

Abstract
Background:
Patients with chronic kidney disease (CKD) and end-stage renal disease (ESRD) have a high prevalence of obstructive sleep apnea (OSA) that can have significant clinical implications. An accurate clinical screening tool for OSA that identifies patients for further diagnostic testing would assist in the identification of this comorbidity. The Berlin Questionnaire (BQ), Adjusted Neck Circumference (ANC), and STOP-BANG questionnaire are 3 such instruments that have been validated in patients with normal kidney function.
Objective:
The objective of this study was to determine the validity of these screening instruments in patients with CKD and ESRD, using overnight cardiopulmonary monitoring to diagnose OSA.
Methods:
One hundred seventy-two patients were recruited from nephrology clinics and hemodialysis units (CKD: n = 109; ESRD: n = 63). All patients completed the BQ, ANC, STOP-BANG, and overnight cardiopulmonary monitoring to diagnose OSA (respiratory disturbance index [RDI] ≥ 15). Sensitivity, specificity, positive and negative predictive values, and accuracy were calculated for the BQ, ANC, and STOP-BANG.
Results:
Obstructive sleep apnea was present in 41 CKD patients (38%) and 32 ESRD patients (51%). All screening instruments had satisfactory sensitivity (56% to 94%) but poor specificity (29% to 77%) and low accuracy (51% to 69%) in both CKD and ESRD patients with RDI ≥ 15. Using an RDI ≥ 30 yielded similar results.
Conclusions:
Current screening questionnaires do not accurately identify patients at high risk for OSA or rule out the presence of OSA in patients with CKD and ESRD. Consequently, objective monitoring during sleep is required to reliably identify sleep apnea in these patient populations.
Citation:
Nicholl DDM; Ahmed SB; Loewen AHS; Hemmelgarn BR; Sola DY; Beecroft JM; Turin TC; Hanly PJ. Diagnostic value of screening instruments for identifying obstructive sleep apnea in kidney failure. J Clin Sleep Med 2013;9(1):31-38.
Keywords: Obstructive sleep apnea, chronic kidney disease, end-stage renal disease, Berlin questionnaire, adjusted neck circumference, STOP-BANG questionnaire
Obstructive sleep apnea (OSA) is common in patients with chronic kidney disease (CKD)1–7 and end-stage renal disease (ESRD).1,8–12 The prevalence of OSA in these populations has been reported to range from 27% to 54% in CKD patients2,3,5–7 and 45% to 70% in ESRD patients,1,8–12 which is significantly higher than the general population.13 Further, the clinical presentation of OSA in the CKD and ESRD populations differs from that in the general sleep apnea population, reflected by a lower prevalence of sleep related symptoms.14,15 Consequently, OSA is more likely to be unrecognized in these populations.
The co-existence of OSA in patients with CKD and ESRD is clinically relevant and has potential to alter important outcomes. In addition to causing impairment of sleep quality and daytime function,16,17 OSA increases the risk of vascular disease18,19 and systemic hypertension,20 both of which are common complications of CKD and ESRD.21 OSA may also accelerate the deterioration of kidney function in patients with CKD, either directly through the effect of hypoxia on the kidney22–24 or indirectly through increases in systemic blood pressure, inflammatory cytokines, and sympathetic nervous system activity.25–28 OSA can be effectively treated in many patients with continuous positive airway pressure (CPAP).29 Consequently, it is important that OSA be recognized and formally diagnosed in these patient populations.
BRIEF SUMMARY
Current Knowledge/Study Rationale: Patients with Chronic kidney disease (CKD) and end-stage renal disease (ESRD have a high prevalence of obstructive sleep apnea (OSA) which can have a significant impact on clinical outcomes. We sought to determine the validity of existing OSA screening instruments in patients with CKD and ESRD.
Study Impact: Current OSA screening questionnaires do not accurately identify patients at risk for OSA and do not rule out the presence of OSA in patients with CKD and ESRD. Consequently, objective cardiopulmonary monitoring is needed to reliably identify OSA in these populations.
Several instruments have been developed to screen patients for OSA in order to direct objective diagnostic monitoring to those considered at high risk of having the disorder. Given the high prevalence of OSA in patients with CKD and ESRD, an instrument to screen for OSA in these populations would be useful. The Berlin Questionnaire (BQ),30 adjusted neck circumference (ANC),31,32 and STOP-BANG33 questionnaire are three such instruments that have been validated in patients with normal kidney function, but not in patients with CKD and ESRD. The objective of this study was to determine the diagnostic value of these screening instruments in patients with CKD and ESRD, using overnight cardiopulmonary monitoring to diagnose OSA.
METHODS
Study Subjects
Consecutive adult patients (≥ 18 years) with CKD (defined by an estimated GFR [eGFR] < 60 mL/min/1.73m2)34 and ESRD (requiring thrice weekly conventional hemodialysis) attending outpatient nephrology clinics and dialysis units in Calgary, Alberta, Canada, were invited to participate in the study. eGFR at the time of the study visit was calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation.35 Exclusion criteria were current treatment with supplemental oxygen, tracheostomy, Cheyne-Stokes respiration (CSR), and inability to give informed consent. Patients currently treated with CPAP therapy were included in the study if their original diagnostic sleep study and sleep questionnaire were available for review and their eGFR at the time of OSA diagnosis was known. The study was approved by the University of Calgary Conjoint Health Research Ethics Board. Informed consent was obtained from all participants in accordance with the Declaration of Helsinki.
Screening Instruments
All patients completed a sleep history questionnaire, which included questions regarding a history of snoring, witnessed apnea during sleep, and nocturnal choking. Additionally, the questionnaire surveyed demographic information and medical history, including a history of hypertension, vascular disease (angina, myocardial infarction, coronary artery bypass surgery, congestive heart failure, stroke, or transient ischemic attack), and diabetes. Each patient's risk of having OSA was estimated from the BQ,30 calculation of the ANC,31,32 and STOP-BANG questionnaire.33
Based on the history of snoring (category 1), daytime sleepiness or fatigue (category 2), and hypertension/obesity (BMI > 30 kg/m2) (category 3), the BQ considers frequent and persistent symptoms in 2 of these 3 categories to indicate a high risk of OSA (Appendix).30 The BQ has a sensitivity of 54% and specificity of 97% for a designation criterion of respiratory disturbance index (RDI) ≥ 15 and a sensitivity of 17% and specificity of 97% for a designation criterion of RDI ≥ 30 in a primary care population.30
The ANC is calculated by measuring the patient's neck circumference (in centimetres) and adding additional centimetres if there is a history of hypertension (4 cm), habitual snoring (3 cm), and nocturnal choking (3 cm).31,32 An ANC < 43 indicates a low probability of sleep apnea, 43-48 intermediate probability (4 to 8 times as probable as low probability), and > 48 indicates a high probability (20 times as probable).31,32
The STOP-BANG questionnaire consists of 4 simple yes/no questions regarding habitual snoring, tiredness/sleepiness, observed apneas, and high blood pressure.33 An additional point is added for each of the following clinical characteristics: BMI > 35 kg/m2, age > 50 years, neck circumference > 40 cm, and male gender. A score ≥ 3 out of a total possible score of 8 is considered high risk for OSA. The STOP-BANG questionnaire has a sensitivity of 92.9% and specificity of 43.0% for a designation criterion of RDI ≥ 15, and a sensitivity of 100% and specificity of 37% for a designation criterion of RDI ≥ 30.33
Diagnosis of OSA
All patients, regardless of OSA symptoms, performed an unattended, overnight cardiopulmonary monitoring study at home (Remmers Sleep Recorder Model 4.2, Saga Tech Electronic, Calgary, AB, Canada) to determine OSA status. ESRD patients underwent the overnight study after a non-dialysis day. The monitor consists of an oximeter to record oxyhemoglobin saturation (SpO2) and heart rate variability, a pressure transducer to record nasal airflow, a microphone to record snoring, and a body position sensor. The oximeter provides the data for an automated scoring algorithm, which calculates the RDI based on the number of episodes of oxyhemoglobin desaturation ≥ 4% per hour of monitoring. Nocturnal oxygen saturation was sampled at 1 Hz. The Remmers Sleep Recorder has been validated by comparison to attended polysomnography.36,37 Sleep apnea was defined as RDI ≥ 15 and RDI ≥ 30, which correspond with moderate-severe and severe sleep apnea, respectively, and are most likely to be clinically significant. The Remmers Sleep Recorder has a sensitivity of 98% and specificity of 88% for a designation criterion of RDI ≥ 15, and a sensitivity of 95% and specificity of 93% for a designation criterion of RDI ≥ 30.37 The raw data were reviewed by a sleep medicine physician (PJH), blinded to patients' kidney function and symptoms, who confirmed that the estimated RDI was accurate and determined whether apnea was central (CSR) or obstructive (OSA), based on the morphology of the airflow recordings. Nasal pressure recordings with a characteristic crescendo/decrescendo pattern and no evidence of airflow limitation were classified as CSR, whereas recordings without a crescendo/decrescendo pattern and with airflow limitation were classified as OSA.
Analysis
Data are presented as mean ± standard deviation or number (percentage), unless otherwise indicated. Estimated OSA risk, as assessed by the BQ, ANC, and STOP-BANG questionnaire, was compared to the diagnosis of OSA (RDI ≥ 15 and ≥ 30, respectively) as determined by objective cardiopulmonary monitoring for both CKD and ESRD patients. Subjects with CSR were excluded from our primary analyses, but were included as part of a sensitivity analysis. Sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV), accuracy (total number of correct risk assessments divided by total number of risk assessments), and area under the receiver operating characteristic (ROC) curve (AUC) were calculated for high risk for the BQ, both moderate to high risk (≥ 43 cm) and high risk (> 48 cm) for the ANC, and high risk for the STOP-BANG questionnaire at moderate (RDI ≥ 15) and severe (RDI ≥ 30) diagnostic criteria for OSA. These were undertaken for CKD and ESRD patients separately. The unpaired t-test or the Mann-Whitney U-test was used for comparisons between continuous variables, while the χ2 test with Fischer's Exact Test was used for dichotomous variables. Finally, we examined the impact of using higher thresholds to assess OSA risk in the ANC (> 53 cm) and the STOP-BANG questionnaire (' 4). All statistical analyses were two-sided and performed with SPSS V.17.0 (SPSS, Chicago, IL, USA). P-values < 0.05 were considered statistically significant.
RESULTS
Patient Recruitment
Six hundred fifty-seven patients were informed of the study between May 2007 and November 2010 (Figure 1); 254 patients declined to participate. In addition, eGFR was too high (≥ 60) in 87 patients, and 14 patients did not complete the questionnaires. The remaining 302 patients (CKD, n = 174; ESRD, n = 128) were eligible for cardiopulmonary monitoring, which was declined by 116 patients (CKD: n = 61; ESRD: n = 56). One hundred thirteen CKD patients and 72 ESRD patients completed cardiopulmonary monitoring. Thirteen patients with CSR (CKD, n = 4; ESRD, n = 9) were excluded from further analyses, resulting in a final study population of 109 CKD patients and 63 ESRD patients. Eight CKD patients and 5 ESRD patients were currently treated with CPAP.
Figure 1. Patient recruitment.
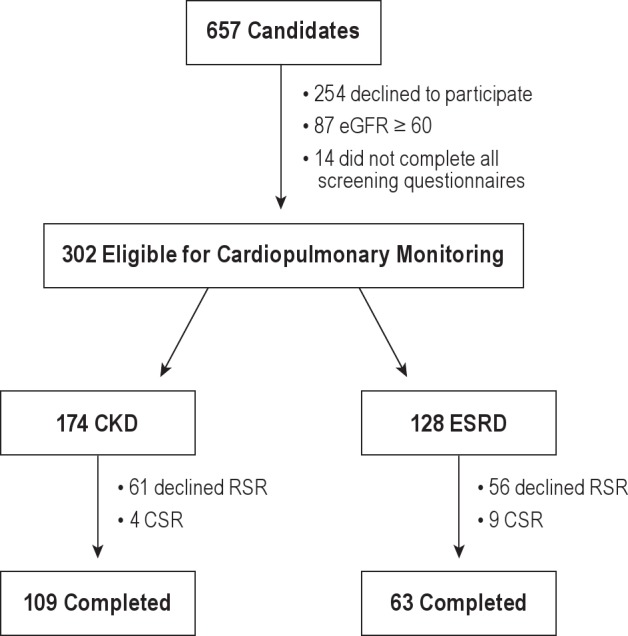
CSR, Cheyne-Stokes respiration; CKD, chronic kidney disease; eGFR, estimated glomerular filtration rate; ESRD, end-stage renal disease; RSR, Remmers Sleep Recorder.
Chronic Kidney Disease
Patient Characteristics
CKD patient characteristics stratified by OSA status (RDI ≥ 15) are presented in Table 1. The mean duration of nocturnal cardiopulmonary monitoring was 7.3 ± 1.5 h for CKD patients, while the proportion of monitoring time that patients reported sleeping was 81% ± 15%. Consequently, estimated sleep efficiency and monitoring time were sufficiently long to capture important respiratory events. Moderate to severe OSA (RDI ≥ 15) was present in 38% of CKD patients. Using a more conservative definition of OSA (RDI ≥ 30), the prevalence of OSA remained high at 23%. As expected, the severity of associated nocturnal hypoxemia was greater in CKD patients with OSA. CKD patients with OSA had an increased BMI and greater neck circumference, but did not differ from CKD patients without OSA in terms of age or gender distribution.
Table 1.
Chronic kidney disease patient characteristics

There were no differences in the individual categories or the final assessed risk of the BQ between CKD patients with and without OSA, although category 1 (snoring) and final risk were of borderline significance. Using the ANC, CKD patients with OSA had greater neck circumference than CKD patients without OSA, although nocturnal choking was of borderline significance. However, these components contributed to higher ANC scores, which resulted in a greater proportion of CKD patients with OSA being assessed as higher risk. Component analyses of the STOP-BANG questionnaire revealed that CKD patients with OSA were more likely to report a history of witnessed apneas, have a BMI > 35 kg/m2, and neck circumferences > 40 cm. Male gender and age > 50 years were of borderline significance. Accordingly, this corresponded to higher STOP-BANG total scores and a greater proportion of CKD patients with OSA being assessed as high risk.
Performance of Screening Instruments
The sensitivity, specificity, PPV, and NPV for a positive BQ, ANC, and STOP-BANG to identify OSA in patients with CKD using RDI thresholds of 15 and 30 are shown in Table 2.
Table 2.
Diagnostic value of obstructive sleep apnea screening instruments in chronic kidney disease patients

Using an RDI ≥ 15, the BQ, ANC ≥ 43, and STOP-BANG performed with good sensitivity but poor specificity; an ANC > 48 had a modest sensitivity and specificity. The BQ, ANC, and STOP-BANG had good NPVs, but poor PPVs. The accuracies of the BQ, ANC ≥ 43, ANC > 48, and STOP-BANG were 52%, 58%, 69%, and 54%, respectively, for identifying OSA at an RDI ≥ 15.
At an RDI ≥ 30, the BQ, ANC ≥ 43, and STOP-BANG had high sensitivity but poor specificity, while an ANC > 48 had both a modest sensitivity and specificity. The BQ, ANC, and STOP-BANG had good NPVs, but poor PPVs. The accuracies of the BQ, ANC ≥ 43, ANC > 48, and STOP-BANG were 45%, 47%, 69%, and 45%, respectively, for identifying OSA using a RDI ≥ 30.
Inclusion of the 4 subjects with CSR did not alter these results. Increasing the threshold for the ANC (> 53) resulted in improved specificity and PPV at the expense of reduced sensitivity and NPV. Accuracy was not improved at RDI ≥ 15, but was improved to 76% at RDI ≥ 30. Increasing the threshold for the STOP-BANG (≥ 4) improved specificity and PPV and mildly reduced sensitivity and NPV at both RDI thresholds. Accuracy was increased to 64% at RDI ≥ 15 and 57% at RDI ≥ 30.
End-Stage Renal Disease
Patient Characteristics
ESRD patient characteristics stratified by OSA status (RDI ≥ 15) are presented in Table 3. The mean duration of nocturnal cardiopulmonary monitoring was 6.4 ± 2.0 h for ESRD patients, while the proportion of monitoring time that patients reported sleeping was 78% ± 18% for ESRD. Consequently, monitoring time and estimated sleep efficiency were sufficiently long to capture important respiratory events. Moderate to severe OSA (RDI ≥ 15) was present in 51% of ESRD patients, and the prevalence of severe OSA (RDI ≥ 30) was also high at 40%. The severity of nocturnal hypoxemia was greater in ESRD patients with OSA. ESRD patients with OSA had an increased BMI and greater neck circumference, but did not differ from ESRD patients without OSA in terms of age or gender distribution.
Table 3.
End-stage renal disease patient characteristics

There were no differences in the individual categories or the final assessed risk of the BQ between ESRD patients with and without OSA. Similarly, apart from neck circumference, there were no differences in the other components of the ANC between ESRD patients with and without OSA. However, the increased neck circumference resulted in higher ANC scores and corresponded to a greater proportion of ESRD patients with OSA being assessed as higher risk. Component analyses of the STOP-BANG questionnaire revealed that ESRD patients with OSA were more likely to report loud snoring, a history of witnessed apneas, have a BMI > 35 kg/m2, and neck circumferences > 40 cm. Accordingly, this resulted in higher STOP-BANG total scores and a greater proportion of ESRD patients with OSA being assessed as high risk.
Performance of Screening Instruments
The sensitivity, specificity, PPV, and NPV for a positive BQ, ANC, and STOP-BANG in identifying OSA in ESRD patients are shown in Table 4.
Table 4.
Diagnostic value of obstructive sleep apnea screening instruments in end-stage renal disease patients
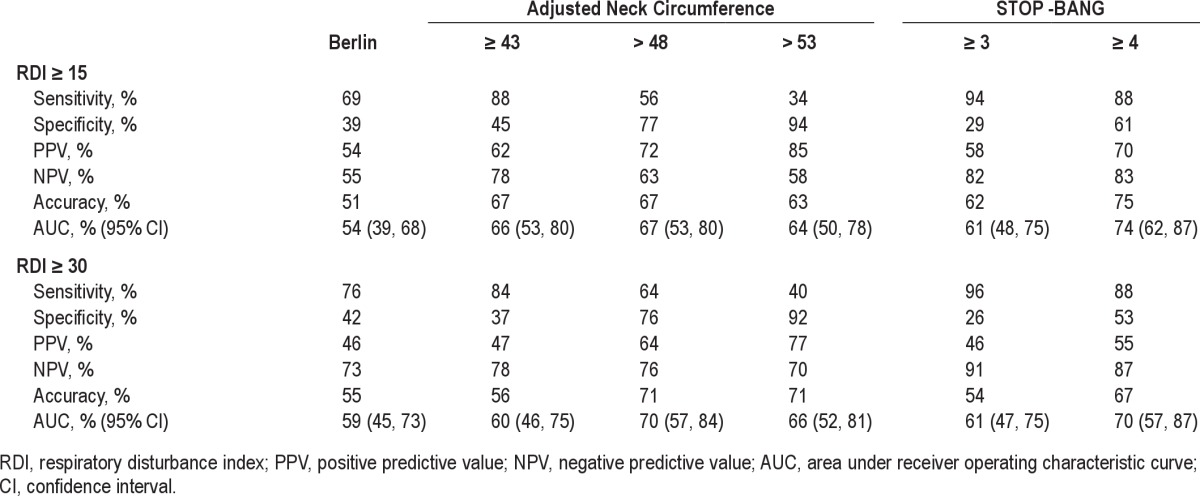
At an RDI ≥ 15, an ANC ≥ 43 and STOP-BANG had good sensitivity, but poor specificity. The BQ had modest sensitivity but poor specificity, while an ANC > 48 had both modest sensitivity and specificity. Each screening instrument had a moderate PPV and NPV. The accuracies of the BQ, ANC ≥ 43, ANC > 48, and STOP-BANG were 51%, 67%, 67%, and 62%, respectively, for determining OSA using RDI ≥ 15.
At an RDI ≥ 30, the BQ and an ANC ≥ 43 had moderate sensitivity and NPV, but poor specificity and PPV. An ANC > 48 had moderate sensitivity, specificity, PPV, and NPV. The STOP-BANG had excellent sensitivity and NPV, but poor specificity and PPV. The accuracies of the BQ, ANC ≥ 43, ANC > 48, and STOP-BANG were 55%, 56%, 71%, and 54%, respectively, for determining OSA using a RDI ≥ 30.
Inclusion of the 9 subjects with CSR did not alter these results. Increasing the threshold for the ANC (> 53) resulted in improved specificity and PPV at the expense of reduced sensitivity and NPV, but did not improve accuracy, at both RDI ≥ 15 and ≥ 30. However, increasing the threshold for the STOP-BANG (≥ 4) improved specificity and PPV, while maintaining good sensitivity and NPV at both RDI thresholds. Accuracy was increased to 75% at an RDI ≥ 15 and 67% at an RDI ≥ 30.
DISCUSSION
This is the first study to systematically examine the validity of OSA screening questionnaires in the CKD and ESRD populations using objective cardiopulmonary monitoring to diagnose OSA. We found that (a) OSA screening instruments had limited accuracy in the CKD and ESRD populations, with accuracies ranging between 45% to 69% in CKD patients and 51% to 71% in ESRD patients at RDI levels of 15 and 30, respectively; (b) the ANC was the most accurate screening tool in both the CKD and ESRD populations; (c) the ANC and STOP-BANG assigned more CKD and ESRD patients with OSA as high risk; and (d) the BQ was unable to distinguish between CKD and ESRD patients with and without OSA.
Several small studies have reported increased OSA risk in the dialysis38–40 and transplant41 populations using the Berlin questionnaire, but in contrast to this study, none included objective overnight monitoring to confirm the diagnosis of OSA. We found that the BQ had a better sensitivity but poorer specificity and predictive value in both the CKD and ESRD populations compared to measures obtained in the initial validation in the primary care setting.30 The ANC has not been validated outside of a sleep centre population.31,32 The STOP-BANG questionnaire performed similarly in our CKD and ESRD populations to what has previously been reported in the preoperative assessment of surgical patients33 and in a more recent community study.42
In order to screen patients for a disorder with an important health outcome, a good screening tool requires a high sensitivity with an acceptable specificity. Overall, we found the BQ, ANC, and STOP-BANG demonstrated high sensitivities, but the specificities were significantly below acceptable levels. High sensitivities are useful in order to avoid missing cases that may lead to adverse health outcomes and healthcare costs, but low specificities result in the inclusion of low-risk patients and higher false positive rates. This limits the utility of these screening tools in the patient population we studied. Given the good negative predictive values we found, there may be a role for these screening questionnaires to exclude OSA and avoid further testing. However, further evaluation will be required in those who have a positive screening questionnaire. Of interest, increasing the thresholds for the ANC and STOP-BANG questionnaire did improve accuracy in our CKD and ESRD patients. However, further studies are required to examine the use of alternative thresholds for OSA diagnosis in these populations, as well as to examine the implications and efficacy of these screening strategies. The poor performance of the BQ is consistent with what has been demonstrated in other disease-specific populations. Although the BQ performed well in the primary-care setting30 and in patients with atrial fibrillation43 and resistant hypertension,44 it did not effectively screen for OSA in the stroke,45 systemic hypertension,46 and sleep clinic populations,47 nor in patients who were evaluated following acute myocardial infarction.48 To date, the ANC and the STOP-BANG have not been validated in disease-specific populations.
The high prevalence of hypertension, which was found in over 90% of our patients and was equally common in those with and without OSA, is one reason the BQ, ANC, and STOP-BANG were unable to reliably distinguish patients with and without OSA in the CKD and ESRD populations. By definition, most CKD and ESRD patients have hypertension either as a cause or consequence of kidney disease.21 Additionally, the reliance of these screening questionnaires on sleep related symptoms, such as snoring, witnessed apneas, nocturnal choking, and daytime sleepiness, limit their accuracy in CKD and ESRD patients, as these populations are less likely to present with the stereotypical features of OSA.14,15 Furthermore, fatigue is a common symptom of CKD and ESRD, which can overlap with complaints of sleepiness and develop independently of sleep disordered breathing.49,50 Fluid status is another potential confounder that is thought to influence upper airway obstruction and neck circumference in kidney failure patients.51–54 Although it is possible that fluid accumulation in the neck accounted for some of the increased neck circumference in patients with OSA, our study was not designed to evaluate this. However, we tried to minimize the potential for fluid status to confound our results by standardizing when ESRD patients were evaluated in relation to the time they received dialysis. Further, the dichotomous categorization of age (> 50 years) used in the STOP-BANG questionnaire is also a limitation as CKD and ESRD are more prevalent in the elderly.55 Consequently, the presence of these factors could significantly reduce the accuracy of these screening tools.
Our study has a number of strengths. First, we recruited a relatively large sample size from a renal population representative of the general CKD and ESRD populations, which increases the relevance of our findings to these patient populations. In fact, our CKD population had a similar clinical profile to the Chronic Renal Insufficiency Cohort study,56 and our ESRD population resembled a larger cohort of ESRD patients from the Southern Alberta Renal Program.57 Second, we used the same methodology, including objective cardiopulmonary monitoring, in patients with a broad spectrum of kidney disease, which enabled us to compare the accuracy of these screening instruments in the CKD and ESRD populations. Third, no inclusion or exclusion criteria were set with respect to age, gender, comorbidities, or medications, which improved the generalizability of our findings to the CKD and ESRD populations. Notwithstanding these strengths, our study also has limitations. First, the potential for selection bias exists as patients attending the nephrology clinics may have been more likely to participate if they suspected they had sleep apnea. We tried to limit this by emphasising that sleep related complaints were not required for recruitment. If such a bias did exist, it should have been reflected in a higher prevalence of sleep related symptoms and higher accuracy of the screening instruments, which was not the case. Second, we used portable monitoring in place of polysomnography. The RDI was calculated based on monitoring time rather than objective sleep duration and thus the frequency of OSA events could have been underestimated. Further, this methodology did not employ a measurement of respiratory effort and consequently we could only estimate the prevalence of central sleep apnea based on the morphology of the nasal pressure recording. We addressed these potential limitations by asking patients to estimate their sleep time, and having the portable monitoring results reviewed by a sleep medicine physician to determine whether the findings were consistent with either Cheyne-Stokes respiration or OSA.
In summary, our study demonstrates that current screening questionnaires do not accurately identify patients at high risk for OSA or rule out the existence of OSA in patients with CKD and ESRD. This is unfortunate given the high prevalence of OSA in these patient populations1–12 and its potential impact on important clinical outcomes.16–20,22,23,24,25,26,27–28 Further studies are required to develop and validate more accurate screening strategies for OSA in patients with CKD and ESRD. In the meantime, objective cardiopulmonary monitoring during sleep is required to reliably identify sleep apnea in these patients.
DISCLOSURE STATEMENT
This was not an industry supported study. The authors have indicated no financial conflicts of interest.
ACKNOWLEDGMENTS
The authors thank the Southern Alberta Renal Program for assistance with patient recruitment, the FMC Sleep Centre for sleep diagnostic testing, and Ms. Patty Nielsen for her clerical assistance. This research was supported by Alberta Innovates–Health Solutions, O'Brien Centre, University of Calgary, and the Department of Medicine, University of Calgary. An abstract for this study was presented at the American Society of Nephrology Kidney Week in Philadelphia, PA, November 8-13, 2011.
Appendix.
Berlin Questionnaire and scoring algorithm

REFERENCES
- 1.Kimmel PL, Miller G, Mendelson WB. Sleep apnea syndrome in chronic renal disease. Am J Med. 1989;86:308–14. doi: 10.1016/0002-9343(89)90301-x. [DOI] [PubMed] [Google Scholar]
- 2.Markou N, Kanakaki M, Myrianthefs P, et al. Sleep-disordered breathing in nondialyzed patients with chronic renal failure. Lung. 2006;184:43–9. doi: 10.1007/s00408-005-2563-2. [DOI] [PubMed] [Google Scholar]
- 3.Canales MT, Lui LY, Taylor BC, et al. Renal function and sleep-disordered breathing in older men. Nephrol Dial Transplant. 2008;23:3908–14. doi: 10.1093/ndt/gfn364. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Sim JJ, Rasgon SA, Kujubu DA, et al. Sleep apnea in early and advanced chronic kidney disease: Kaiser Permanente Southern California cohort. Chest. 2009;135:710–6. doi: 10.1378/chest.08-2248. [DOI] [PubMed] [Google Scholar]
- 5.Roumelioti ME, Buysse DJ, Sanders MH, Strollo P, Newman AB, Unruh ML. Sleep-disordered breathing and excessive daytime sleepiness in chronic kidney disease and hemodialysis. Clin J Am Soc Nephrol. 2011;6:986–94. doi: 10.2215/CJN.05720710. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sakaguchi Y, Shoji T, Kawabata H, et al. High prevalence of obstructive sleep apnea and its association with renal function among nondialysis chronic kidney disease patients in Japan: a cross-sectional study. Clin J Am Soc Nephrol. 2011;6:995–1000. doi: 10.2215/CJN.08670910. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Nicholl DD, Ahmed SB, Loewen AH, et al. Declining kidney function increases the prevalence of sleep apnea and nocturnal hypoxia. Chest. 2012;141:1422–30. doi: 10.1378/chest.11-1809. [DOI] [PubMed] [Google Scholar]
- 8.Wadhwa NK, Mendelson WB. A comparison of sleep-disordered respiration in ESRD patients receiving hemodialysis and peritoneal dialysis. Adv Perit Dial. 1992;8:195–8. [PubMed] [Google Scholar]
- 9.Wadhwa NK, Seliger M, Greenberg HE, Bergofsky E, Mendelson WB. Sleep related respiratory disorders in end-stage renal disease patients on peritoneal dialysis. Perit Dial Int. 1992;12:51–6. [PubMed] [Google Scholar]
- 10.Stepanski E, Faber M, Zorick F, Basner R, Roth T. Sleep disorders in patients on continuous ambulatory peritoneal dialysis. J Am Soc Nephrol. 1995;6:192–7. doi: 10.1681/ASN.V62192. [DOI] [PubMed] [Google Scholar]
- 11.Unruh ML, Sanders MH, Redline S, et al. Sleep apnea in patients on conventional thrice-weekly hemodialysis: comparison with matched controls from the Sleep Heart Health Study. J Am Soc Nephrol. 2006;17:3503–9. doi: 10.1681/ASN.2006060659. [DOI] [PubMed] [Google Scholar]
- 12.Hanly PJ, Pierratos A. Improvement of sleep apnea in patients with chronic renal failure who undergo nocturnal hemodialysis. N Engl J Med. 2001;344:102–7. doi: 10.1056/NEJM200101113440204. [DOI] [PubMed] [Google Scholar]
- 13.Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. The occurrence of sleep-disordered breathing among middle-aged adults. N Engl J Med. 1993;328:1230–5. doi: 10.1056/NEJM199304293281704. [DOI] [PubMed] [Google Scholar]
- 14.Nicholl DD, Ahmed SB, Loewen AH, et al. Clinical presentation of obstructive sleep apnea in patients with chronic kidney disease. J Clin Sleep Med. 2012;8:381–7. doi: 10.5664/jcsm.2028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Beecroft JM, Pierratos A, Hanly PJ. Clinical presentation of obstructive sleep apnea in patients with end-stage renal disease. J Clin Sleep Med. 2009;5:115–21. [PMC free article] [PubMed] [Google Scholar]
- 16.Malhotra A, White DP. Obstructive sleep apnoea. Lancet. 2002;360:237–45. doi: 10.1016/S0140-6736(02)09464-3. [DOI] [PubMed] [Google Scholar]
- 17.Bennett LS, Barbour C, Langford B, Stradling JR, Davies RJ. Health status in obstructive sleep apnea: relationship with sleep fragmentation and daytine sleepiness, and effects of continuous positive airway pressure treatment. Am J Respir Crit Care Med. 1999;159:1884–90. doi: 10.1164/ajrccm.159.6.9808107. [DOI] [PubMed] [Google Scholar]
- 18.Marin JM, Carrizo SJ, Vicente E, Agusti AG. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet. 2005;365:1046–53. doi: 10.1016/S0140-6736(05)71141-7. [DOI] [PubMed] [Google Scholar]
- 19.Redline S, Yenokyan G, Gottlieb DJ, et al. Obstructive sleep apnea-hypopnea and incident stroke: the sleep heart health study. Am J Respir Crit Care Med. 2010;182:269–77. doi: 10.1164/rccm.200911-1746OC. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Peppard PE, Young T, Palta M, Skatrud J. Prospective study of the association between sleep-disordered breathing and hypertension. N Engl J Med. 2000;342:1378–84. doi: 10.1056/NEJM200005113421901. [DOI] [PubMed] [Google Scholar]
- 21.National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis. 2002;39:S1–266. [PubMed] [Google Scholar]
- 22.Fine LG, Norman JT. Chronic hypoxia as a mechanism of progression of chronic kidney diseases: from hypothesis to novel therapeutics. Kidney Int. 2008;74:867–72. doi: 10.1038/ki.2008.350. [DOI] [PubMed] [Google Scholar]
- 23.Fine LG, Orphanides C, Norman JT. Progressive renal disease: the chronic hypoxia hypothesis. Kidney Int Suppl. 1998;65:S74–8. [PubMed] [Google Scholar]
- 24.Ahmed SB, Ronksley PE, Hemmelgarn BR, et al. Nocturnal hypoxia and loss of kidney function. PLoS One. 2011;6:e19029. doi: 10.1371/journal.pone.0019029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Zoccali C, Benedetto FA, Mallamaci F, et al. Left ventricular hypertrophy and nocturnal hypoxemia in hemodialysis patients. J Hypertens. 2001;19:287–93. doi: 10.1097/00004872-200102000-00016. [DOI] [PubMed] [Google Scholar]
- 26.Zoccali C, Benedetto FA, Tripepi G, et al. Nocturnal hypoxemia, night-day arterial pressure changes and left ventricular geometry in dialysis patients. Kidney Int. 1998;53:1078–84. doi: 10.1111/j.1523-1755.1998.00853.x. [DOI] [PubMed] [Google Scholar]
- 27.Zoccali C, Mallamaci F, Tripepi G. Nocturnal hypoxemia predicts incident cardiovascular complications in dialysis patients. J Am Soc Nephrol. 2002;13:729–33. doi: 10.1681/ASN.V133729. [DOI] [PubMed] [Google Scholar]
- 28.Zoccali C, Mallamaci F, Tripepi G, Benedetto FA. Autonomic neuropathy is linked to nocturnal hypoxaemia and to concentric hypertrophy and remodelling in dialysis patients. Nephrol Dial Transplant. 2001;16:70–7. doi: 10.1093/ndt/16.1.70. [DOI] [PubMed] [Google Scholar]
- 29.Pressman MR, Benz RL, Schleifer CR, Peterson DD. Sleep disordered breathing in ESRD: acute beneficial effects of treatment with nasal continuous positive airway pressure. Kidney Int. 1993;43:1134–9. doi: 10.1038/ki.1993.159. [DOI] [PubMed] [Google Scholar]
- 30.Netzer NC, Stoohs RA, Netzer CM, Clark K, Strohl KP. Using the Berlin Questionnaire to identify patients at risk for the sleep apnea syndrome. Ann Intern Med. 1999;131:485–91. doi: 10.7326/0003-4819-131-7-199910050-00002. [DOI] [PubMed] [Google Scholar]
- 31.Flemons WW, Whitelaw WA, Brant R, Remmers JE. Likelihood ratios for a sleep apnea clinical prediction rule. Am J Respir Crit Care Med. 1994;150:1279–85. doi: 10.1164/ajrccm.150.5.7952553. [DOI] [PubMed] [Google Scholar]
- 32.Flemons WW. Clinical practice. Obstructive sleep apnea. N Engl J Med. 2002;347:498–504. doi: 10.1056/NEJMcp012849. [DOI] [PubMed] [Google Scholar]
- 33.Chung F, Yegneswaran B, Liao P, et al. STOP questionnaire: a tool to screen patients for obstructive sleep apnea. Anesthesiology. 2008;108:812–21. doi: 10.1097/ALN.0b013e31816d83e4. [DOI] [PubMed] [Google Scholar]
- 34.Levey AS, Coresh J, Balk E, et al. National Kidney Foundation practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Ann Intern Med. 2003;139:137–47. doi: 10.7326/0003-4819-139-2-200307150-00013. [DOI] [PubMed] [Google Scholar]
- 35.Levey AS, Stevens LA, Schmid CH, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150:604–12. doi: 10.7326/0003-4819-150-9-200905050-00006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Issa FG, Morrison D, Hadjuk E, Iyer A, Feroah T, Remmers JE. Digital monitoring of sleep-disordered breathing using snoring sound and arterial oxygen saturation. Am Rev Respir Dis. 1993;148:1023–9. doi: 10.1164/ajrccm/148.4_Pt_1.1023. [DOI] [PubMed] [Google Scholar]
- 37.Vazquez JC, Tsai WH, Flemons WW, et al. Automated analysis of digital oximetry in the diagnosis of obstructive sleep apnoea. Thorax. 2000;55:302–7. doi: 10.1136/thorax.55.4.302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Sabry AA, Abo-Zenah H, Wafa E, et al. Sleep disorders in hemodialysis patients. Saudi J Kidney Dis Transpl. 2010;21:300–5. [PubMed] [Google Scholar]
- 39.Araujo SM, de Bruin VM, Nepomuceno LA, et al. Restless legs syndrome in end-stage renal disease: Clinical characteristics and associated comorbidities. Sleep Med. 2010;11:785–90. doi: 10.1016/j.sleep.2010.02.011. [DOI] [PubMed] [Google Scholar]
- 40.Araujo SM, Bruin VM, Daher EF, Medeiros CA, Almeida GH, Bruin PF. Quality of sleep and day-time sleepiness in chronic hemodialysis: a study of 400 patients. Scand J Urol Nephrol. 2011;45:359–64. doi: 10.3109/00365599.2011.584694. [DOI] [PubMed] [Google Scholar]
- 41.Szentkiralyi A, Czira ME, Molnar MZ, et al. High risk of obstructive sleep apnea is a risk factor of death censored graft loss in kidney transplant recipients: an observational cohort study. Sleep Med. 2011;12:267–73. doi: 10.1016/j.sleep.2010.08.012. [DOI] [PubMed] [Google Scholar]
- 42.Silva GE, Vana KD, Goodwin JL, Sherrill DL, Quan SF. Identification of patients with sleep disordered breathing: comparing the four-variable screening tool, STOP, STOP-Bang, and Epworth Sleepiness Scales. J Clin Sleep Med. 2011;7:467–72. doi: 10.5664/JCSM.1308. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Gami AS, Pressman G, Caples SM, et al. Association of atrial fibrillation and obstructive sleep apnea. Circulation. 2004;110:364–7. doi: 10.1161/01.CIR.0000136587.68725.8E. [DOI] [PubMed] [Google Scholar]
- 44.Gus M, Goncalves SC, Martinez D, et al. Risk for obstructive sleep apnea by Berlin Questionnaire, but not daytime sleepiness, is associated with resistant hypertension: a case-control study. Am J Hypertens. 2008;21:832–5. doi: 10.1038/ajh.2008.184. [DOI] [PubMed] [Google Scholar]
- 45.Srijithesh PR, Shukla G, Srivastav A, Goyal V, Singh S, Behari M. Validity of the Berlin Questionnaire in identifying obstructive sleep apnea syndrome when administered to the informants of stroke patients. J Clin Neurosci. 2011;18:340–3. doi: 10.1016/j.jocn.2010.04.048. [DOI] [PubMed] [Google Scholar]
- 46.Drager LF, Genta PR, Pedrosa RP, et al. Characteristics and predictors of obstructive sleep apnea in patients with systemic hypertension. Am J Cardiol. 2010;105:1135–9. doi: 10.1016/j.amjcard.2009.12.017. [DOI] [PubMed] [Google Scholar]
- 47.Ahmadi N, Chung SA, Gibbs A, Shapiro CM. The Berlin questionnaire for sleep apnea in a sleep clinic population: relationship to polysomnographic measurement of respiratory disturbance. Sleep Breath. 2008;12:39–45. doi: 10.1007/s11325-007-0125-y. [DOI] [PubMed] [Google Scholar]
- 48.Sert Kuniyoshi FH, Zellmer MR, Calvin AD, et al. Diagnostic accuracy of the Berlin Questionnaire in detecting sleep-disordered breathing in patients with a recent myocardial infarction. Chest. 2011;140:1192–7. doi: 10.1378/chest.10-2625. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Hanly PJ, Gabor JY, Chan C, Pierratos A. Daytime sleepiness in patients with CRF: impact of nocturnal hemodialysis. Am J Kidney Dis. 2003;41:403–10. doi: 10.1053/ajkd.2003.50066. [DOI] [PubMed] [Google Scholar]
- 50.Parker KP, Bliwise DL, Bailey JL, Rye DB. Daytime sleepiness in stable hemodialysis patients. Am J Kidney Dis. 2003;41:394–402. doi: 10.1053/ajkd.2003.50049. [DOI] [PubMed] [Google Scholar]
- 51.Beecroft JM, Hoffstein V, Pierratos A, Chan CT, McFarlane PA, Hanly PJ. Pharyngeal narrowing in end-stage renal disease: implications for obstructive sleep apnoea. Eur Respir J. 2007;30:965–71. doi: 10.1183/09031936.00161906. [DOI] [PubMed] [Google Scholar]
- 52.Beecroft JM, Hoffstein V, Pierratos A, Chan CT, McFarlane P, Hanly PJ. Nocturnal haemodialysis increases pharyngeal size in patients with sleep apnoea and end-stage renal disease. Nephrol Dial Transplant. 2008;23:673–9. doi: 10.1093/ndt/gfm598. [DOI] [PubMed] [Google Scholar]
- 53.Tang SC, Lam B, Ku PP, et al. Alleviation of sleep apnea in patients with chronic renal failure by nocturnal cycler-assisted peritoneal dialysis compared with conventional continuous ambulatory peritoneal dialysis. J Am Soc Nephrol. 2006;17:2607–16. doi: 10.1681/ASN.2005090936. [DOI] [PubMed] [Google Scholar]
- 54.Tang SC, Lam B, Lai AS, et al. Improvement in sleep apnea during nocturnal peritoneal dialysis is associated with reduced airway congestion and better uremic clearance. Clin J Am Soc Nephrol. 2009;4:410–8. doi: 10.2215/CJN.03520708. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Stevens LA, Viswanathan G, Weiner DE. Chronic kidney disease and end-stage renal disease in the elderly population: current prevalence, future projections, and clinical significance. Adv Chronic Kidney Dis. 2010;17:293–301. doi: 10.1053/j.ackd.2010.03.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Lash JP, Go AS, Appel LJ, et al. Chronic Renal Insufficiency Cohort (CRIC) Study: baseline characteristics and associations with kidney function. Clin J Am Soc Nephrol. 2009;4:1302–11. doi: 10.2215/CJN.00070109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Hemmelgarn BR, Manns BJ, Quan H, Ghali WA. Adapting the Charlson Comorbidity Index for use in patients with ESRD. Am J Kidney Dis. 2003;42:125–32. doi: 10.1016/s0272-6386(03)00415-3. [DOI] [PubMed] [Google Scholar]