

Abstract
Background and aims
Dental caries still remains a major problem in the field of oral and dental health and its prevention is more important than its treatment. Fluoride plays a significant role in prevention of caries, and improving oral and dental health. One of the common ways of fluoride use is the use of a fluoride-containing mouthwash, the most important of which in use is 0.2% sodium fluoride mouthwash. School-based fluoride mouthwash programs have been used for delivering oral and dental health to children in recent years. The aim of the present study was to assess the efficiency of 0.2% sodium fluoride mouthwash in prevention of dental caries according to DMFT index.
Materials and methods
The study included a case and a control group. For each group, 100 students were selected randomly from elementary schools of Tabriz, Iran. Case group had been participating in school-based fluoride mouthwash program for three years, while control group did not benefit from the program. The two groups were assessed by means of intra-oral examination. Data was recorded using DMFT index.
Results
Following the use of 0.2% sodium fluoride mouthwash, mean DMFT index in case group decreased as much as 51.5% compared to that of control group. The mean values of decrease for the decayed, missing and filled indices were 45%, 44% and 59%, respectively. The decrease in DMFT value of the case group compared to that of control group was statistically significant (p<0.001). A statistically significant decrease was seen in the decayed and filled indices of case group (p=0.042 and p=0.016, respectively), however the missing index did not show any statistically significant difference between the two groups (p=0.361).
Conclusion
According to this study results, the weekly use of 0.2% sodium fluoride mouthwash program has been successful in elementary schools of Tabriz. Such program can play an important role in the improvement of oral and dental health among children of school age.
Keywords: Dental caries, DMFT index, fluoride mouthwash
Introduction
Fluoride has played a significant role in improvement of oral and dental health during the past 50 years. Our knowledge of dental caries and its mechanism, and the role of fluoride in this process have evolved during recent years.
Early studies revealed that fluoridation of drinking water to a level of 1 ppm results in maximum decrease in the incidence of dental caries. Since then, adding fluoride to drinking water was brought in for discussion in scientific assemblies of dentists and a number of measures were taken in this field. Currently, it is recommended that each individual should receive 0.05 mg/kg/day fluoride (0.03 to 0.07 mentioned in different studies) to obtain the maximum reduction in dental caries while minimizing the risk of severe fluorosis, which can cause changes in the color of enamel and/or enamel pitting.
Fluoride intake occurs through consumption of drinking water, fluoridated salt, fluoridated products including various drinks, foods, supplements, and powdered milk and the use of fluoridated toothpastes, mouthwashes, and topical fluoride. Foods or drinks prepared using fluoridated drinking water will also contain some fluoride. Since fluorosis can only occur in children under 6 years of age, the use of fluoride should be limited in this group of children. In fact, the use of fluoride mouthwash is not recommended in children younger than 6 years old with the exception of cases where child is at a high risk for caries.,2
According to previous reports, the use of fluoride mouthwash seems to be effective in both large group and individual studies. 0.05% and 0.2% sodium fluoride mouthwashes are currently available. 0.05% sodium fluoride mouthwash is a weak solution which should be used daily, whereas 0.2% sodium fluoride mouthwash is stronger and should be used once a week. Twenty to forty percent reduction in caries is expected with this therapeutic method. In a study in Sweden, researchers observed that fluoridated brush is more effective on maxillary teeth. In addition, other studies have reported that the effect of fluoride mouthwash is more pronounced on proximal surfaces. The use of fluoride mouthwash is recommended for children receiving orthodontics or radiotherapy.1 - 4
Another study in Sweden reported that the use of fluoride mouthwash as well as regular use of fluoridated toothpaste and brush has a significant effect in decreasing dental caries.5 In one study in South Africa, the use of 0.2% sodium fluoride for a period of 6 years resulted in reduction of dental caries incidence according to DMFT index.1 In a study involving 750 children in the USA, the weekly use of 0.2% sodium fluoride mouthwash resulted in 52.2% decrease of in the mean DMFT score.6
Previous studies have demonstrated that socio-economic status of families influence the amount of caries reduction following the use of fluoride: The amount of reduction in DMFT scores is generally higher in groups with low socio-economic status.7 - 9
Although the usefulness of sodium fluoride mouthwash seems to be established, we decided to evaluate the success rate of Iranian Health Ministry’s policy concerning free distribution of 0.2% sodium fluoride mouthwash among public schools considering the sociocultural aspects of the selected population in northwestern Iran.
Materials and Methods
In this case-control study, forth grade students of elementary schools in North-Western city of Tabriz, Iran, were taken into consideration. Four schools were selected randomly. Sodium fluoride mouthwash program had been in progress for at least three years in two of the four schools (case group). The other two schools had not participated in the program (control group). Both groups consisted of a girls’ and a boys’ school. Fifty students were selected randomly from each school. The total number of samples was 200 which included 100 students in the case group and 100 students in the control group.
Data Collecting Methods
A questionnaire was given to the students. The students’ age, gender and frequency of fluoride mouthwash use were recorded. The status of students’ oral health was evaluated by means of recording the frequency of brushing and using dental floss. The answers were recorded as follows: No teeth brushing or flossing, occasionally (once in a while), once daily, and more than once daily.
Determining the economic status of a family is a controversial subject, as its assessment requires evaluating various data. Since all possible data cannot usually be evaluated appropriately, the economic status of family was assessed by recording the monthly income, frequency of trips in a year, and frequency of occasions on which family members eat out in a month. Monthly income was recorded based on these six groups: lower than 1 million Rials, 1-1.99 million Rials, 20-2.99 million Rials, 3-3.99 million Rials, 4-4.99 million Rials and 5 million Rials or more. Frequency of trips in a year and frequency of occasions on which family members eat out in a month were recorded as follows: never, rarely, occasionally, and often.
Questionnaire was completed by the student and his/her parents’ assistance. Upon the completion of the questionnaire, oral and dental examination was carried out by a dentist using a dental mirror, an explorer, and a tongue depressor. The examinations were performed on a chair in natural daylight setting. DMFT Data was recorded separately for decayed, missing and filled indices.
To eliminate the confounding effect of some variables on proper assessment of data, the effect of these variables were evaluated and the samples were normalized before performing the main analysis of data, if necessary. These variables included age, gender, economic status of the family, and oral and dental health status (the use of brush and dental floss).
Statistical Methods
Data was analyzed using SPSS 14.0 computer software. With regard to the variable under assessment, chi-square, independent samples t-test and ANOVA tests were used.
Ethical Regards
Subjects and their parents had the authority to complete the questionnaire. There was no information on the questionnaire that would lead to the identification of individuals. The completed questionnaires were not given to school personnel and in case of their request, only the results of the study were submitted to them. There was no interference in the study and no charge was imposed to the student or his/her family.
Results
Oral and dental health condition was defined as the frequency of brushing and using dental floss. The mean frequency of brushing in the case group was once daily (0.5% never, 16.5% once in a while, 59% once daily and 24% more than once daily); the condition of using dental floss in case group was as follows: 41% never, 35.5% once in a while, 14% once daily and 9.5% more than once daily. Most of the students did not use dental floss. There was no significant difference between the two groups with regard to brushing and using dental floss (p=0.319 and p=0.143, respectively).
None of three variables related to the socio-economic status showed a significant difference between case and control groups (for monthly income, frequency of trips in a year, and frequency of occasions on which family members eat out in a month, p=0.101, p=0.153, p=0.271, respectively). Therefore, these confounding variables could not have a pronounced effect on the results.
The mean DMFT value for the control group was 1.32±0.11. The mean values for decayed, missing and filled indices in the control group were 0.60±0.08, 0.09±0.02 and 0.63±0.09, respectively. The mean DMFT index for the case group was 0.64±0.1. The mean values for decayed, missing and filled indices of case group were 0.33±0.06, 0.05±0.02 and 0.26±0.08, respectively. The comparison of case and control groups based on DMFT is shown in figure 1.
Figure 1.
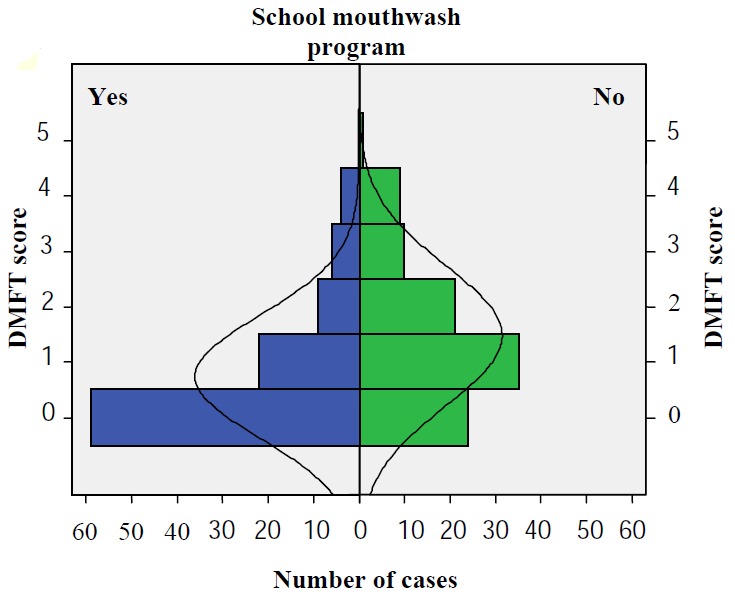
DMFT index in case and control groups.
The difference of DMFT index between case and control groups was statistically significant (p<0.001). Significant statistical difference was observed between control and case groups based on decayed and filled indices (p=0.042 and p=0.016, respectively), but there was not any significant difference with regard to missing index between control and case groups (p=0.361).
The mean DMFT value of the case group decreased 0.68 scores (51.5%) compared to the control group. The decrease in the values of decayed, missing and filled indices were 0.27 (45%), 0.04 (44%), and 0.37 (59%), respectively. The decrease in DMFT value in the case group was statistically significant after introducing oral and dental health program (p<0.001). There was also a significant decrease in decayed and filled indices (p=0.042 and p=0.016, respectively), but the decrease in missing index of case group was not statistically significant (p=0.361).
The number of 10 year-old elementary school children that were caries free increased from 53% in the control group to 75% in the case group. In addition, the number of children that did not need dental restorations increased from 67% in control group to 82% in case group.
Discussion
According to the results, the use of 0.2% sodium fluoride mouthwash program in elementary schools has significantly decreased dental caries after three years. These results are in accordance with previous studies in other parts of the world.9 - 26
There are, however, other studies that do not indicate a significant reduction in dental caries following administration of 0.2% sodium fluoride mouthwash program in schools. The studies of Poulsen27, Disney28, and Chikte29 are among them.
In the present study, the decrease of DMFT index in the case group in comparison to the control group was 51.5%. A review article by Twetman reported nearly 30% reduction in caries.25 A decrease as much as 54.1% at Ripa study following a 6-year program11, 76.1% at Yoshihara study16, 14.2% at Lovwa study following three-year program of using sodium fluoride mouthwash20, 86% at Kobayashi study following a long-term program21, and 15% at Chikte study following a three-year program of using sodium fluoride mouthwash29 have been reported.
In this study the number of caries-free children increased to 22% after a three-year program of using fluoride mouthwash in 10-year-old children. The increase in caries-free children in other reports varies from 23% following a six-year program of using fluoride mouthwash in 12-year-old children11 to 60% following a long-term program of using fluoride mouthwash.21
It should be noted that the present study was carried out mostly on 10-year-old elementary school children in whom the incisors and the first molars were generally the only erupted permanent teeth. Many previous studies have been carried out among 12-year-old children with a complete permanent dentition.11 , 25 , 27 Although fewer number of permanent teeth leads to a lower DMFT value, the obtained results are still valuable since the mean age of case and control subjects in the present study was the same. However, the difference between studied age groups should be considered when comparing the results of this study with that of the previous studies.
In addition, there are other differences between previous studies and the present study which include differences in the level of fluoride in drinking water, socio-economic status of subjects, the condition of individuals’ dental caries prior to initiation of the fluoride program and the condition of the control group.
The level of fluoride in drinking water in Tabriz is 0.3 ppm which is regarded a low level. In many of the previous studies the level of fluoride in drinking water was low as well.11 , 13 Studies indicated that inhabitants of regions with low level of fluoride in drinking water take the most advantage from such programs.25 This must be taken into consideration in evaluating the effect of the fluoride mouthwash program. Additional methods of fluoride intake are also considered to be a contributing factor.
The caries status of individuals before introducing the fluoride program is also important, because people with a high level of caries take the most advantage and exhibit maximum reduction in caries.28
In some of the previous studies cleaning of the teeth with distilled water was performed weekly in control group so that the reduction of caries following the use of fluoride mouthwash could be more connected to the effect of fluoride ion instead of merely washing effect of the mouthwash.10 , 27 Like most of the previous studies,9 , 11 , 14 , 18 , 30 however, we did not use distilled water as a mouthwash in the control group.
Conclusion
According to the obtained results, it can be concluded that the weekly use of 0.2% sodium fluoride mouthwash in elementary schools of Tabriz has been successful. The reduction in the level of caries due to the fluoride mouthwash program was significant and in accordance with the results of other studies in low hygiene regions. This program can play an important role in the improvement of oral and dental health of elementary school students.
References
- 1.McDonald RE, Avery DR, George KS. Dental caries in the child and adolescent. In: McDonald RE, Avery DR, Dean JA: Dentistry for the Child and Adolescent. 8th ed. St. Louis: Mosby; 2004. 205-32 [Google Scholar]
- 2.Clarkson JJ, McLoughlin J. Role of flouride in oral health promotion. Int Dent J. 2000;50:119–28. doi: 10.1111/j.1875-595x.2000.tb00552.x. [DOI] [PubMed] [Google Scholar]
- 3.Nowak AJ, Call JJ. Prevention of dental disease. In: Pinkham JR, Casamssimo PS, Fields HW, Nowak AJ: Pediatric Dentistry: Infancy through Adolescence. 4th ed. St. Louis: Elsevier Saunders; 2005. 513-9 [Google Scholar]
- 4.Volker JF, Russle DL. The prevention of dental caries with fluoride. In: Finn SB: Clinical Pedodontics. 4th ed. Philadelphia: Saunders; 1998. 495-516 [Google Scholar]
- 5.Roberson TM, Lundeen TF. Cariology: The lesion, etiology, prevention, and control. In: Roberson MR, Heymann HO, Swift EJ: Sturdevant’s Art and Sience of Operative Dentistry. St. Louis: Mosby; 2002. 98-129 [Google Scholar]
- 6.Koch G, Modeer T, Poulsen S, Rasmussen P. Pedodontics: A Clinical Approach. 3rd ed. Copenhagen: Munksgaard; 1997. [Google Scholar]
- 7.Hosseinpour A. Evaluation of effect of 0.2% sodium fluoride mouthwash on caries in guidance schools of Showt, Maku. [Graduation Thesis], Tabriz University of Medical Sciences; 2005.
- 8.Kanellis MJ, Warren JJ, Damiano PC. Dental public health issues in pediatric dentistry. In: pinkham JR, Casamssimo PS, Fields HW, Nowak AJ: Pediatric Dentistry: Infancy through Adolescence. St. Louis: Elsevier Saunders; 2005. 160-4 [Google Scholar]
- 9.Birkeland KM, Broch L, Jorkjend L. Benefits and prognoses following 10 years of a fluoride mouthrinsing program. Scand J Dent Res. 1997;85:31–7. doi: 10.1111/j.1600-0722.1977.tb00528.x. [DOI] [PubMed] [Google Scholar]
- 10.Bawden JW, Granath L, Holst K, koch G, Krasse P, Rootzen H. Effect of mouthrinsing with a sodium fluoride solution in children with different caries experience. Swed Dent J. 1980;4:111–7. [PubMed] [Google Scholar]
- 11.Ripa LW, Leske GS, Sposato A, Rebich T. Supervised Weekly rinsing with a 02 percent neutral NaF solution: final results of a demonstration program after six school years. J Public Health Dent. 1983;43:53–62. doi: 10.1111/j.1752-7325.1983.tb01112.x. [DOI] [PubMed] [Google Scholar]
- 12.Leverett DH, Sveen OB, Jensen OE. Weekly rinsing with a fluoride mouthrinse in an unfluoridated community: results after seven years. J Public Health Dent. 1985;45:95–100. doi: 10.1111/j.1752-7325.1985.tb01945.x. [DOI] [PubMed] [Google Scholar]
- 13.Clark DC, Robert G, Tessier C, Frechette N, Le Blanc G, Boucher L, et al. The results after 20 months of a study testing the efficacy of a weekly fluoride mouthrinsing program. J Public Health Dent. 1985;45:252–6. doi: 10.1111/j.1752-7325.1985.tb01159.x. [DOI] [PubMed] [Google Scholar]
- 14.Horowitz HS, Meyers RJ, Heifetz SB, Driscoll WS, Li SH. Combined fluoride school-based program in a fluoride-deficient area: results of an 11-year study. J Am Dent Assoc. 1986;112:621–5. doi: 10.14219/jada.archive.1986.0090. [DOI] [PubMed] [Google Scholar]
- 15.Ruilen R, Truin GJ, Konig K, Vogels A, van’t Hof M. Clinical cariostatic effectiveness of a NaF rinse in a low prevalence child population. Community Dent Oral Epidemiol. 1987;15:57–9. doi: 10.1111/j.1600-0528.1987.tb00481.x. [DOI] [PubMed] [Google Scholar]
- 16.Molina MX, Rodriguez FG, Urbina T, Vargas S. Effect of weekly mouthrinses with 02% neutral NaF solution on caries incidence in first permanent molars. Odontol Chil. 1989;37:176–82. [PubMed] [Google Scholar]
- 17.Heidmann J, Poulsen S, Arnbjerg D, Kirkegaard E, Laurberg Laurberg. Caries development after termination of a fluoride rinsing program. Community Dent Oral Epidemiol. 1992;20:118–21. doi: 10.1111/j.1600-0528.1992.tb01543.x. [DOI] [PubMed] [Google Scholar]
- 18.Yoshihara A, Kobayashi S, Yagi M, Horii K. Benefits of a community oriented fluoride mouth rinsing program. Nippon Koshu Eisei Zasshi. 1993;40:1054–61. [PubMed] [Google Scholar]
- 19.Sterritt GR, Frew RA, Rozier RG. Evaluation of Guamanian dental caries preventive programs after 13 years. J Public Health Dent. 1994;54:153–9. doi: 10.1111/j.1752-7325.1994.tb01207.x. [DOI] [PubMed] [Google Scholar]
- 20.Louw AJ, Carstens IL, Hartshorne JE, Blignaut RG. Effectiveness of two school-based caries preventive programmes. J Dent Assoc S Art. 1995;50:43–9. [PubMed] [Google Scholar]
- 21.Kobayashi S, Kishi H, Yoshihara A, Horri K, Tsutsui A, Himeno T, et al. Treatment and posttreatment effects of fluoride mouthrinsing after 17 years. J Public Health Dent. 1995;55:229–33. doi: 10.1111/j.1752-7325.1995.tb02374.x. [DOI] [PubMed] [Google Scholar]
- 22.Yamaguchi N, Saito T, Oho T, Sumi Y, Yamashita Y, Koga T. Influence of the discontinuation of a school-based, supervised fluoride mouthrising programme on the prevalence of dental caries. Community Dent Health. 1997;14:258–61. [PubMed] [Google Scholar]
- 23.Tapias MA, De Miguel G, Jimenez-Garicia R, Gonzalez A, Dominguez V. Incidence of caries in an infant population in Mostoles, MadridEvaluation of a preventive program after 75 years of follow-up. Int J Paediatr Dent. 2001;11:440–60. doi: 10.1046/j.0960-7439.2001.00307.x. [DOI] [PubMed] [Google Scholar]
- 24.Marinho VCC, Higgins JPT, Logan S, Sheiham A. Fluoride mouthrinses for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. 2003;3:CD002284. doi: 10.1002/14651858.CD002284. [DOI] [PubMed] [Google Scholar]
- 25.Twetman S, Petersson L, Axelsson S, Dahlgern H, Holm AK, Kallestal C. Caries-preventive effect of sodium fluoride mouthrinses: a systemic review of controlled clinical trials. Acta Odontol Scand. 2004;62:223–30. doi: 10.1080/00016350410001658. [DOI] [PubMed] [Google Scholar]
- 26.Skold UM. On caries prevalence and school-based fluoride programmes in Swedish Adolescents. Swed Dent J Suppl. 2005;178:11–75. [PubMed] [Google Scholar]
- 27.Poulsen S, Kirkegaard E, Bangsbo G, Bro K. Caries clinical trial of fluoride rinses in a Danish Public Child Dental Service. Community Dent Oral Epidemiol. 1984;12:283–7. doi: 10.1111/j.1600-0528.1984.tb01456.x. [DOI] [PubMed] [Google Scholar]
- 28.Disney JA, Graves RC, Stamm JW, Bohannan HM, Abernathy JR. Comparative effects of a 4-year fluoride mouthrinse program on high and low caries forming grade 1 children. Community Dent Oral Epidemiol. 1989;17:139–43. doi: 10.1111/j.1600-0528.1989.tb00008.x. [DOI] [PubMed] [Google Scholar]
- 29.Chikte UM, Lewis HA, Rudolph MJ. The effectiveness of a school-based fluoride mouth rinse programme. J Dent Assoc A Art. 1996;51:697–700. [PubMed] [Google Scholar]
- 30.Holland TJ, Whelton H, O’Mullane DM, Creedon P. Evaluation of a fortnightly school-based sodium fluoride mouthrinse 4 years following its cessation. Caries Res. 1995;29:431–4. doi: 10.1159/000262109. [DOI] [PubMed] [Google Scholar]