

Abstract
Background:
The morbidity and mortality of asthma have risen among children, especially those under 18, during the past 3 to 4 decades. There are various single studies in different target populations of Iran, which have reported different estimations. The present study designed in order to estimate a pooled prevalence among Iranian guidance school children.
Materials and Methods:
After searching for relevant articles in international and local databases from 1997 to 2009, we found 16 relevant articles and studies having the inclusion criteria. The outcome measure was the prevalence of asthma, and forest plot was used for presenting the findings of the meta-analysis. Heterogeneity between the studies was evaluated by the Cochran test. Moreover, the random effects model was used for estimation of pooled measures in Stata software (version 10).
Results:
From all the entered studies, 10 articles were published in English and the rest in Persian language. The pooled estimates for females, males and both genders were calculated as 3.9% (95% CI: 3.2% - 4.6%), 5% (95% CI: 4.2% - 5.8%), and 4.4% (95% CI: 3.7% - 5.1%), respectively.
Conclusion:
The prevalence of asthma among Iranian children varied from 1.26% to 11.6%, which is possibly due to the difference in sex, ethnicity race, and socio-economic level of Iranian population. Also, the prevalence of asthma among Iranian guidance school children was lower in comparison to the other neighborhood countries.
Keywords: Asthma, children, ISSAC, Iran, meta analysis, prevalence
INTRODUCTION
The prevalence of allergic diseases has an upward trend in children, in the world. Among the wide spectrum of such diseases, asthma is the most common, dangerous, and life-threatening chronic disease.[1] The morbidity and mortality of asthma have risen in children during the past 3 to 4 decades.[1–4] However, some decreasing trends have been observed in developing countries with the number of asthma-related deaths declining in recent years.[2] Moreover, it has affected all age groups, especially those younger than 18 years old.[1]
The ISAAC program was a worldwide strategy for determination of the prevalence of asthma in developed as well as developing countries.[5] This program provides a simple and unique method for measuring asthma and allergic diseases in childhood, which is appropriate for any place and language.[6] It has also facilitated an estimation and comparison of the prevalence of asthma by using a standard questionnaire for data collection in both international and regional levels.[5] Phase one of the ISAAC was developed based on the considerable interest, for an estimation of the current prevalence and projection of future trend of asthma as well as other allergic diseases in western and developing countries.[6]
An increasing trend of prevalence of asthma started from the 1970s, and now, the worldwide prevalence of this disease has been estimated to be 4% to 7%.[7] The results of the first International Study of Asthma and Allergies in Childhood (ISAAC) showed that the prevalence of asthma symptoms in different countries varied from 1.6% to 36.8%,[1,5] but this is related to age, race, gender, and residency place.[1] There are many studies on an evaluation of asthma prevalence among Iranian children in different cities.[5,8–33] These studies show that the prevalence of asthma varied from 1%[22] to 9.8%[5] and 35.4%[12] in ISSAC and non-ISSAC questionnaire based surveys. Another meta-analysis study estimated the prevalence of asthma in Iranian primary school age children as 3.9%, which ranged from 3.2% to 4.7%.[34] Also, in some studies, these estimates were different regarding sex.[5,12]
Meta-analysis is a method, which increases the power and precision of single studies by raising the sample size.[35] An application of meta-analysis for combining the results of observational studies gives a reference estimate, which is appropriate for health professionals as well as for policy makers.[36,37] Therefore, concerning the variety of studies conducted on different target populations with a considerable heterogeneity, the present study aims to estimate an overall prevalence of asthma in Iranian guidance school children. [Figure 1]
Figure 1.
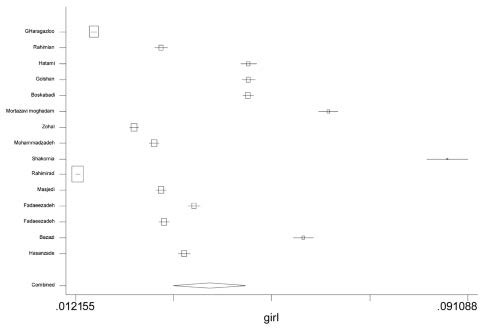
Forest plot of Asthma prevalence in Iranian female children
MATERIALS AND METHODS
We searched for relevant articles in international databases, including Medline, Pub-med, ISI, Google Scholar, and Scopus, and local databases such as, Scientific Information Database (SID), Iranmedex, and Irandoc, from 1997 to 2009. The key words of the research were asthma, prevalence, children, Iran, and ISSAC. After fulfilling a complete search, 63 related articles were founded. Reference lists of the searched articles were reviewed to identify additional eligible studies, as well. The inclusion criteria were utilizing the ISSAC questionnaire as the data collection instrument, a sample size equal to at least 1000 individuals, and guidance school children as the target population. These criteria were selected based on the recommendations of ISSAC program.[6] It is suggested that a 3000-subject sample size is required for an estimation of severe asthma, but based on the population size, and limited resources as well as equipments of the research, it could decline to a 1000-subject one. Some studies, which had not reported the total prevalence of asthma, were excluded from the study. Therefore, the studies without the qualification criteria, such as the ones published in two languages or double report in congresses or journals, were excluded from the study.
In the second stage, all the articles found were reviewed by two reviewers independently based on both inclusion and exclusion criteria. In this stage, we read and summarized favorable studies, and finally 16 relevant articles were selected and applied in the analyzes. It should be noted that we recalculated the prevalence in one study.[11] Also, regarding a study, which had been published 3 times,[23–25] we used the results of the one which was more comprehensive compared to the others.[23]
An outcome measure was the prevalence of asthma, reported in the studies based on the question “ever asthma”. The standard error of prevalence was calculated by binomial probability distribution. In addition, the heterogeneity between the studies was evaluated by the Cochran test. Moreover, random effect model with DerSimonian-Laird method was used for estimation of pooled measures, which calculates the pooled estimate and confidence interval, based on the weighted least square (weighting is given by the reciprocal sum of between and within study variances).[38] Publication bias was appraised by funnel plot and Begg as well as egger regression tests. All the analyzes were performed through the Stata software (version 10). In addition, the significant level for the Cochran test was considered as 0.05.
RESULTS
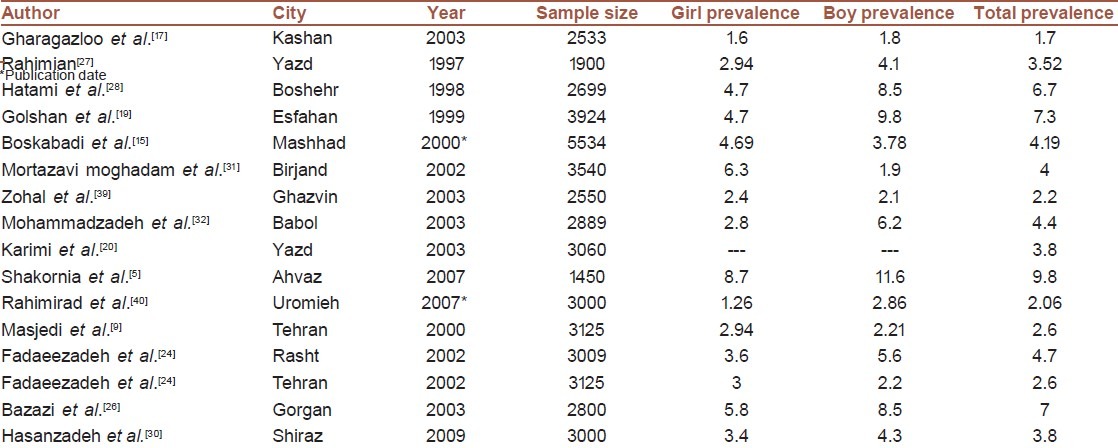
From the 63 studies which were found, 16 were relevant and had been published. From the 16 published articles, 10 were published in English and the rest in Persian. 10 study subjects (62.5%) were between 13 and 14 years old, while the age of the participants in other studies varied from 11 to 16 years old. Table 1 shows the details of the study subjects based on the total prevalence of asthma, regarding sex, and sample sizes.
Table 1.
Characteristics of single studies included in the Meta analysis
15 studies were used in the calculation of the pooled estimate for males and females, while 16 studies were utilized for the overall estimation. Fig 1 shows the pooled estimate of the females. It is obvious that the prevalence of asthma varied from 1.26% to 8.7% in the study subjects, and the pooled estimate was equal to 3.9% (95% CI: 3.2% - 4.6%). The range of the prevalence of asthma and the pooled estimate of the males are presented in Fig 2. The range of the prevalence of the disease between studies in males was wider than that of the females and varied from 1.8% to 11.6%. The pooled estimate was calculated as 5% (95% CI: 4.2% - 5.8%). Also, the total prevalence of asthma among the Iranian guidance school children can be observed in Fig 3, varying from 1.7% to 9.8%. Moreover, the pooled estimate of the meta-analysis was equal to 4.4% (95% CI: 3.7% - 5.1%).
Figure 2.
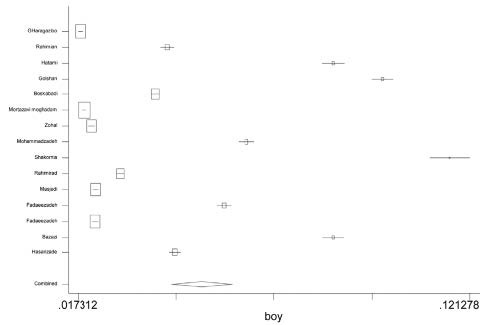
Forest plot of Asthma prevalence in Iranian male children
Figure 3.
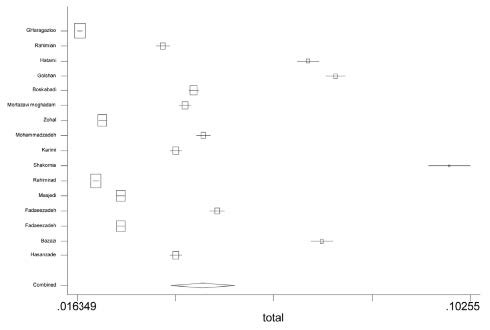
Forest plot of Asthma prevalence in Iranian guidance school children
DISCUSSION
The overall pooled estimate among the Iranian guidance-school children is equal to 4.4%, whose confidence interval changes from 3.7% to 5.1% in different places. The pooled prevalence estimate was higher in males, comparison to females. In another systematic review, conducted on Iranian people younger than 18 in 2003, the pooled estimate was equal to 13.14% (95% CI: 9.97 - 16.30%).[16] This difference is due to investigating the prevalence, based on “history of wheezing in the past 12 months” replaced by “ever asthma”.[11,15,19,39] Also, Entezari's study[16] reported that, all the single studies have been conducted based on the ISSAC protocol; however, one of the studies did not have this criterion.[10] This study reported the prevalence as 39.5%, which highly affects the pooled estimate. However, ascertainment methods and case definitions could change the asthmatic patients as well as the prevalence of asthma in different observational researches.[41] In order to decrease the controversies among the studies, based on different case definitions, such as parental reports of past asthma diagnosis, history of wheezing, asthma medication use, and documentation of asthma diagnoses as well as medication in the medical chart, in the present study, only single studies, which applied the ISSAC instrument for data collection, were used.
In another study, conducted on Asian and European primary school children in Southampton,[42] it was found that the number of children with “diagnosed as asthma” was 6.2%. Although the study participants were migrants, they were from a wide range of Asian countries and were comparable with our subjects. This implies that the prevalence of asthma in Iranian children was less than the Asian children.
Pal et al. conducted a systematic review and meta-analysis on Indian children by using 15 relevant articles, selected among 300 published articles and scientific meetings from 1966 to 2008. They estimated the mean prevalence and overall weighted mean prevalence to be equal to 7.24% and 2.74%, respectively. In addition, in comparison to 6-7 years old children, the prevalence of childhood asthma was less among the 13-14 years old ones.[7] The ISSAC screening committee study also reported the prevalence of asthma in Eastern Mediterranean region countries, such as Kuwait (17.5%), Lebanon – Beirut city (11.6%), Oman- Al-Khod city (20.7%), and Pakistan-Karachi city (7.3%).[6] Therefore, the overall prevalence of asthma in Iranian children is founded to be lower compared to the neighborhood countries’ children because the upper limit of the pooled estimate is lower than the estimated prevalence of these countries.
The results of a systematic review on 48 single full studies since 1990 to 2008 showed no evidence of declining asthma prevalence in the international trend of the disease in adults and children; however, in this review, a gap was observed in the literature in Africa as well as in some parts of Asia.[43] Therefore, any reduction in health care and health utilization might have undesirable results related to the future of the disease.
According to our results, the prevalence of asthma varied from 1.26 to 11.6 in Iranian children. Because of the different socio-economic and geographic factors, sex, ethnicity, and race of Iranian population, we observed heterogeneity among the studies. In order to reduce the within sex heterogeneity variance, the data were separately analyzed, based on sex.
Although we searched all the published and non-published studies to remove the publication bias, the funnel plot had an asymmetric shape. However, it may be a sign of publication bias. In addition, it should be noted that the funnel plot is useful in case there is a wide range of studies with different sample sizes.[38] Moreover, regarding the ISSAC recommendations, only the studies with larger than 1000 sample sizes were included in the present study.[6] Also, it should be emphasized that a skewed funnel plot may be created by factors other than the publication bias. For example, it has been shown that if the quality of the studies varies with the study size, a funnel plot may give the visual impression of publication bias while it is really confounded by the study quality. Also, differences in the underlying risk among the population of the primary studies and chance are other factors, which can cause the skewed funnel plot.[38] However, we assumed that difference in the underlying risk among the studies populations causes the skew of funnel plot.
Nevertheless, the studies which had been conducted on the 6-7 year old children were excluded from the present study because the children's age was a source of heterogeneity, especially in children's asthma, and at the same time, ISSAC designed two different questionnaires for the two age groups. Therefore, a limitation of the current study can be the fact that it cannot estimate the pooled estimate for all the Iranian children.
The results of this study showed that the prevalence of asthma in Iranian children ranges from 1.26 to 11.6. It is possibly due to different socio-economic and geographic factors, sex, ethnicity, and race of Iranian population. However, the overall prevalence of asthma in Iranian children is founded to be lower than the children in neighborhood countries.
ACKNOWLEDGMENT
We would like to thank all single studies’ authors that helped us collect the data and have access to full texts of their articles. Research improvement Center of Shiraz University of Medical Sciences and Ms. Afsaneh Keivanshekouh are also appreciated for improving the use of English in the manuscript. This project was conducted with personal budget and has not any conflict of interest.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Kudzyte J, Griska E, Bojarskas J. Time trends in the prevalence of asthma and allergy among 6-7-year-old children. Results from ISAAC phase I and III studies in Kaunas, Lithuania. Medicina (Kaunas) 2008;44:944–52. [PubMed] [Google Scholar]
- 2.Smyth RL. Asthma: A major pediatric health issue. Respir Res. 2002;3:S3–7. doi: 10.1186/rr188. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Carter ER, Debley JS, Redding GJ. Changes in asthma prevalence and impact on health and function in Seattle middle-school children: 1995 vs 2003. Ann Allergy Asthma Immunol. 2005;94:634–9. doi: 10.1016/S1081-1206(10)61320-8. [DOI] [PubMed] [Google Scholar]
- 4.Gessner BD, Neeno T. Trends in asthma prevalence, hospitalization risk, and inhaled corticosteroid use among Alaska Native and nonnative Medicaid recipients younger than 20 years. Ann Allergy Asthma Immunol. 2005;94:372–9. doi: 10.1016/S1081-1206(10)60990-8. [DOI] [PubMed] [Google Scholar]
- 5.Shakurnia AH, Assar S, Afra M, Latifi M. Prevalence of asthma among schoolchildren in Ahvaz, Islamic Republic of Iran. East Mediterr Health J. 2010;16:651–6. [PubMed] [Google Scholar]
- 6.The International Study of Asthma and Allergies in Childhood (ISAAC) Screening Committee. Worldwide variations in the prevalence of asthma symptoms: the International Study of Asthma and Allergies in Childhood (ISAAC) Eur Respir J. 1998;12:315–35. doi: 10.1183/09031936.98.12020315. [DOI] [PubMed] [Google Scholar]
- 7.Pal R, Dahal S, Pal S. Prevalence of bronchial asthma in Indian children. Indian J Community Med. 2009;34:310–6. doi: 10.4103/0970-0218.58389. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Bidad K, Anari S, Aghamohammadi A, Pourpak Z, Moayeri H. Prevalence of asthma related to BMI in adolescents in Tehran, Iran, 2004-2005. Eur J Pediatr. 2007;166:453–4. doi: 10.1007/s00431-006-0259-0. [DOI] [PubMed] [Google Scholar]
- 9.Ziaee V, Yousefi A, Movahedi M, Mehrkhani F, Noorian R. The prevalence of exercise-induced bronchospasm in soccer player children, ages 7 to 16 years. Iran J Allergy Asthma Immunol. 2007;6:33–6. [PubMed] [Google Scholar]
- 10.Mirsaeid Ghazi B, Sharifi SH, Goodarzipoor K, Aghamohammadi A, Atarod L, Rezaei N, et al. The Prevalence of Asthma among the Students (7-18 Years Old) in Tehran during 2002-2003. Iran J Allergy Asthma Immunol. 2004;3:89–92. [PubMed] [Google Scholar]
- 11.Masjedi MR, Fadaizadeh L, Najafizadeh K, Dokouhaki P. Prevalence and Severity of Asthma Symptoms in Children of Tehran- International Study of Asthma and Allergies in Childhood (ISAAC) Iran J Allergy Asthma Immunol. 2004;3:25–30. [PubMed] [Google Scholar]
- 12.Mirsaid Ghazi B, Imamzadehgan R, Aghamohammadi A, Darakhshan Davari R, Rezaei N. Frequency of Allergic Rhinitis in School-age Children (7-18 Years) in Tehran. Iran J Allergy Asthma Immunol. 2003;2:181–4. [PubMed] [Google Scholar]
- 13.Miri S, Farid R, Akbari H, Amin R. Prevalence of allergic rhinitis and nasal smear eosinophilia in 11- to 15 yr-old children in Shiraz. Pediatr Allergy Immunol. 2006;17:519–23. doi: 10.1111/j.1399-3038.2006.00424.x. [DOI] [PubMed] [Google Scholar]
- 14.Hedayati MT, Mayahi S, Denning DW. A study on Aspergillus species in houses of asthmatic patients from Sari City, Iran and a brief review of the health effects of exposure to indoor Aspergillus. Environ Monit Assess. 2010;168:481–7. doi: 10.1007/s10661-009-1128-x. [DOI] [PubMed] [Google Scholar]
- 15.Boskabady MH, Kolahdoz GH. Prevalence of asthma symptoms among the adult population in the city of Mashhad (north-east of Iran) Respirology. 2002;7:267–72. doi: 10.1046/j.1440-1843.2002.00398.x. [DOI] [PubMed] [Google Scholar]
- 16.Entezari A, Mehrabi Y, Varesvazirian M, Pourpak Z, Moin M. A systematic review of recent asthma symptom surveys in Iranian children. Chron Respir Dis. 2009;6:109–14. doi: 10.1177/1479972309103884. [DOI] [PubMed] [Google Scholar]
- 17.Gharagozlou M, Khalili S, Hallajmofrad M, Mohammadzadeh R, Mousavi G, Golkari H. Gender similarity in low agreement between written and video ISAAC asthma questionnaires. Monaldi Arch Chest Dis. 2006;65:184–8. doi: 10.4081/monaldi.2006.547. [DOI] [PubMed] [Google Scholar]
- 18.Golshan M, Mohamad-Zadeh Z, Zahedi-Nejad N, Rostam-Poor B. Prevalence of asthma and related symptoms in primary school children of Isfahan, Iran, in 1998. Asian Pac J Allergy Immunol. 2001;19:163–70. [PubMed] [Google Scholar]
- 19.Golshan M, Mohammad-Zadeh Z, Khanlar-Pour A, Iran-Pour R. Prevalence of asthma and related symptoms in junior high school children in Isfahan, Iran. Monaldi Arch Chest Dis. 2002;57:19–24. [PubMed] [Google Scholar]
- 20.Karimi M, Mirzaei M, Ahmadiah MH. Prevalence of Asthma, Allergic Rhinitis and Eczema Symptoms among 13-14 Year-old School Children in Yazd in 2003. Scientific Medical Journal of Ahwaz University of Medical Sciences. 2007;6:270–5. [Google Scholar]
- 21.Ahmadiafshar A, Parchegani MR, Moosavinasab N, Koosha A. A Study of Relation between BCG Scar and Atopy in Schoolchildren of Zanjan City. Iran J Allergy Asthma Immunol. 2005;4:185–8. [PubMed] [Google Scholar]
- 22.Hedayatmofidi SM, Ahmadi A, Baeleh MT, Bakhsha F, Joshaghani HR. Prevalence of asthma in school children in gorgan, Iran by questionnaire survey 2006. J Med Sci. 2007;7:1054–56. [Google Scholar]
- 23.Najafizadeh K, Fadaizadeh L, Salek S. Prevalence and Severity of Asthmatic Symptoms in Rasht Students: A Report from ISAAC Study. Tanaffos. 2008;7:40–6. [Google Scholar]
- 24.Fadaizadeh L, Salek, Najafizadeh K, Masjedi MR. Prevalence and Severity of Asthma Symptoms in Students of Tehran and Rasht: Phase III ISAAC Study. Tanaffos. 2008;7:31–6. [Google Scholar]
- 25.Ranjbar ZA. Prevalence of asthma symptoms in children. Journal Guilan Univ Med Sci. 2006;14(56):9–1. [Google Scholar]
- 26.BazaziI H, Gharagozlou M, Kassai M, Zahmatkesh H, Parsikia A. The prevalence of asthma and allergic disorders among school children on Gorgan. J Res Med Sci. 2007;12:28–33. [Google Scholar]
- 27.Rahimian M. Prevalence of current Asthma in middle-school students in Yazd city. J Shahid Sadoghi Univ Med Sci. 1999;6:19–22. [Google Scholar]
- 28.Hatami G, Amir Azodi E, Najafi A, Razavi SH, Afrasiabi K, Afarid M, et al. Prevalence of Asthma and Asthma-related symptoms among 13-14 yr. schoolchildren in Bushehr, ISSAC. Iranian South Med J. 2003;2003:2. [Google Scholar]
- 29.Mortazavi Moghaddam, AR SJ. Prevalence of Asthma symptoms among 13-14 years old children in Birjand. J Zahedan Univ Med Sci (Tabib-e-shargh) 2004;6:183–91. [Google Scholar]
- 30.Hasanzadeh H, Basiri F, Mohammadbeigi A. Prevalence and severity of symptoms of asthma and allergic diseases with ISSAC method in guide school boys and girls, Shiraz 2009. Zahedan Journal of Research in Medical Sciences, J Zahedan Univ Med Sci. 2012;13:35–9. [Google Scholar]
- 31.Mortazavi Moghaddam SGh.R, Akbari H, AR S. Asthma in Iranian Schoolchildren: Comparison of ISAAC Video and Written Questionnaires. Iran J Med Sci. 2005;30:110–4. [Google Scholar]
- 32.Mohammadzadeh I, Ghafari J, Barari Savadkoohi R, Tamaddoni A, Esmaeili Dooki MR, Alizadeh Navaei R. The Prevalence of Asthma, Allergic Rhinitis and Eczema in North of Iran: The International Study of Asthma and Allergies in Childhood (ISAAC) Iran J Pediatr. 2008;18:117–22. [Google Scholar]
- 33.Rahimirad MH, Hejazi ME. Agreement between written and video asthma symptoms questionnaires in school children in Urmia, Iran. Iran J Allergy Asthma Immunol. 2007;6:21–5. [PubMed] [Google Scholar]
- 34.Mohammadbeigi A, Hassanzadeh J, Mousavizadeh A. Prevalence of asthma in elementary school age children in Iran, A systematic review and Meta-analysis. Pak J Bio Sci. 2011;14:887–93. doi: 10.3923/pjbs.2011.887.893. [DOI] [PubMed] [Google Scholar]
- 35.Cohn LD, Becker BJ. How meta-analysis increases statistical power. Psychol Methods. 2003;8:243–53. doi: 10.1037/1082-989X.8.3.243. [DOI] [PubMed] [Google Scholar]
- 36.Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D, et al. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA. 2000;283:2008–12. doi: 10.1001/jama.283.15.2008. [DOI] [PubMed] [Google Scholar]
- 37.Haghdoost AA, Sadeghirad B, Hajarizadeh B, Mirzazadeh A. The Application of Systematic Review and Meta-analysis Concepts in Summarizing the Findings of Observational Studies. Iran J Psychiatry. 2007;2:132–6. [Google Scholar]
- 38.Sutton AJ, Abrams KR, Jones DR, Sheldon TA, Song F. Methods for meta analysis in medical sciences. Ltd. England: John Wiley and Sons; 2000. [Google Scholar]
- 39.Zohal MA, HashemiNasab R. Prevalence of Asthma among school-age children in Qazvin, 2003. J Qazvin Univ Med Sci. 2006;9:64–8. [Google Scholar]
- 40.Rahimi Rad MH, Hejazi ME, Behrouzian R. Asthma and other allergic diseases in 13-14-year-old schoolchildren in Urmia, Iran. [corrected] East Mediterr Health J. 2007;13:1005–16. doi: 10.26719/2007.13.5.1005. [DOI] [PubMed] [Google Scholar]
- 41.Greenlee RT, Chyou PH, Kieke A, Naik YG, Kirkhorn S. Prevalence of asthma in a general population cohort of farm children: Comparison of estimates based on parental report and medical record review. J Agromedicine. 2008;13:225–31. doi: 10.1080/10599240802454593. [DOI] [PubMed] [Google Scholar]
- 42.Pararajasingam CD, Sittampalam L, Damani P, Pattemore PK, Holgate ST. Comparison of the prevalence of asthma among Asian and European children in Southampton. Thorax. 1992;47:529–32. doi: 10.1136/thx.47.7.529. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Anandan C, Nurmatov U, van Schayck OC, Sheikh A. Is the prevalence of asthma declining? Systematic review of epidemiological studies. Allergy. 2010;65:152–67. doi: 10.1111/j.1398-9995.2009.02244.x. [DOI] [PubMed] [Google Scholar]