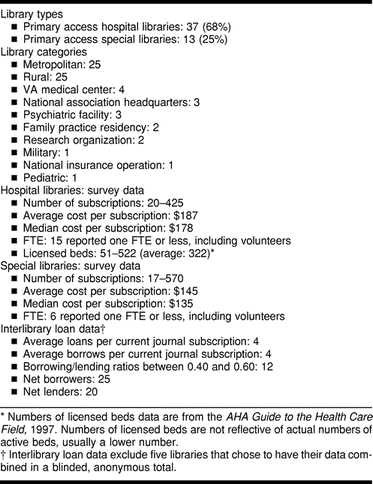
By February 1998, fifty-five libraries had returned letters of agreement. One corporate library declined to participate. Another library that agreed to participate in the study had not used DOCLINE or OCLC in 1997 and therefore was excluded. Of the fifty-four final survey participants, two were state resource libraries; two were general academic libraries; thirteen were primary access special libraries; and thirty-seven were primary access hospital libraries.
The letters of agreement were forwarded to NLM staff, who transferred the DOCLINE data to the CCML ILL Task Force in electronic form. Four text-based files (All Borrowing Activity [1.1MB], All Lending Activity [650K], Borrowing Summary [130K], and Lending Summary [130K]) were created and transferred via file transfer protocol (ftp) making this the first CCML ILL survey in which data were transferred electronically. The four text files were revised in Microsoft® Word 98 by replacing all spaces with tab delimiters. The files were then imported into a Microsoft Excel 98 spreadsheet using the Text Import Wizard feature. Finally, borrowing and lending files were compared to ensure the accuracy of the data. Similar procedures were followed to obtain and prepare the OCLC ILL data. The Excel Pivot Table function was used to calculate totals of borrowed and loaned items, and separate subsets of the data were created and imported into JMP® 3.2.2. to calculate the Spearman correlation coefficient values.
RESULTS
H1: Colorado and Wyoming primary access libraries comply with the recommended ILL guideline of adhering to a hierarchical structure, emphasizing local borrowing.
In 1997, CCML primary access libraries received 61% of requested ILLs via DOCLINE from their peer CCML libraries and 13% from their state resource libraries, the University of Colorado Health Sciences Center and the University of Wyoming (Figure 1), thereby complying with the guideline to emphasize local borrowing. Ten percent of ILL requests by CCML primary access libraries via DOCLINE were received from the other seven Region 4 resource libraries, 12% from other DOCLINE libraries, and 4% from NLM.
Figure 1.
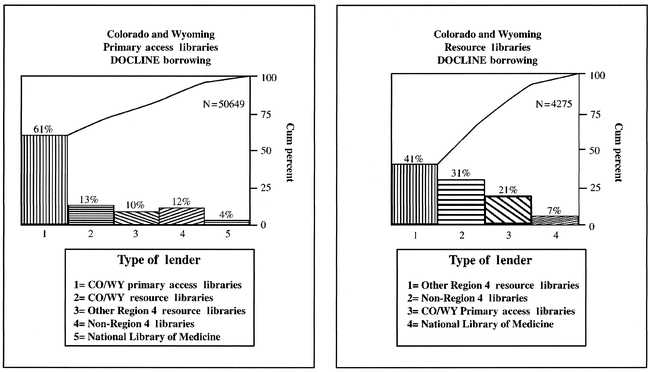
1997 DOCLINE borrowing data, demonstrating the percentage of borrowed items at various levels of the ILL hierarchy
Colorado and Wyoming resource libraries also complied with the recommended guideline. They received 21% of requested ILLs via DOCLINE from CCML primary access libraries and 41% from other Region 4 resource libraries, for a total of 62%. Thirty-one percent of ILL requests by Colorado and Wyoming resource libraries via DOCLINE were supplied by other DOCLINE libraries, and 7% were supplied by NLM.
H2: The closures of two CCML libraries in 1996 resulted in twenty-three Colorado primary access libraries' borrowing more from their state resource library in 1997.
In 1996, two CCML member libraries, Fitzsimons Army Medical Center Library (FAMCL) and Mercy Medical Center Library (MMCL), closed. In order to assess the effect of these library closures on CCML borrowing and lending patterns, the ILL activity of twenty-three CCML libraries, each borrowing more than ten items from FAMCL or MMCL in 1992, was examined.
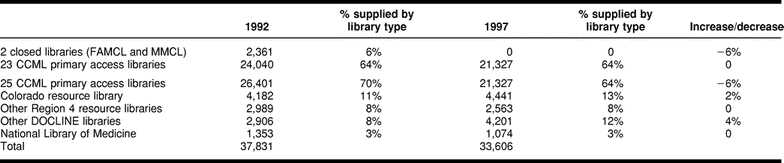
In 1992, the twenty-three libraries received 2,361 ILLs, or 6% of their total ILLs, from FAMCL and MMCL combined. In 1997, borrowing within the group of the twenty-three CCML primary access libraries decreased by 6% (Table 2). The twenty-three libraries borrowed 2% more from their Colorado resource library, while the amount borrowed from other Region 4 resource libraries remained the same. Their borrowing from other DOCLINE libraries increased by 4%, while their level of borrowing from NLM remained the same.
Table 2 1992 and 1997 DOCLINE lending data for twenty-three libraries that each borrowed ten or more resources from FAMCL and MMCL
H3: The number of subscriptions held by Colorado and Wyoming primary access libraries is positively correlated with the number of items they loan, and negatively correlated with the number of items they borrow.
In 1997, the numbers of current journal subscriptions held by CCML primary access libraries ranged from 17 to 570, with hospital libraries averaging 182 subscriptions each. To determine the relationship between collection size and ILL activity, the number of current journal subscriptions, along with borrowing and lending data, were examined for forty-five survey participants. Of the fifty primary access library survey participants, five chose to be blinded and could not be used for this analysis. Figure 2 represents the correlation between the number of subscriptions and numbers of items borrowed and loaned. The correlation between the number of subscriptions held by a CCML primary access library and the number of items it loaned was significantly positive (0.67, P < 0.0001), supporting H3, while the correlation between the number of subscriptions and the number of items borrowed was marginally positive (0.29, P = 0.0523), contradicting H3.
Figure 2.
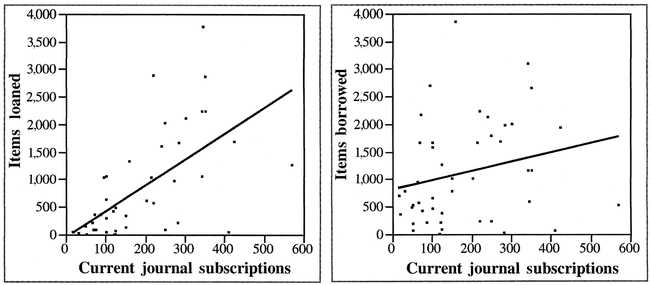
Graphic representation of the correlation between the number of journal subscriptions and the number of items borrowed and the number of items loaned. Legend: Loaned items to journal subscriptions, significantly positive correlation: 0.67 (P < 0.0001). Borrowed items to journal subscriptions, marginally positive correlation: 0.29 (P = 0.0523).
DISCUSSION
With the proliferation of biomedical knowledge and exponential growth in biomedical publications, access to a wide range of information resources has become increasingly important for health professionals. Interlibrary loan enables libraries to provide their users with access to important biomedical resources that are not available in their home libraries. Providing accurate, cost-effective, timely ILL service to their users enables primary access libraries to make a valuable contribution to the quality of patient care and the overall effectiveness of their institutions.
By adhering to recommended ILL practices, primary access libraries play a key role in promoting the efficiency and equity of the ILL system. One recommended ILL practice guideline, designed to promote efficiency and equity, is to borrow from peer and smaller libraries as often as possible, in order to avoid overburdening larger libraries that have more resources. In the second edition of the Interlibrary Loan Practices Handbook [23], Boucher cautions ILL staff to “be reasonable and use common sense in approaching very large research libraries, which customarily supply far more than they borrow. These libraries should be used as a last resort.” Section 4.5 of the National Interlibrary Loan Code for the United States 1993 states, “The requesting library should avoid sending the burden of its requests to a few libraries. Major resource libraries should be used as a last resort” [24]. In volume 3 of the Current Practice in Health Sciences Librarianship series [25], Arnold and Fishel state, “The National Library of Medicine encourages primary access libraries to arrange their DOCLINE routing tables to borrow from each other, before borrowing from state resource libraries, regional resource libraries, and finally, the National Library of Medicine. … Generally, the rule is to exhaust local resources first, before moving outside the local area.”
The literature review discussed above identified only one study, published in 1968 [26], that quantified primary access libraries' borrowing from each other. In a study of the Metropolitan Detroit Network, primary access network libraries supplied each other with only 14% of their total ILLs. Rather than borrowing among themselves, they depended primarily upon the Michigan resource library, which supplied 58% of their ILLs. In contrast, in 1997, CCML primary access libraries supplied each other with 61% of requested ILLs and received only 13% from the Colorado and Wyoming resource libraries. This change over time toward an emphasis on local borrowing is likely due to the efficiency of DOCLINE and OCLC, particularly the ability of these automated systems to promote greater awareness of others' collections and to make borrowing from each other more convenient for smaller libraries.
In a five-year follow-up to the Detroit study, Cruzat stated, “The Detroit Medical Library Group found that there must be a base or standard developed for interlibrary loan service; otherwise, inequities in service will remain” [27]. Even thirty years ago, the importance of a standard was recognized, and the need remains today. The present study provides baseline benchmark data that other primary access libraries and library consortia can use for comparison and evaluation of their own ILL practices to determine how well they adhere to the guideline. The authors of this paper hope that the Medical Library Association's Benchmarking Network, currently in the development stage, will enable primary access health sciences libraries to gather and compare ILL data, identify and work with benchmarking partners, and establish the most efficient, effective practices.
The efficiency of ILL services can be affected by outside influences as well as internal practices. Mergers, institutional restructuring, and changing organizational affiliations have resulted in the closures or downsizing of increasing numbers of hospital and other small biomedical libraries. Yet the literature review found no published studies quantifying the impact of library closures on ILL activity.
Two consortium libraries that were important ILL resources for CCML closed in 1996. Fitzsimons Army Medical Center closed due to cutbacks in military spending by the U.S. government; Mercy Medical Center merged with another hospital and, as a result, closed its library. A comparison of the 1992 and 1997 borrowing and lending data of a subset of CCML primary access libraries revealed that 6% of ILLs that likely would have been supplied by FAMCL and MMCL, based on 1992 patterns, were redistributed in 1997. In 1997, the twenty-three libraries received 2% more ILLs from the Colorado resource library. Borrowing from other Region 4 resource libraries remained the same; however, the twenty-three libraries received 4% more ILLs from other DOCLINE libraries at higher levels in the ILL hierarchy. Although this study presented no evidence to indicate whether the increases were a burden, they did not represent trivial numbers of requests. Clearly, the loss of FAMCL's and MMCL's resources affected the entire system, not just CCML libraries.
The third hypothesis was developed to determine whether CCML primary access libraries used the ILL system proportionately more than larger libraries, based on their journal collection sizes. The researchers assumed that libraries with small collections did a lot of borrowing to offset their own limited resources. The deduction from this assumption was that if they had more subscriptions, they would do less borrowing and would therefore make fewer demands on resource libraries. However, the data showed that as the library's collection size increased, its level of borrowing also increased—more subscriptions did not translate into fewer requests, so the notion that libraries with small collections did a disproportionately greater amount of borrowing to compensate was not supported.
These findings were supported by other studies that showed that purchasing more journal subscriptions did not result in a decrease in ILL borrowing. In 1984, Costello concluded that “libraries with the biggest collections both borrow and loan the most” [28]. In 1991, Miller found that “the assumption that if a library has a large collection then it will not have to borrow much through ILL does not hold true for … health sciences libraries that own fewer than 70,000 volumes.” Miller further concluded that “whatever benefits are to be derived from aggressive collection building efforts, a reduction in ILL will not be one of them” [29]. Based on the results of this study, purchasing more journal subscriptions would not significantly reduce borrowing by CCML primary access libraries.
The analysis above shows that there is little evidence to support several commonly held beliefs regarding ILL system use by primary access libraries. CCML primary access libraries do not appear to overburden libraries located at higher levels in the ILL hierarchy. Instead, they supply each other with the majority of their ILLs. The closures of two CCML primary access libraries appear to have had an impact on the entire ILL system, resulting in a greater volume of ILL activity for their state resource library and other DOCLINE libraries higher in the ILL hierarchy and highlighting the contribution made by these small libraries. Lastly, CCML primary access libraries appear to borrow and lend in amounts that are proportional to their collection size. As the foundation of the NN/LM ILL hierarchy, primary access libraries clearly play a vital role in promoting the effectiveness, efficiency, and equity of the national ILL system.
CONCLUSION
Three hypotheses were developed to test several commonly held beliefs related to ILL system use by primary access libraries. The first hypothesis explored adherence to the recommended ILL guideline to borrow as many items locally as possible before requesting ILLs from larger or more remote libraries. The literature review produced no recent articles that quantified this guideline for primary access libraries. The 1997 ILL survey data confirmed that CCML primary access libraries borrowed the majority of requested documents (61%) from each other, providing a benchmark that other primary access libraries could use to evaluate their compliance with the guideline.
The second hypothesis examined the effect of primary access library closures on ILL system activity. A subset of libraries that in 1992 exchanged ten or more items each with two libraries, which would later close, was examined to study the impact of their closures on 1997 ILL activity. The data indicated that 6% of the loans that had been supplied by the two libraries in 1992 were redistributed to the Colorado resource library and other DOCLINE libraries higher up in the ILL hierarchy in 1997. This redistribution affected the entire ILL system, resulting in increased ILL volume for libraries located higher in the ILL hierarchy and illustrating the important contribution primary access libraries make to the national ILL system.
The third hypothesis examined the relationship between collection size and ILL activity in primary access libraries. The data revealed a marginally positive correlation between items borrowed and number of subscriptions in small CCML primary access libraries and a significantly positive correlation between items loaned and number of subscriptions. These results suggested that CCML primary access libraries did not overtax the ILL system in place of purchasing more journals and that, contrary to popular belief, subscribing to more journal titles would not significantly decrease their level of borrowing from libraries higher up in the ILL hierarchy.
The authors hope that other library consortia and groups will conduct similar studies to compare with, and add to, CCML's data. In addition, several questions that are outside the scope of this study warrant further research.
What is the direct impact upon primary access libraries when their peer libraries close? The results in this study have shown that primary access library closures have an impact on libraries located at higher levels in the ILL hierarchy. Primary access libraries must also be affected when their peer libraries close, perhaps by factors such as higher direct ILL costs and greater turnaround times.
What is the effect of charging for ILL service by resource libraries and NLM on the ILL activity of primary access libraries? Are the costs associated with borrowing from larger libraries, rather than an understanding of the ILL hierarchy, responsible for the increase in primary access libraries' borrowing from each other over time?
What factors enable primary access libraries to supply their patrons with the majority of their journal article requests? Perhaps decreases in ILL borrowing by primary access libraries are due to adequate funding that enables them to meet their users' needs. In the 1970s, primary access libraries began to experience phenomenal growth, resulting in larger collections. Despite the recent negative impact of the health care economic environment on many hospital libraries, some remain well funded. Good collection-development practices may also be responsible for primary access libraries' self-sufficiency with respect to ILL. Many primary access libraries use the annual DOCLINE collection development report, Ranked List of SERLINE Titles Requested, to identify journals for addition to their collections.
How homogeneous are primary access library collections? A study of journal use in hospital libraries conducted by the Southern Chapter of the Medical Library Association in 1995 [30] revealed a surprising lack of common features among the most frequently used journals in the thirty-five hospital libraries studied. It would be interesting to determine whether CCML primary access libraries are able to fill each other's ILL requests, because, contrary to popular belief, their collections are not identical but contain many items that are unique.
This study would not have been possible without CCML's long tradition of collecting and reporting ILL statistics. The use of statistics, generated electronically by the DOCLINE and OCLC systems, coupled with the use of spreadsheets, make this data analysis possible. The authors are optimistic that statistics provided by the new Web-based DOCLINE system will be more spreadsheet-compatible and will be arranged in such a way as to be useful to library consortia, as well as individual libraries. Now that computerization has simplified collecting ILL data, more library consortia may share such information. Additional comparison and study of ILL statistics will encourage research and benefit the entire ILL system.
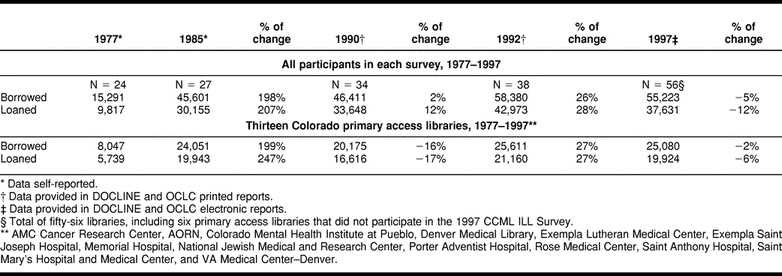
Table 3 Interlibrary loan statistics for CCML primary access libraries and for the thirteen CCML primary access libraries that participated in every CCML ILL survey
Acknowledgments
The authors gratefully acknowledge the assistance of Boyd Jacobson, Illustration/Photography Department; the staff of the Biostatistics Department, National Jewish Medical and Research Center; and Sheila Ovenhouse, Denison Memorial Library, University of Colorado Health Sciences Center. The authors would also like to thank the members of the Colorado Council of Medical Librarians for their long tradition of cooperation and for their continued ILL participation and the Medical Library Association for providing a variety of research initiatives that assist members in developing research skills.
History and cooperative projects of the Colorado Council of Medical Librarians
The Colorado Council of Medical Librarians (CCML) originated on December 4, 1956, when a group of fourteen medical librarians met at Fitzsimons Army Hospital to address “a long-felt need for closer cooperation and dissemination of professional information among the medical librarians of Denver” [1]. This handful of librarians could not have predicted the changes that their association would weather.
This new organization identified two primary objectives, to compile a union list of serials to facilitate ILLs among Denver medical libraries and to provide a forum for the exchange of ideas and discussion of library problems. The first recorded meeting of the Denver Medical Librarians occurred on June 18, 1957. The fourteen members who attended—including Isabelle T. Anderson, president of the Medical Library Association (MLA) from 1958 to 1959—began to plan a union list of serials owned by member libraries.
The organizational structure, which closely resembled the structure of CCML today, was established in 1959. As the organization continued to develop in the 1960s, individuals from health sciences libraries throughout Colorado were invited to join, and the name was changed to the Colorado Council of Medical Librarians. Today, membership has grown to include 125 individuals, representing fifty-four institutions throughout Colorado and Wyoming. Bimonthly meetings, held at member institutions on a rotating basis, have featured educational programs on librarianship or health sciences topics, followed by business meetings. Members communicate via Council Quotes, a bimonthly newsletter that began publication in 1977, an email discussion list created in 1991, and an association Website, established in 1997, that can be found at http://www.sni.net/∼ccmlnet/;.
Members' professional development is enhanced by numerous CCML-sponsored educational opportunities. The CCML Education Committee regularly contracts with MLA continuing-education instructors to provide local training to CCML members. A professional-development fund enables members to attend state and regional professional conferences and continuing-education activities. In 1980, CCML established the Isabelle T. Anderson Library Science Collection, which currently contains 197 books, audiovisual materials, and MLA course syllabi and is housed at Denison Memorial Library, University of Colorado Health Sciences Center.
CCML has a long history of promoting interlibrary cooperation among its members. The first Union List of Serials, published in 1959, consisted of typed cards representing the journal holdings of nine metropolitan Denver health sciences libraries. Methods of ILL evolved from American Library Association (ALA) forms and telephone calls; to Mile High Mail, an early electronic messaging system; to OCTANET, the precursor to DOCLINE; to DOCLINE in the late 1980s. Today, CCML's Journal Locator—Colorado and Wyoming is updated annually. The twenty-third edition, published in December
1999, included the health sciences journal holdings of fifty-three Colorado and Wyoming libraries. A Web-based union list, available to members from the association's Website, is planned.
CCML initiated what would become an ongoing series of ILL surveys in 1977 to provide a mechanism for promoting balanced ILL activity among member libraries. The first CCML ILL survey [2], conducted in 1977 as a master's thesis project by a University of Denver library science graduate student, was completed before the advent of electronic borrowing and lending systems. Although this early effort relied solely on data collected manually and reported by the participating libraries, it nonetheless established the basic methodology repeated in subsequent CCML surveys. A second survey [3], based on 1981 to 1985 CCML ILL activity, reflected the use of OCTANET. The prototype for DOCLINE, OCTANET was developed and used by the National Network of Libraries of Medicine—Midcontinental Region (NN/LM—MR), formerly Region 8 of the Regional Medical Library (RML) Program [4].
The third CCML survey [5] reported ILL activity for 1990, the first complete year of DOCLINE use by CCML libraries. It was estimated that DOCLINE, introduced in Region 8 (now Region 4) in 1989, accounted for 85% to 90% of all ILL activity among CCML member libraries in 1990. This survey was the first in which ILL data were system generated, rather than collected and reported by individual participating libraries. Based on 1992 ILL data, the fourth CCML survey [6] included DOCLINE and OCLC borrowing and lending statistics, representing an estimated 95% of all CCML ILL activity for that year.
The fifth survey, described in this paper, was based on the 1997 DOCLINE and OCLC ILL data of fifty-four CCML member libraries, including fifty primary access libraries, two state resource libraries, and two general academic libraries in Colorado and Wyoming. Thirteen Colorado primary access libraries have participated in all five CCML surveys. Table 3 provides 1977 to 1997 summary ILL data for all participating CCML primary access libraries and separate summary data for the thirteen libraries that participated in every survey.
The primary objective of the CCML ILL survey is to improve services by promoting efficient, equitable ILL resource sharing among CCML members. Each survey has resulted in specific recommendations for improving the effectiveness, efficiency, and equity of ILL services, including, for example, a recommended CCML DOCLINE routing table.
During the 1980s, nine CCML primary access libraries and Denison Memorial Library at the University of Colorado Health Sciences Center formed MEDCONNECT, a cooperative online catalog using the Innovative Interfaces, Inc. (III), integrated library system. In 1999, CCML established an ILL resources Web page that can be found at http://www.sni.net/∼ccmlnet/illresources.html.
REFERENCES
1. Barrett M, Anderson IT. Letter to Col. HW Doan, Deputy Commander, Fitzsimons Army Hospital [personal communication]. Denver, CO, 1957 Jan 8.
2. O'Neill SA. An interlibrary loan survey of Denver area medical libraries [thesis]. Denver, CO: University of Denver, 1977.
3. Colorado Council of Medical Librarians Interlibrary Loan Task Force. Summary and final results of the 1985 ILL survey. Denver, CO, 1986 May.
4. Gadzikowski C. Octanet—an electronic library network; the first four years: summary and evaluation. Inf Technol & Libr 1987 Jun;6(2):138–43.
5. Dudden RF, Katsh S. Interlibrary loan survey interpretation. Council Quotes: Bulletin of the Colorado Council of Medical Librarians 1991 Jul;14(4):2–5, 12–5.
6. Dudden RF, Urich C. Colorado Council of Medical Librarians 1992 interlibrary loan survey. Council Quotes: Bulletin of the Colorado Council of Medical Librarians 1993 Sep;16(5 suppl):13–24.
REFERENCES
- Arnold GN, Fishel MR. Interlibrary loan and document delivery. In: Lipscomb CE, ed. Information access and delivery in health sciences libraries. Lanham, MD: Medical Library Association and Scarecrow Press, 1996:103–4. (Current practice in health sciences librarianship, v. 3). [Google Scholar]
- U.S. National Library of Medicine. Fact sheet National Network of Libraries of Medicine [Web document]. Bethesda, MD: National Network of Libraries of Medicine. [rev. 21 Sep 1999; cited 12 May 2000]. <http://www.nlm.nih.gov/pubs/factsheets/nnlm.html. [Google Scholar]
- Colorado Council of Medical Librarians Interlibrary Loan Survey Task Force. 1997 interlibrary loan survey report Colorado Council of Medical Librarians (CCML). Council Quotes. 1999 Jan–Feb. 22(1 Suppl 1):1–18. [Google Scholar]
- Waldhart TJ. Patterns of interlibrary loan in the U.S.: a review of research. Libr Inf Sci Res. 1985 Jul–Sep. 7(3):209–29. [Google Scholar]
- Prabha CG.. Estimating interlibrary loan volume in 1993 academic, public, special, and federal libraries. OCLC Syst Serv. 1995;10(4):36–9. [Google Scholar]
- Kurth WH. Survey of the interlibrary loan operation of the National Library of Medicine. Washington, DC: Public Health Service, National Institutes of Health, 1962. [Google Scholar]
- Lacroix EM, Dutcher GA. A comparison of interlibrary loan requests received by the National Library of Medicine: 1959 and 1984. Bull Med Libr Assoc. 1987 Jan. 75(1):7–13. [PMC free article] [PubMed] [Google Scholar]
- Kingma BR. The economics of access versus ownership: the costs and benefits of access to scholarly articles via interlibrary loan and journal subscriptions. Binghamton, NY: Haworth Press, 1996. [Google Scholar]
- Budd JM.. Interlibrary loan activity among ARL members, 1977–78 to 1986–87. J Interlibrary Loan Inf Supply. 1990;1(1):13–23. [Google Scholar]
- Costello J, Duffy C.. Academic interlibrary loan in New York state: a statistical analysis. J Interlibrary Loan Inf Supply. 1990;1(2):41–3. [Google Scholar]
- Waldhart TJ. The growth of interlibrary loan among ARL university libraries. J Acad Libr. 1984 Sep. 10(4):204–8. [Google Scholar]
- Irving S, Senglup K.. Empire express: case study of a New York state resource sharing model. J Interlibrary Loan Doc Deliv Inf Supply. 1997;7(4):21–35. [Google Scholar]
- Jackson ME. Measuring the performance of interlibrary loan operations in North American research and college libraries. Washington, DC: Association of Research Libraries, 1998. [Google Scholar]
- Morton DJ. Analysis of interlibrary requests by hospital libraries for photocopied journal articles. Bull Med Libr Assoc. 1977 Oct. 65(4):425–32. [PMC free article] [PubMed] [Google Scholar]
- Lacroix EM. Interlibrary loan in U.S. health sciences libraries: journal article use. Bull Med Libr Assoc. 1994 Oct. 82(4):363–8. [PMC free article] [PubMed] [Google Scholar]
- Clevesy SR, Inglis IE. Predicting the impact of the new copyright law on the interlibrary loan transactions of a hospital library consortium. Bull Med Libr Assoc. 1978 Jul. 66(3):339–42. [PMC free article] [PubMed] [Google Scholar]
- Monroe J. Hospital library cooperation in Kentucky, Ohio & Michigan. Hosp Libr. 1976 Dec 15. 1(12):5–7. [PubMed] [Google Scholar]
- Mundt JL. Hospital libraries' consortium blunts impact of budget cuts. Hospitals. 1978 Jun 1. 52(11):75–6,78. [PubMed] [Google Scholar]
- Bailey AS, Tibbetts P. The Twin Cities Biomedical Consortium. Bull Med Libr Assoc. 1975 Jul. 63(3):252–8. [PMC free article] [PubMed] [Google Scholar]
- Smith JMB. Metropolitan Detroit's network: an analysis of interlibrary loan in metropolitan Detroit. Bull Med Libr Assoc. 1968 Jul. 56(3):281–4. [PMC free article] [PubMed] [Google Scholar]
- Felber S, Hill TW, and Barry M. The SEND (SouthEastern Network on DOCLINE) project: a reciprocal document delivery network. Bull Med Libr Assoc. 1999 Apr. 87(2):214–6. [PMC free article] [PubMed] [Google Scholar]
- U.S. National Library of Medicine. Using NLM's DOCUSER®. [Web document]. Bethesda, MD: National Network of Libraries of Medicine. [rev. 30 Dec 1998; cited 17 Sep 1999]. <http://www.nnlm.nlm.nih.gov/nnlm/docdel/docuser.html>. [Google Scholar]
- Boucher V. Interlibrary loan practices handbook. 2d ed. Chicago, IL: American Library Association, 1996:37. [Google Scholar]
- American Library Association. National Interlibrary Loan Code for the United States 1993. [Web document]. Chicago, IL: RASD MOPSS Interlibrary Loan Committee. [rev. 4 Jun 1999; cited 17 Sep 1999]. <http://www.ala.org/rusa/stnd_lnc.html>. [Google Scholar]
- Arnold GN, Fishel MR. Interlibrary loan and document delivery. In: Lipscomb CE, ed. Information access and delivery in health sciences libraries. Lanham, MD: Medical Library Association and Scarecrow Press, 1996:103–4. (Current practice in health sciences librarianship, v. 3). [Google Scholar]
- Smith JMB. Metropolitan Detroit's network: an analysis of interlibrary loan in metropolitan Detroit. Bull Med Libr Assoc. 1968 Jul. 56(3). , 281–4. [PMC free article] [PubMed] [Google Scholar]
- Cruzat GS. Metropolitan Detroit's Network: Detroit medical library group: five year progress report. Bull Med Libr Assoc. 1968 Jul. 56(3):285–91. [PMC free article] [PubMed] [Google Scholar]
- Costello , Costello J, and Duffy C. Academic interlibrary loan in New York state: a statistical analysis. J Interlibrary Loan Inf Supply. 1990 1(2). , 43. [Google Scholar]
- Miller J. Primary clientele as a predictor of interlibrary borrowing: a study of academic health sciences libraries. Bull Med Libr Assoc. 1997 Jan. 85(1):11–5. [PMC free article] [PubMed] [Google Scholar]
- Dee CR, Rankin JA, and Burns CA. Using scientific evidence to improve hospital library services: Southern Chapter/Medical Library Association journal usage study. Bull Med Libr Assoc. 1998 Jul. 86(3):301–6. [PMC free article] [PubMed] [Google Scholar]