

Abstract
Background and aims
It is critical to have a proper knowledge of the normal anatomy of the pulp and its variations for the success of endodontic treatment. The aim of this study was to determine the canal configuration and the prevalence of C-shaped canals in mandibular first and second premolars in a North-Western Iranian population.
Materials and methods
A total of 163 extracted mandibular first and 103 mandibular second premolars were injected with India ink and demineralized . They were made clear and transparent with methyl salicylate and the anatomy of their canal(s) was studied.
Results
The results showed that 98% of mandibular first premolars had one root, 2% had two roots, 70.6% had one canal, 27.8% had two canals, 1.2% had three canals and the prevalence of C-shaped canals was 2.4%. All mandibular second premolars had one root, 80.5% had one canal, 17.5% had two canals and the prevalence of C-shaped canals was 2%.
Conclusion
It is important that clinicians, before treatment of mandibular first and second premolars, pay complete attention to radiographs, have a true concept of the number of root(s) and canal(s), and prepare a correct access cavitiy.
Keywords: C-shaped canal, canal configuration, clearing, mandibular first premolar, mandibular second premolar
Introduction
The objective of endodontic therapy is the restoration of the treated tooth to its proper form and function in the masticatory apparatus in a healthy state.1 Knowledge of pulp anatomy is essential to endodontic treatment success and lack of sound knowledge of the pulp anatomy can contribute to treatment failure. Knowledge of the normal or unusual configuration of the pulp and possible variations is highly critical for success in endodontics. It is absolutely essential for an operator to form a mental picture of the pulp in cross section and from the coronal aspect to the apical foramen. Each canal contains irregular and hidden regions that should be taken into account during endodontic treatment. Instruments must access these hidden regions and clean and shape them as maximally as possible to avoid or minimize treatment failure.2
Increasing emphasis is placing on retaining pulpally involved teeth by dentists since no replacement can function as efficiently as natural teeth. In recent years endodontics has greatly enhanced its role in modern dentistry regarding the preservation of natural teeth. Endodontic treatment is highly successful (90%)3 in retaining natural teeth if it is combined with efficient restoration of the involved tooth.
As a group, the mandibular premolars are very difficult to treat; they have a high flare-up and failure rate. A possible explanation may be the extreme variations in root canal morphology in these teeth. The root canal system of the mandibular first premolar is wider buccolingually than mesiodistally. Two pulp horns are present: a large, pointed buccal horn and a small, rounded lingual horn. At the cervical line the root and canal are oval; this shape tends to become round as the canal approaches the middle of the root. If two canals are present; they tend to be round from the pulp chamber to their foramen. In another anatomic variation, a single, broad root canal may bifurcate into two separate root canals. Direct access to the buccal canal is usually possible, whereas the lingual canal may be very difficult to find. The lingual canal tends to diverge from the main canal at a sharp angle. In addition, the lingual inclination of the crown tends to direct files buccally, making location of a lingual canal orifice more difficult. To counter this situation, the clinician may need to extend the lingual wall of the access cavity farther lingually; this makes the lingual canal easier to locate.
The mandibular first premolar sometimes may have three roots and three canals.3 One study reported a C-shaped canal anatomy in this tooth.4 The oval external outline form of the mandibular first premolar typically is wider mesiodistally than its maxillary counterpart, making it more oval and less slot-shaped. Because of the lingual inclination of the crown, buccal extension can nearly approach the tip of the buccal cusp to achieve straight-line access. Lingual extension barely invades the poorly developed lingual cusp incline. The access preparation is mesiodistally centered between the cusp tips and the preparation must often be modified to allow access to the complex root canal anatomy frequently seen in the apical half of the tooth root.
The mandibular second premolar is similar to the first premolar, with the following differences: the lingual pulp horn usually is larger; the root and root canal are more often oval than round; the pulp chamber is wider buccolingually; and the separation of the pulp chamber and root canal is normally distinguishable compared with the more regular taper in the first premolar. The canal morphology of the mandibular second premolar is similar to that of the first premolar with its many variations: two, three, and four canals and a lingually tipped crown. Fortunately, these variations are found less often in the second premolar.
The access cavity form for the mandibular second premolar varies in at least two ways in its external anatomy. First, because the crown typically has a smaller lingual inclination less extension up the buccal cusp incline is required to achieve straight-line access. Second, the lingual half of the tooth is more fully developed; therefore the lingual access extension is typically halfway up the lingual cusp incline. The mandibular second premolar can have two lingual cusps, sometimes of equal size. When this occurs, the access preparation is centered mesiodistally on a line connecting the buccal cusp and the lingual groove between the lingual cusp tips. When the mesiolingual cusp is larger than the distolingual cusp, the lingual extension of the oval outline form is just distal to the tip of the mesiolingual cusp.3
The purpose of this study was to investigate the canal configuration and the prevalence of C-shaped canals in mandibular first and second premolars in an Iranian population in the North-West of Iran.
Materials and Methods
A total of 163 extracted mandibular first and 103 mandibular second premolars were collected from Tabriz Faculty of Dentistry, dental clinics and private offices of Tabriz, a city in the North-West of Iran. The identification of these teeth as mandibular second premolars was confirmed by two independent observers using accepted criteria of Woelfel (1990).5 Only those teeth on which both investigators agreed were used in this study. The teeth were collected during one year and stored in 10% formalin. Since a large number of these teeth had been extracted because of periodontal problems, they were intact or had small caries or fillings in coronal portions. The selected teeth were cleaned of any adherent soft tissues, bone fragments and calculus by scaling and polishing. An endodontic access cavity was then prepared in each tooth with diamond fissure burs (DG16-Germany).The floors of the pulp chambers were examined with a DG16 endodontic explorer (Hu Freiday, Chicago, IL, USA) to identify the root canal orifices. After locating the orifices, the teeth were placed in 5.25% sodium hypochlorite solution (Golrang, Tehran, Iran) for 48h to dissolve debris and pulp remnants. All the specimens were then thoroughly rinsed in running water for 4h to clean the root canals of any debris. Once washed, India ink was injected into the root canals and the teeth were demineralized for 3 days in 5% nitric acid at room temperature (20ºC). The nitric acid solution was changed every day. After demineralization, the teeth were rinsed in running water for 4h. The dehydration process consisted of a series of ethyl alcohol (Ararat, Tehran, Iran) rinses starting with 80% overnight, followed by 90% for 1h and then 100% ethyl alcohol rinses for 1h. The dehydrated teeth were placed in methyl salicylate (B.P.63 Poland) for 2h to make them clear and transparent. The cleared teeth were examined under a magnifying-glass (Lumagny, No.7540 Hong Kong) at ×5 magnification. The root canal systems were classified according to the classification of Vertucci (1984).6
Results
Out of 163 mandibular first premolars, 160 (98%) teeth had one root and 3 (2%) had two roots. The canal configurations of mandibular first premolars according to Vertucci’s classification6 (Table 1) were as follow: type I=113 (70.6%), type II=3 (1.9%), type III=6 (3.8%), type IV=6 (3.8%), type V=27 (16.9%) (Figure 1), type VI=2 (1.2%), type VII=1 (0.6%) and two teeth had unusual form (1.2%) (Figure 2, Table 2), three of the mandibular first premolars had two roots and two canals (one canal in each root) (Table 1), 4 (2.4%) teeth had C-shaped configuration; type I=3 (1.8%) and type IV=1 (0.6%) (Figure 3).
Table 1. The number and percentage of the roots in the mandibular first premolars.
| One-rooted | Two-rooted | Three-rooted | Total | |
| Number | 160 | 3 | 0 | 163 |
| Percent | 98% | 2% | 0 | 100 |
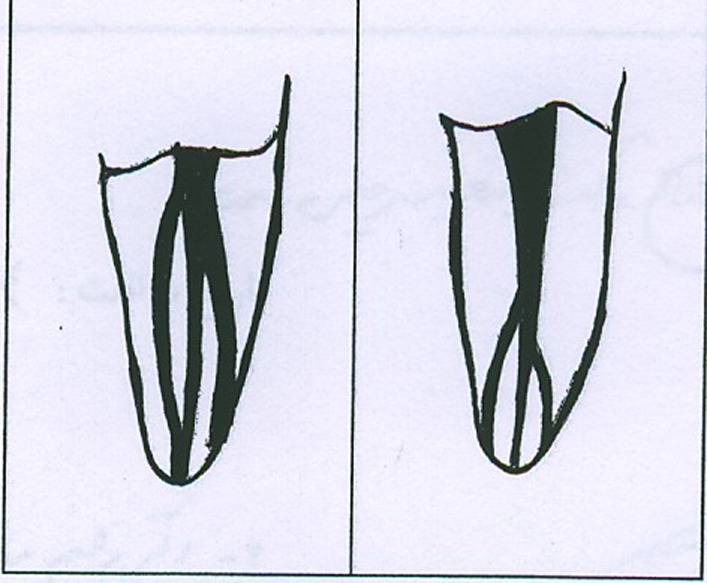
Figure 1.

Type V canal configuration in mandibular first premolars.
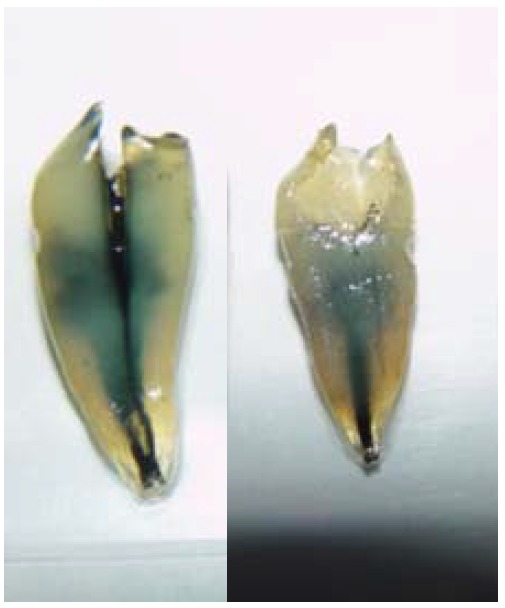
Figure 2.
Unusual canal configuration in mandibular first premolars.
Table 2. Canal configuration in one-rooted mandibular first premolars.
| Canals | Canal configurations of the roots | Total | ||||||||
| I | II | III | IV | V | VI | VII | VIII | Unusual | ||
| Number | 113 | 3 | 6 | 6 | 27 | 2 | 1 | 0 | 2 | 160 |
| Percent | 70.6 | 1.9 | 3.8 | 3.8 | 16.9 | 1.2 | 0.6 | 0 | 1.2 | 100 |
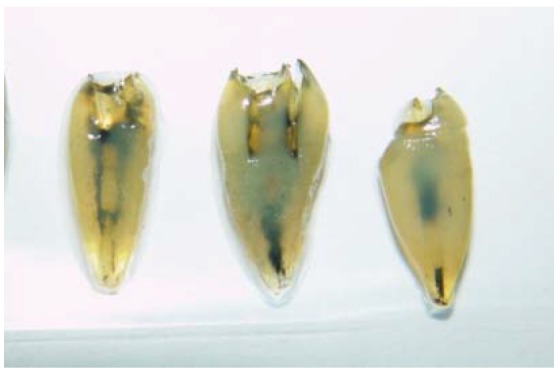
Figure 3.
C-shaped canals in mandibular first premolars.
All 103 mandibular second premolars were one rooted and the canal configurations of mandibular second premolars according to Vertucci’s classification6 were as follow: type I=77 (76.3%), type II=8 (7.9%), type III=10 (9.9%), type IV=6 (5.9%) (Table 3) and two teeth had C-shaped configuration (2%) type I=2 (Figure 4).
Table 3. Canal configuration in one-rooted mandibular second premolars.
| Canals | Canal configurations of the roots | Total | |||||||
| I | II | III | IV | V | VI | VII | VIII | ||
| Number | 77 | 8 | 10 | 6 | 0 | 0 | 0 | 0 | 101 |
| Percent | 76.3 | 7.9 | 9.9 | 5.9 | 0 | 0 | 0 | 0 | 100 |
Figure 4.
C-shaped canals in mandibular second premolars.
Discussion
There are different methods to study the morphology of human permanent teeth. These include the use of radiography,7 placing files in the canals to determine canal configuration, cutting the teeth in different levels,8 polyester resin cast replicas of the pulp space,9 and clearing and injection of dye.10 The clearing technique is valuable for studying the root canal anatomy with these advantages: (1) it produces a 3-D view of the pulp cavity,11 and (2) instruments are not needed to enter the pulp system.11 Therefore, this technique helps to maintain the original form of the pulp system.11 Because of the accuracy of clearing technique, this method was used in the present study.
Our study revealed that 98% of mandibular first premolars had one root and only 2% had two roots; 70.6% had one canal similar to the results of the previous studies (69.3%-86%).7 , 12 , 13 , 14 Mandibular first premolars had two canals in 27.8% of cases which is also similar to the results of the previous studies (14%-25.5%).7 , 12 , 13 , 14 The incidence of three canals in the mandibular first premolars was 1.2% which is similar to the results of the previous studies (0.4%-0.9%).7 , 12 , 13 , 14 In general, the results of this study is similar to the results of a recent literature review showing that 97.9% of the mandibular first premolars had a single root, 1.8% had two, 0.2% had three and less than 0.1% had four roots and one canal was present in 75.8% and two or more canal systems were found in 24.2% of the teeth studied.15
In this study the mandibular first premolars had one canal in 76.2%, two canals in 23.1%, and three canals in 0.6% of specimens in the apex that is similar to the Vertucci’s study (74%, 25.5%, and 0.5%, respectively).14 One rooted mandibular first premolars had one canal and one apical foramen in 70.6%, two canals and one apical foramen in 5.6%, two canals and two foramen in 22% and had three canals in 1.2% of cases which is similar to Ingle’s results (one canal and one apical foramen=73.5%, two canals and one apical foramen=6.5%, two canals and two apical foramen=19.5% and three canals=0.5%).16
The interesting finding of this study was the noticeable prevalence of C-shaped canals (2.4%) in the mandibular first premolars. The prevalence of C-shaped canals in the mandibular first premolars had only been reported in three previous studies (Baisden et al, 19924[14%]; Sikri and Sikri, 199417 [10%]; Lu et al, 200618 [18%]). The differences between the results obtained in various studies regarding the anatomy of mandibular first premolars and the prevalence of C-shaped canals may arise from racial differences and methods of studying.
All of the mandibular second premolars in the present study were one rooted and a large number of them had one canal (85.5%) that is similar to Ingel’s results.16 However, 17.8% of these teeth had two canals which is different from Vertucci’s study (2.5%).6 Such differences may result from racial differences and methods of studying.
According to the results of this study, the mandibular second premolars had one canal in the apex in 82.5% of cases and two canals in the apex in 15.5% of cases, which is a similar finding to Ingel’s16 results (one canal in the apex=87% and two canals in the apex=11.5%). Mandibular second premolars had one canal and one apical foramen in 74.7% and had two canals and two foramens in 9.7% of cases. This finding is slightly different from Ingel’s16 results (one canal and one apical foramen=85.5% and two canals with two apical foramen foramens=11.5%).
Mandibular second premolars had two canals with one apical foramen in 7.8% of the cases that is different from Ingel’s results (two canals with one apical foramen=1.5%) and may also result from racial differences and methods of studying.16
Other interesting finding of this study was the 2% prevalence of C-shaped canals in the mandibular second premolars which was not reported in previous studies.
The results of this study revealed that mandibular first and second premolars had many variations in canal(s) morphology. It is, therefore, recommended that clinicians consider a thorough assessment of radiographs before treatment of mandibular premolars and have a true concept of the number of root(s) and canal(s). Special attention must be given to the preparation of a correct access cavity that is the key to finding all orifices and a successful treatment. The concept of mandibular premolars with one canal should not be considered as a rule. The future studies may reveal interesting facts about the canal configuration and the prevalence of C-shaped canals in mandibular first and second premolars in different parts of the world.
References
- 1.Weine FS. Endodontic Therapy. 5th ed. St. Louis: CV Mosby; 1996. 1,2,230-304 [Google Scholar]
- 2.Walton RE, Torabinejad M. Principal and Practice of Endodontics. 3rd ed. Philadelphia: Saunders; 2002. 167 [Google Scholar]
- 3.Cohen S, Burns RC. Pathways of the Pulp. 8th ed. St Louis: CV Mosby; 2006. 216-19 [Google Scholar]
- 4.Baisden MK, Kulilid JC, Weller RN. Root canal configuration of the mandibular first premolar. J Endod. 1992;18:505–8. doi: 10.1016/S0099-2399(06)81352-X. [DOI] [PubMed] [Google Scholar]
- 5.Woelfel JB, Scheid RC. Dental Anatomy. 5th ed. Baltimore: Williams & Willkins; 1997. 191-212 [Google Scholar]
- 6.Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol. 1984;58:589–99. doi: 10.1016/0030-4220(84)90085-9. [DOI] [PubMed] [Google Scholar]
- 7.Pineda F, Kutller Y. Mesiodistal and buccolingual roengenographic investigation of 7275 root canals. Oral Surg Med Oral Pathol. 1972;33:101–10. doi: 10.1016/0030-4220(72)90214-9. [DOI] [PubMed] [Google Scholar]
- 8.Weine FS, Pasiewics RA, Rice RT. Canal configuration of the mandibular second molar using a clinically oriented in vitro method. J Endod. 1988;14:207. doi: 10.1016/S0099-2399(88)80171-7. [DOI] [PubMed] [Google Scholar]
- 9.Skidmore AE, Bjorndal AM. Root canal morphology of the human mandibular first molar. Oral Surg Med Oral Pathol. 1971;32:119–24. doi: 10.1016/0030-4220(71)90304-5. [DOI] [PubMed] [Google Scholar]
- 10.Weine FS, Healing HJ, Gerstein H, Evanson L. Canal configuration in the mesiobuccal root of the maxillary first molar and its endodontic significance. Oral Surg Oral Med Oral Pathol. 1969;28:419–25. doi: 10.1016/0030-4220(69)90237-0. [DOI] [PubMed] [Google Scholar]
- 11.Barker BCW, Lockett BC, Parsons KC. The demonstrations of root canal anatomy. Aust Dent J. 1969;14:37–41. doi: 10.1111/j.1834-7819.1969.tb03330.x. [DOI] [PubMed] [Google Scholar]
- 12.Green D. Double canals in single roots. Oral Surg Oral Med Oral Pathol. 1973;35:689–96. doi: 10.1016/0030-4220(73)90037-6. [DOI] [PubMed] [Google Scholar]
- 13.Zillich R, Dawson J. Root canal morphology of mandibular first and second premolars. Oral Surg Oral Med Oral Pathol. 1973;36:738–44. doi: 10.1016/0030-4220(73)90147-3. [DOI] [PubMed] [Google Scholar]
- 14.Vertucci FS. Root canal morphology of mandibular premolars. J Am Dent Assoc. 1978;97:47–50. doi: 10.14219/jada.archive.1978.0443. [DOI] [PubMed] [Google Scholar]
- 15.Cleghorn BM, Christie WH, Dong CCS. The root and root canal morphology of the human mandibular first premolar: a literature review. J Endod. 2007;33:509–16. doi: 10.1016/j.joen.2006.12.004. [DOI] [PubMed] [Google Scholar]
- 16.Ingle JI, Bakland Lk. Endodontics. 5th ed. Hamilton: BC Decker Inc; 2002. 449-51 [Google Scholar]
- 17.Sikri VK, Sikiri P. Mandibular premolars: aberationsin pulp space morphology. Indian J Dent Res. 1994;5:9–14. [PubMed] [Google Scholar]
- 18.Lu TY, Yang SF. Complicated root canal morphology of mandibular first premolar in a Chinese population using the cross section method. J Endod. 2006;32:932–6. doi: 10.1016/j.joen.2006.04.008. [DOI] [PubMed] [Google Scholar]