

Abstract
Through archival analysis this article traces the emergence, maintenance, and enhancement of biogerontology as a scientific discipline in the United States. At first, biogerontologists' attempts to control human aging were regarded as a questionable pursuit due to: perceptions that their efforts were associated with the long history of charlatanic, anti-aging medical practices; the idea that anti-aging is a “forbidden science” ethically and scientifically; and the perception that the field was scientifically bereft of rigor and scientific innovation. The hard-fought establishment of the National Institute on Aging, scientific advancements in genetics and biotechnology, and consistent “boundary work” by scientists, have allowed biogerontology to flourish and gain substantial legitimacy with other scientists and funding agencies, and in the public imagination. In particular, research on genetics and aging has enhanced the stature and promise of the discipline by setting it on a research trajectory in which explanations of the aging process, rather than mere descriptions, have become a central focus. Moreover, if biogerontologists' efforts to control the processes of human aging are successful, this trajectory has profound implications for how we conceive of aging, and for the future of many of our social institutions.
Ambitions and attempts to control aging have been part of human culture since early civilizations (Gruman, 2003). An obsession with immortality is a central theme in a Babylonian legend about the king Gilgamesh who ruled southern Mesopotamia in about 3000 B.C. In the third century B.C., adherents of the Taoist religion in China developed a systematic program aimed at prolonging life (Olshansky & Carnes, 2001). Through the centuries, a variety of anti-aging approaches have recurred. Among them have been alchemy, the use of precious metals (e.g., as eating utensils) that have been transmuted from baser minerals; “shunamatism” or “gerocomy” (cavorting with young girls); grafts (or injected extracts) from the testicles, ovaries, or glands of various animal species; cell injections from the tissues of newborn or fetal animals; consumption of elixirs, ointments, drugs, hormones, dietary supplements, and specific foods; cryonics; and rejuvenation from devices and exposure to various substances such as mineral and thermal springs (Gruman, 2003; Hayflick, 1994).
Anti-aging aspirations and efforts flourish today, perhaps more than ever, in the forms of: (1) commercial and clinical enterprises that offer anti-aging products, regimens, and treatments; and (2) research and development efforts of biogerontologists – scientists who study the biology of aging. Indeed, anti-aging has been identified as one of the specific topics to be considered at the 19th World Congress of Gerontology and Geriatrics in Paris in 2009 (International Association of Gerontology and Geriatrics, 2007). Many biogerontologists also seek to achieve what historian Gerald Gruman (2003) has termed “prolongevity” – a significant extension of average human life expectancy and/or maximum life span without extending suffering and infirmity.
Although not universally true, one thing that characterizes both contemporary and previous anti-aging endeavors is their public perception as something simultaneously seductive and desirable yet also transgressive, suspicious, and even dangerous. As such, contemporary anti-aging research is a type of “forbidden knowledge” (Kempner, Perlis, & Merz, 2005) – an area of research that is, in some ways, considered off limits for various, often moralistic, reasons. However, the field of anti-aging research is not only tinged with questions about the moral transgressions of interfering with the “natural” process of aging, but it also has emerged from a tainted history where the science itself was considered marginal and without much merit. This history has conflated questions about whether we should pursue anti-aging interventions and whether we can control aging (Moody, 2001/2). Because of these questions, the field is still somewhat mired by its historically marginal and forbidden status, despite its recognition by large funding agencies and others as a now reputable and cutting-edge area of research.
At first, scientists' attempts to control human aging were regarded as a questionable pursuit due to: perceptions that their efforts were associated with the long history of charlatanic, anti-aging medical practices; the idea that anti-aging is a “forbidden science” ethically and scientifically; and the perception that the field was scientifically bereft of rigor and scientific innovation. The hard-fought establishment of the National Institutes on Aging, scientific advancements in genetics and biotechnology, and consistent “boundary work” by scientists, has allowed biogerontology to flourish and gain substantial legitimacy with other scientists and funding agencies, and in the public imagination. However, scientists in this field are vigilant about protecting the scientific status and credibility of biogerontology, which is still somewhat fragile.
This article traces the emergence, maintenance, and enhancement of biogerontology as a scientific discipline that is dedicated to understanding the biology of the aging process. Our data comes from secondary sources on the history of (bio)gerontology, primary materials documenting the establishment of the National Institute of Aging, and an exhaustive review of biogerontologists' publications on the history and state of the discipline. The archival analysis led us to consider theoretical insights from the social studies of science to describe biogerontologists' activities and intentions as they work to establish and bolster their legitimacy as scientists, and moreover as scientists worthy of research funding and public support. Using an inductive process, we toggled back and forth between data and theory to form our analysis of the emergence of biogerontology. At the end of the paper, we consider the significance of the emergence of biogerontology in shaping our cultural and scientific understanding of the aging process and its potential social implications for the future.
The emergence of biogerontology as a scientific discipline
The history of biomedical research on aging in the United States is a classic story of a new scientific discipline's struggle for legitimacy and funding. Scholars in the social studies of science have long been interested in the emergence of new scientific disciplines (Hedgecoe, 2003). The premise of this scholarship is that disciplinary building is a social, political, and cultural endeavor [see e.g. (Abir-Am, 1985; Bud, 1993; Gieryn, 1983)]. A new discipline may in fact develop around a new set of scientific discoveries, new methodologies, or new objects of inquiry. However, these scientific “facts” alone are not enough to constitute a new discipline. Individuals, groups, and institutions need to work towards legitimation within the larger scientific and social arena, through garnering political support, allying themselves with credible and respected scientists and other elite members of society, and convincing those around them (often through rhetorical strategies) that their discipline is indeed worthy of scientific inquiry (Abir-Am, 1985; Fujimura,1996; Hedgecoe, 2003; van Lente & Rip 1998). The history of biogerontology's emergence is one that follows this pattern as members in the field tried to establish their work as a legitimate scientific discipline. This story is particularly significant given the legacy of ill-repute that anti-aging/prolongevity efforts garnered in the many years prior to the establishment of the field. This perception of anti-aging research as not only scientifically inferior, but also as an area of “forbidden knowledge” (Kempner et al., 2005) made the fight to establish the discipline all the more difficult.
Once the discipline was established, biogerontologists sought (and still seek) to maintain and enhance the discipline. This requires work to preserve their hard hard-fought status through other claims-making activities – “boundary work” – wherein members of the new discipline attempt to distinguish themselves from other groups in the same social arena (Gieryn, 1983), particularly those with less credibility and stature than themselves. In the case of biogerontologists, their boundary work activities aim to do two things: 1) weaken the boundaries between themselves and genetic researchers in other areas of the biosciences and 2) strengthen the boundaries between themselves and anti-aging practitioners and entrepreneurs. Mere association with these latter groups was thought by biogerontologists to threaten their own scientific credibility, whereas association with genetic researchers was to bolster their professional standing and support for their research. This hard-won legitimacy, achieved in part through biogerontology's affiliation with genetics, shapes contemporary and future (anti-)aging research, setting it on a trajectory which highlights a molecular understanding of aging and its potential interventions.
Modern biogerontology: the early years
In his monograph on the history of ideas about “prolongevity” Gruman observed that the subject tends to be:
relegated to a limbo reserved for impractical projects or eccentric whims not quite worthy of serious scientific or philosophic consideration. One reason for this neglect is that there is, in philosophy, science, and religion, a long tradition of apologism, the belief that the prolongation of life is neither possible nor desirable… Another reason is the fact that there are few subjects which have been more misleading to the uncritical and more profitable to the unscrupulous; the exploitation of this topic by the sensational press and by medical quacks and charlatans is well known. (2003, pp. 6)
In her history of the development of U.S. governmental support for research on aging, published several decades ago, political scientist Betty Lockett (1983) observed: “Those who would study aging in order to retard or halt the process have been considered on the fringe of biomedical research, looking for the fountain of youth… a marginal area… with so little backing from the scientific community” (p. 5).
As Achenbaum (1995), Hayflick (1994), and Lockett (1983) detail, the early development of the modern research enterprise in the biology of aging in the United States, and in geriatrics as well, was to a significant degree stimulated by the Josiah Macy Foundation. During the late 1930s it supported surveys on aging and commissioned a seminal volume on Problems of Aging: Biological and Medical Aspects (Cowdry, 1939) that reviewed research knowledge and issues regarding how to prolong human life and how to reduce disabilities and chronic diseases in old age. The foundation also funded a series of professional conferences that brought together researchers from a variety of disciplines and professions who formed a Club for Research on Aging which eventually became the Gerontological Society of America.
In 1940, the U.S. Surgeon General, who had attended a meeting of the Club, took the lead in establishing a small intramural research program in gerontology under the auspices of the U.S. National Institutes of Health (NIH). However, despite the substantial growth in the broad field of gerontology over the next three decades, the development of the biomedical research enterprise in gerontology stagnated. The NIH intramural research program on aging barely got off the ground during World War II as it was diverted by research devoted to the war effort. In 1948 it was designated as the Gerontology Branch of the National Heart Institute, was given a line item budget, and conducted physiological research on elderly men.
Although an NIH Gerontological Study Section for reviewing extramural research applications was created in 1946, it was abolished three years later. In the 1950s and 1960s, extramural research on aging gained little ground at NIH. During this period, in response to pressures from Congress, five regional multidisciplinary centers for aging research and training were funded through NIH's program project mechanism. However, only one of these centers (at Duke University) ultimately survived, and an internal NIH evaluation of the work of these centers was pointedly uncomplimentary concerning the quality of their gerontological research (Lockett, 1983). Meanwhile, a Senate Subcommittee on Problems of the Aging and Aged issued a report “disparaging the quality of gerontologic research” (Achenbaum, 1995, p. 200).
When a National Institute of Child Health and Human Development (NICHD) was established in 1963, NIH programs on aging became part of NICHD's Adult Development and Aging Branch. Although the branch had an external peer review committee comprising a multidisciplinary roster of gerontological researchers, it only reviewed applications for program projects and training and career development grants, not research grants. Over the next ten years gerontologists expressed their disappointment with the NICHD arrangement, especially the low proportion of that institute's funds earmarked for research on aging (see, e.g., Eisdorfer, 1968).
The institutionalization of research on aging
By the late 1960s, frustrated by NIH's lack of funding for research on the basic mechanisms of aging, biogerontologists set in motion the forces that ultimately led to the establishment of a separate National Institute on Aging in order to ensure that earmarked funds for gerontological research would be adequate. They drafted a bill in 1968 that called for a new NIH Institute with a five-year research plan “to promote intensive coordinated research on the biological origins of aging” (Lockett, 1983, p. 85). In order to gain the support of the Gerontological Society of America, however, the bill was quickly broadened to include the medical, behavioral, and social sciences (Binstock, 2003).
During the subsequent political processes that finally led to the establishment of NIA in 1974, themes suggesting the marginal status of biogerontology persistently emerged. For example, the key political actor in the successful lobbying effort, Florence Mahoney, was an ardent pursuer of anti-aging interventions. She was very interested in rejuvenation therapies offered by an institute in Bucharest, Romania and accustomed to taking serum treatments that were purported to slow or prevent aging. Mahoney was also a powerful Washington “insider” with politically elite connections, a long-time behind-the-scenes effective advocate for expanded government support for biomedical research. As noted in her biography, however, Mahoney's “accuracy in separating real science from charletan [sic] science was not precise; she occasionally backed a rejuvenation expert who had mastered promotion and mystique” (Robinson 2001, p. 237). Because of Mahoney's personal interest in anti-aging interventions her crucial political support in establishing the NIA may have further aligned perceptions of biogerontologists' work with seemingly charlatanic medicine.
Throughout the protracted legislative history of NIA's establishment, from 1969 through 1974, various opponents of such an institute were quite candid regarding their negative view of the quality and promise of gerontological research. At a Senate hearing in 1971, for instance, an assistant secretary in the Department of Health, Education, and Welfare argued that the field of aging was not ripe for the injection of major new resources because it lacked “a substantial body of interested and competent research investigators, plus enough research leads, or promising ideas within the field to challenge the researchers to productive endeavors” (Lockett, 1983, p. 98). Similarly, in a House of Representatives hearing in 1972, the president of the Association of American Medical Colleges asserted that “there is a paucity of trained researchers and valid ideas in the field of aging research” (Lockett, 1983, p. 22). And when one version of the bill passed in 1972, a memo from the Office of Management and Budget to President Nixon urged him to veto it – which he ultimately did – because an NIA “could raise false expectations that the aging process can somehow be controlled and managed through biomedical research” (Lockett, 1983, p. 139). Despite Nixon's veto – and consistent opposition from high-level NIH officials who apparently did not want to have a new institute carving out its own share of NIH appropriations (Lockett, 1983; U.S. Senate Subcommittee on Aging, 1973) – Mahoney, a cadre of gerontologists, and several key members of Congress persisted in their efforts. In 1974, in the midst of calls for his impeachment, Nixon signed the legislation creating NIA (Research on Aging Act of 1974, 1974).
The establishment of NIA provided for biogerontology the kind of institutionalization that confers scientific stature and power (Cozzens, 1990). It began a process that legitimated research on aging both as more of a “mainstream” subject for biomedical research than the broader scientific community had regarded it, and as an appropriate area in which to invest sizeable amounts of public funds. Since NIA began operation, a number of important scientific frontiers have been opened up in research on the fundamental biological process of aging (see Masoro & Austad, 2006). Moreover, the overall NIA budget, which was only about $20 million in its first year of operation (Lockett, 1983), grew substantially during the next 30 years to reach over $1 billion by fiscal year 2007 (National Institute on Aging, 2007).
Although there are, of course, a number of distinguished European biogerontologists, nothing comparable to the NIA has been established in Europe. Some of them look to the U.S. NIA for research support and often succeed. But, as Warner (2007) reports, other than in Belgium and Denmark there have been no sustained initiatives by European governments or the European Union to fund biogerontological research on aging.
The struggle to maintain legitimacy and status
Parallel to the modern emergence of biogerontology as a scientific discipline has been the development of anti-aging medicine. Mykytyn (2006a) characterizes anti-aging medicine as a social movement in the sense that it involves a group of people bound together under a particular mission in opposition to the “mainstream” with, in this instance, mainstream referring primarily to both mainstream biogerontology and clinical medicine.
However, unlike other health social movements which are often characterized by a resistance to biomedicine from those outside of it – e.g., patients, activists, grassroots organizations (see e.g., Epstein, 1996; Brown & Zavetoski 2004; Landzelius, 2006) – the anti-aging medicine social movement has its roots in large part from within biomedicine, if perhaps a marginal wing of biomedicine. Aging, a cluster of human conditions and experiences previously considered to be nonpathological, has become medicalized like many other features of the human condition (Clarke, Shim, Mamo, Fosket, & Fishman, 2003). This phenomenon has been specifically noted in the field of gerontology as the “biomedicalization of aging” (Estes & Binney, 1989) and chronicled with respect to the sociopolitical transformation of cognitive senility into Alzheimer's disease (Fox, 1989).
At the same time, contemporary interest in anti-aging medicine is fueled by the promises and predictions of cutting-edge biomedical and scientific research, such as stem cell research, nanotechnology, and gene therapy (Mykytyn, 2006b). Anti-aging medicine is thought to be feasible because of its reliance on the rhetoric of scientific breakthroughs. Biogerontologists, too, have benefited from the promises of cutting-edge biotechnology and have thereby made a number of recent scientific discoveries that seemingly have relevance for breakthroughs in slowing the rate of aging in human beings (see Masoro & Austad, 2006). As we will document, it is the promise of biotechnological advances that is at the heart of the boundary work in which biogerontologists engage. On one hand, they attempt to downplay their relationship with anti-aging medicine and extravagant anti-aging claims. On the other hand, they work to codify their relationship with biotechnology research in order to maintain their still fragile scientific status as a discipline.
The modern anti-aging movement
The modern anti-aging medicine movement was spear-headed in the 1960s and 1970s in Europe. A Romanian biologist and physician, Anna Aslan, established an institute in Bucharest that offered rejuvenation therapies and an elixir called Gerovital (Robinson, 2001) which is still widely marketed. Members of the European and Asian elite, including Nikita Kruschev, visited the institute for treatments, and the Soviet Union established its own institute to study Gerovital and other potential anti-aging interventions. Today, a substantial German-speaking anti-aging movement is headed by Johannes Huber, an Austrian scientist, physician, and theologian who develops, applies, and sells hormone treatments, dietary supplements, and predictive gene testing (Spindler in this issue). And various academies and centers on anti-aging medicine can also be found in France, Belgium, and Japan, along with European-wide and Asian/Pacific organizations of this ilk (Robert, 2004).
At the same time that Gerovital was marketed throughout Europe, Geritol — a similar product — was aggressively marketed in the United States. Although there has always been strong interest in anti-aging products, it was not until several decades later that the market really took off. The use of anti-aging products, particularly dietary supplements, soared especially in the years following the enactment of the Dietary Supplement Health and Education Act of 1994 which relaxed regulation of such products (U.S. GAO, 2001). From the late 1990s to the present day, hundreds of popular anti-aging books have been published, such as You: Staying Young: The Owner's Manual for Extending Your Warranty (Roizen & Oz, 2007). The authors, prominent physicians in the United States, often appear on the Oprah television show and their book was the 23rd bestselling book on Amazon. com's website within three months of its release (Amazon. com, 2008). A refereed scientific publication, the Journal of Anti-Aging Medicine (subsequently renamed Rejuvenation Research), began publishing in 1998 and several non-refereed publications with similar sounding names also appeared. Hundreds of websites like “Youngevity: The Anti-Aging Company” have marketed products such as “The Vilcabamba Mineral Essence” to enable people to live their lives “in a state of youthfulness” (Youngevity, 2003).
There are no hard statistics on the size of the overall anti-aging market in the United States but some estimates are available. A research report prepared by the Business Communications Company, Inc. (2005) estimates that the anti-aging market in the United States alone will reach about $72 billion by 2009. It defines the market in terms of three categories (excluding exercise and physical therapy): appearance products and services; drugs and supplements targeting diseases of aging; and products based on “advanced technologies.” Whatever the magnitude of the market, it seems highly likely to grow further given the intensity and prevalence of mass-marketing advertising campaigns.
One particular element of the anti-aging movement that has directly challenged the established gerontological community is the American Academy of Anti-Aging Medicine (A4M) which despite its name, is international in scope. Founded in 1993, the organization claims it has 20,000 members from 90 countries (Klatz, 2007). The latest publicly available income tax returns show that it had accumulated net assets of $5.9 million by 2005 and had $2 million in income that year (Guidestar, 2007).
Although A4M is not recognized by the American Medical Association or the American Board of Medical Specialties, it has established certification programs under its auspices for physicians, chiropractors, dentists, naturopaths, podiatrists, pharmacists, registered nurses, nurse practitioners, physician assistants, nutritionists, dieticians, sports trainers and fitness consultants, and “medical spa facilities” (A4M, 2008). The organization puts on three annual anti-aging conferences in the United States, as well as conferences in nations throughout the world. Its first “World Congress” of anti-aging medicine outside the United States was held in Paris in 2003 in partnership with French, German, Japanese, European, and Asian-Pacific anti-aging societies and organizations (Robert, 2004). In fact, in 2008 alone, the A4M scheduled 12 conferences in nine different countries. A4M's conferences have been so financially successful that in 2007 the organization sold an 80% stake in its conference business for $49 million to a London-based international media firm, Tarsus Group (Wilson, 2007).
A4M states that it does not sell or endorse any commercial product or promote or endorse any specific treatment. But it actively solicits and displays numerous advertisements on its website for products and services (such as cosmetics, alternative medicines and therapies), anti-aging clinics, pharmacies, and anti-aging physicians and practitioners, most of them listing certification by A4M.
What A4M terms “the traditional, antiquated gerontological establishment” (Arumainathan, 2001) may disagree with many of the organization's messages and the measures it promotes. Yet, most elements of A4M's broadly-stated goals are basically the same as those of many biomedical researchers and practitioners in gerontology and geriatrics, as we will demonstrate later in this article. The stated mission of A4M is:
the advancement of technology to detect, prevent, and treat aging related disease and to promote research into methods to retard and optimize the human aging process…. A4M believes that the disabilities associated with normal aging are caused by physiological dysfunction which in many cases are ameliorable [sic] to medical treatment, such that the human life span can be increased, and the quality of one's life improved as one grows chronologically older (A4M, 2005)
This A4M mission is, in fact, very similar to a portion of NIA's mission. For instance, an important research goal in an official NIA strategic plan is “Unlocking the Secrets of Aging, Health and Longevity”; the plan declares that “The ultimate goal of this effort is to develop interventions to reduce or delay age-related degenerative processes in humans” (National Institute on Aging, 2001).
Boundary work
The growth and popularity of the anti-aging medicine social movement in recent years has provoked biogerontologists to distinguish themselves from it, in order to preserve their hard-won scientific and political legitimacy, as well as to maintain and enhance funding for their research. The efforts of biogerontologists to differentiate themselves from the anti-aging movement are a classic example of what Gieryn (1983) termed “boundary work,” paralleling disputes in many other areas of science in which rhetorical demarcations are employed to maintain legitimacy and power. As Taylor (1996, p. 5) observes, “Practicing scientists, consciously or otherwise, discursively construct working definitions of science that function, for example, to exclude various non- or pseudo-sciences so as to sustain their (perhaps well-earned) position of epistemic authority and to maintain a variety of professional resources.” Such is the case with individual biogerontologists, and with the discipline collectively.
The boundary work engaged in by biogerontologists has been highly evident in public documents in recent years. A notable example was a lengthy position statement endorsed by an international roster of 51 gerontological scientists in 2002, summarized in an article in a popular magazine, Scientific American, under the title “No Truth to the Fountain of Youth.” The article declared that,
The hawking of anti-aging “therapies” has taken a particularly troubling turn of late. Disturbingly large numbers of entrepreneurs are luring gullible and frequently desperate customers of all ages to “longevity” clinics, claiming a scientific basis for the anti-aging products they recommend and, often, sell. At the same time, the Internet has enabled those who seek lucre from supposed anti-aging products to reach new consumers with ease. (Olshansky, Hayflick, & Carnes, 2002a, p. 92)
It went on to assert that “no currently marketed intervention — none — has yet been proved to slow, stop, or reverse human aging, and some can be downright dangerous” (pp. 92–93).
Shortly after the article appeared, the full position statement was also posted online at a website of the American Association for the Advancement of Science and the journal Science. It was then reprinted in the Journal of Gerontology: Biological Sciences (Olshansky, Hayflick, & Carnes, 2002b) and arrangements were made to have it published (in translation) in Chinese, French, German, Korean, and Spanish journals. The scientists' message also reached a very large audience when the AARP Bulletin, with a circulation of more than 35 million, made the Scientific American article the lead story in its next issue (Pope, 2002).
The internationally-endorsed position statement was the most publicized but not the only effort to distance the field of gerontological science from anti-aging medicine. Although different types of strategies have been employed in these efforts, one common goal has been to ensure that the hard hard-won respectability attained by the community of biogerontological researchers not be tainted by the anti-aging movement. As the position statement acknowledges, “Our concern is that when proponents of anti-aging medicine claim that the fountain of youth has already been discovered, it negatively affects the credibility of serious scientific research efforts on aging” (Olshansky et al., 2002b, p. B295).
One approach has been to discredit the anti-aging medicine movement by disparaging it for making a “quick profit” by fraudulently “exploiting the ignorance and gullibility of the public” (Hayflick 2001/2, p. 25). To this end, the organizers of the position statement constituted themselves as a committee to designate annual “Silver Fleece Awards” (in the form of bottles of salad oil, labeled “Snake Oil”) in “a lighthearted attempt to make the public aware of the anti-aging quackery that has become so widespread here and abroad” (University of Illinois at Chicago, 2002). The first Silver Fleece Award for an Anti-Aging Organization, in 2002, was presented in absentia to A4M, which was characterized “as responsible for leading the lay public and some in the medical and scientific community to the mistaken belief that technologies already exist that stop or reverse human aging.”
A second and more subtle rhetorical approach has been to mobilize the adjective “legitimate” to modify research on aging and thereby distinguish it from the anti-aging movement. As biogerontologist Richard Miller explains, “Scientists and their patrons — even those who have legitimate research interests in interventional gerontology — do not wish to be seen hanging out with snake-oil vendors (Miller, 2002, p. 167, emphasis added). Thus, the newsletter of the International Longevity Center, headed by the founding director of NIA, declares, “Legitimate aging research is particularly important due to the prevalence of `anti-aging therapies' therapies' being peddled in the marketplace that are not based on any scientific evidence and could possibly be dangerous” (Nyberg, 2002, p.1, emphasis added). The international position statement signed by the 51 scientists also presents this contrast: “The misleading marketing and the public acceptance of anti-aging medicine is not only a waste of health dollars; it has also made it far more difficult to inform the public about legitimate scientific research on aging and disease” (Olshansky, et al., 2002b, p. B293, emphasis added).
Genetic discoveries and scientific status
As a group of 28 self-described “representative mainstream biogerontologists” observed in a 2005 article, “Aging research is a discipline just now emerging from a reputation for charlatanry” (Warner et al., 2005, p. 1007). The boundary work of biogerontologists against the anti-aging social movement has essentially been a rearguard action to preserve the gains in scientific stature that the discipline has made over the past 30 years. However, in addition to preservation, biogerontologists have also been able to enhance their status through an influx of genetic research on aging. As more geneticists dwell in the world of biogerontology, the field has raised its profile as both more rigorous and of more consequence for our understanding of health and disease. The creation and flowering of the NIA clearly played a major role in these gains. But the scientific stature of biogerontology has also been enhanced by a series of discoveries that have specifically linked aging and longevity to genetics (see Masoro & Austad, 2006).
Many areas of biological research on aging have been descriptive, simply associating various phenomena with aging. For instance, a key example of this is the eight decades of research, using numerous animal models, that have established the longevity effects of dietary caloric restriction (see Masoro, 2001). In contrast, more recent research on the genetics of aging is seen as having powerful explanatory capabilities (e.g., see Masoro & Austad, 2006). Consequently, the genetic discoveries by biogerontologists have provided the discipline with new ways to study aging and longevity. It has also professionally allied biogerontologists with other basic scientists interested in using genetic techniques. In short, it has enabled the discipline of biogerontology to join what Fujimara (1996) has called the “scientific bandwagon” of molecular science. Emblematic of biogerontologists' eagerness to join the genetics bandwagon is the website of the American Federation for Aging Research (AFAR), a non-profit organization comprising biogerontologists and geriatricians. Founded in 1981, before most of the modern discoveries that have linked genes and aging, AFAR's website now proclaims — “There is no fountain of youth. But there may be genes” (American Federation for Aging Research, 2008).
The growing importance of genetics in the study of aging is apparent in Fig. 1, which presents data from a search of the U.S. CRISP (Computer Retrieval of Information on Scientific Projects) database of federally-funded biomedical research projects. The data are for each of three full decades of research funding, starting with 1975 (the year that NIA began funding operations) through 2004. The search was executed by entering the search term keywords “genetics aging” in the Enter Search Terms text field. We then selected the Boolean search option of “And” by clicking on the radio button. The CRISP search engine looked for these keywords within the text of the Grant Titles and Grant Abstracts to find at least any occurrence containing both genetics and aging. However, the results may or may not contain those words in that exact sequence. In addition to NIA-funded projects, it was possible to search for all NIH research grants that have linked genetics and aging, as well as such grants funded by six additional federal agencies.
Fig. 1.
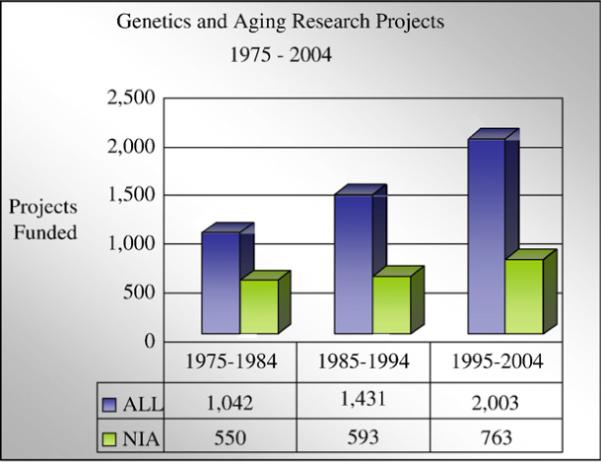
Source: CRISP database of U.S. federally federally-funded biomedical research projects, with search executed on April 21, 2008 by using the combined search terms “genetics and aging” for the years 1975–2004 http://crisp.cit.nih.gov/crisp/crisp_query.generate_screen.
As can be seen in Fig. 1, the growth of funded research projects on aging that feature genetics was steady over these 30 years. Especially striking is the growth in the number of projects on genetics and aging in the 1995–2004 decade. This is the historical period immediately following and including the years when a number of important research studies that linked genetics and aging were published. The number of NIA grants for studies of genetics and aging in the 1995–2004 decade increased by 29% over the previous decade. Especially striking is that the total number of grants by all of the federal agencies listed in the CRISP database, for research on genetics and aging, increased by 40% from the 1985–1994 decade.
As indicated in the article by Settersten et al. in this issue, one way that biogerontologists talk about the power of genetic and other explanatory discoveries is to refer to their work as uncovering the “fundamental mechanisms” of aging. In other words, instead of earlier models of aging which looked at the manifestations and effects of age-related diseases, contemporary biogerontologists, by and large, see their work as understanding the root causes of aging.
In describing what they mean by “fundamental mechanisms” scientists rely on ideas about how basic research on aging can uncover not only the mechanisms for aging, but therein also the mechanisms that lead to age-related diseases. Although many employ genetics for these mechanisms, what is important to these scientists is that they hope their work can tell us what lies at the center of all of the diseases associated with old age. As one senior and distinguished biogerontologist has put it, “One of the major underlying tenets held by virtually every geriatician is that aging is the greatest risk factor for all of the pathologies that they study” (Hayflick, 2002, p. 420).
The emphasis on fundamental mechanisms also accomplishes several other goals for the scientists. First, it establishes their work as both important and as having more potential than other areas of gerontology or even biomedical research. Their logic is that uncovering the basic mechanisms of aging would also uncover the causes for many of the diseases from which we suffer, and lead to specific applications to stop them. Second, it is an attempt to argue that NIH funding priorities, which tend to favor funding disease-based research over funding basic biogerontological research, should be reversed.
The public, political leaders, and health administrators easily understand the need to support research on Alzheimer's disease, cancer, stroke, or cardiovascular disease because these conditions are not only familiar to everyone but are feared by most. On the other hand, to most laypersons the biology of aging is a foggy abstraction that does not seem to play a direct role in what will be written on their death certificate…. Decision makers, the public, and many biomedical scientists themselves must realize that a greater commitment of resources must be made to understand the greatest risk factor for anything that will be written on their death certificates if they are lucky enough to become old. (Hayflick, 2002, p. 421).
Staying within “limits”
Biogerontologists' struggles for legitimation require that on the one hand, they keep their image consonant with the overarching goals of the NIA which are to prevent and cure age-related diseases. On the other hand they want to disassociate themselves from the imagery of the mythical fountain of youth. Biogerontologist Richard Miller has expressed this delicate balance:
[D]iscussions of research on life span extension are carefully skirted in political discourse at the National Institutes of Health and among similar custodians of public funding. One can sometimes get away with cautious circumlocutions (“we do research on late life illness”), but to be safe, it is clearly better to focus on how to “add life to years” and how “to learn the secrets of contributing to a healthy old age.” (Miller, 2002, p. 167)
On the other hand, many biogerontologists aspire to fountain-of-youth-like goals, that is, helping people remain relatively youthful throughout substantially extended life spans. For instance, Miller, himself, has suggested that by slowing aging it may be possible to “increase the mean and maximal life span by about 40%, which is a mean age at death of about 112 years for Caucasian American or Japanese women, with an occasional winner topping out at about 140 years” (Miller, 2002, p. 164). Miller's examples convey a sense of transhumanism that sharply transcends the boundaries of the NIH mission and culture. Moreover, rather than enhancing support for the biology of aging, it is fodder for vigorous opposition from sectors of society that object to life extension of these (and even lesser) magnitudes on moral and ethical grounds (see e.g., Kass, 2001). In 2003 the President's Council on Bioethics (2003) in the United States issued a report in which it highlighted the transhuman aspects of anti-aging research, labeling it as “beyond therapy.”
Aspirations such as Miller's lead him and other biogerontologists to continuously work at keeping perceptions of the goals of anti-aging science in harmony with the goals of NIH.
In 2006, three of Miller's colleagues joined him in an effort to emphasize that the goals of biogerontologists are modestly incremental. In a magazine article entitled “In Pursuit of the Longevity Dividend” they explained:
“What we have in mind is not the unrealistic pursuit of dramatic increases in life expectancy, let alone the kind of biological immortality best left to science fiction novels. Rather… we envision a modest deceleration in the rate of aging sufficient to delay all aging-related diseases and disorders by about seven years.” (Olshansky, Perry, Miller, & Butler, 2006, p. 32)
Six months later, at an event staged at the U.S. Capitol, a summary of the article was presented (orally and in writing) to members of Congress and their staffs. Ninety-nine scientists and other leaders in gerontology endorsed the document. This public display by biogerontologists is another boundary work activity, aimed at endearing themselves to NIA while distancing themselves from yet another set of marginal actors: “transhumanists” who promote the search for vastly extending human lifespan. By simultaneously denouncing this idea and promoting their work to prevent age-related diseases, biogerontologists attempt to cling to their status as mainstream and respectable scientists.
Nonetheless, while publicly steering clear of offering up the “forbidden fruits” of the previous and current “charlatans” in anti-aging medicine, biogerontology still aims to have a significant impact in the scientific arena and in affecting the nature of human aging. The work of biogerontologists in establishing the discipline has also simultaneously shaped the course of aging research. By promoting their field they have promoted a view of the aging process as a molecular and moreover genetic process. Despite the fact that they argue that there is no one gene that governs aging (Olshansky et al., 2002b), as we have indicated in this article it is the genetics of aging that currently carries the authoritative mantle for explaining the aging process. Biogerontology's status as a recognized and federally-funded science, affiliated with genetics, places it in prime position to influence both the aging process and our conception of what aging is.
There is much at stake in the continued and enhanced legitimacy of biogerontology, not only for the scientists but for society at large. As molecular explanations wax, other explanations are likely to wane, and so the field of gerontology as a whole is likely to move in new directions, with greater emphasis on intervening in the aging process. This presents mainstream gerontology with an “ideological crisis” (Moody, 2001/21) about whether we (and gerontology in particular) should indeed be intervening in the aging process. Biogerontology is playing a key role in shaping the very discipline that charges itself with the mission of research and thinking on aging.
Should biogerontology be successful in its goals (as varied and nebulous as those might be), it promises to alter our conception and treatment of illness and disease. Rather than treating one disease at a time, we may be combating one of the major risk factors for a wide variety of diseases and disabilities, radically altering our approach for treatment and perhaps even disease prevention. Not only might this alter life expectancy rates and individuals' experiences of health and illness but it might also radically change many of our social institutions, such as the nature of family life, the composition of labor forces, consumer markets, politics, the law, and public policy (see e.g., Hackler, 2001–2002, Post & Binstock, 2004, Seltzer, 1995). Also of particular concern might be issues of distributive justice regarding access to and allocation of anti-aging technologies (see e.g., Chapman, 2004), and possible scarce resources and ecological consequences of overpopulation (Hayflick, 1994). In short, as Juengst, Binstock, Mehlman, and Post (2003) have observed, what's at stake if biogerontologists are successful in controlling human aging are potential social and moral consequences that may be more profound than those generated by cloning and other controversial biotechnological developments.
Conclusions
This paper has demonstrated how biogerontology, as a field, has responded to the age-old notion that it is producing “forbidden knowledge” (Shattuck, 1996; Kempner et al., 2005). Forbidden knowledge refers to the idea that some arenas of scientific inquiry are considered off limits because of the perceived dangerousness of the knowledge in its potential to undermine social norms or to offend religious or moral authorities (Kempner et al., 2005). Biogerontology's perceived danger lies in its perception of radically changing human social life as we currently conceive it and also of allowing us to intervene in the aging process, thereby interfering with nature. Life extension research further breaks down cultural categories (e.g., life vs. death) from which we as a society make meaning of the world (Vincent, 2003).
Biogerontology is also a forbidden knowledge in other ways, in that the potential uses of this knowledge (whether legitimate or illegitimate) are ripe for commodification and profiteering, still considered a forbidden use according to the normative tenets of the scientific project (Merton, 1973). Indeed, as we have shown, there are many people out there who have already used the science (or at least its rhetoric) for this purpose. In order to combat these perceptions and implementations, biogerontologists distinguish the scientific knowledge they generate from these other more dangerous and moreover unsavory elements of “anti-aging” in order to stay in the good graces of national funding agencies and the public. However, it seems that with the continued attention and attraction of anti-aging as a field of inquiry and as a consumerist goal, biogerontology will continue to need to walk a fine line between promoting its research while minimizing its dangers.
Acknowledgements
This research was supported by a grant from the National Institute on Aging (2 RO1 AG020916-04A1), “Controlling Human Aging: Alternative Rationales and Implications.” The authors wish to acknowledge the assistance of the other members of our research team: Michael Flatt, Roselle Ponsaran, and Richard Settersten, Jr.
References
- A4M (American Academy of Anti-Aging Medicine) The American Academy of Anti-Aging Medicine. 2005 Retrieved May 31 2005, from http://www.worldhealth.net/p/96.html.
- A4M (American Academy of Anti-Aging Medicine) Board certifications. 2008 Retrieved January 8, 2008 from http://www.worldhealth.net/p/100,360.html.
- Abir-Am P. Themes, genres and orders of legitimation in the consolidation of new scientific disciplines: Deconstructing the historiography of molecular biology. History of Science. 1985;xxiii:73–117. doi: 10.1177/007327538502300103. [DOI] [PubMed] [Google Scholar]
- Achenbaum WA. Crossing frontiers: Gerontology emerges as a science. Cambridge University Press; New York: 1995. [PubMed] [Google Scholar]
- Amazon.com 2008 Retrieved January 12, 2008, from http:///www.amazon.com/You-Staying-Owners-Extending-Warranty/dp/0743292561/ref=pd_bbs_sr_1?ie=UTF8&s=books&qid=1200327242&sr=8-1.
- American Federation for Aging Research 2008 Retrieved April 22, 2008, from http://afar.org.
- Arumainathan S. Intellectual dishonesty in geriatric medicine — Truth versus fallacy: A4M sets the record straight on a campaign of disinformation challenging the facts of the science of anti-aging medicine. 2001 Retrieved November 3, 2003, from http://www.worldhealth.net/resources/IntellDishonesty.PDF.
- Binstock RH. The war on anti-aging medicine. Gerontologist. 2003;43:4–14. doi: 10.1093/geront/43.1.4. [DOI] [PubMed] [Google Scholar]
- Brown P, Zavetoski S. Social movements in health: An introduction. Sociology of Health and Illness. 2004;26:679–694. doi: 10.1111/j.0141-9889.2004.00413.x. [DOI] [PubMed] [Google Scholar]
- Bud R. The uses of life: A history of biotechnology. Cambridge University Press; Cambridge, UK: 1993. [Google Scholar]
- Business Communications Co., Inc. Anti-aging products and services. 2005 Retrieved September 26, 2007 from http:///www.bccresearch.com/RepTem-plate.cfm?reportID=465&RepDet=HLT/cat=phm&target=rep.detail.cfm.
- Chapman AR. The social and justice implications of extending the human life span. In: Post SG, Binstock RH, editors. The fountain of youth: Cultural, scientific, and ethical perspectives on a biomedical goal. Oxford University Press; New York: 2004. pp. 340–361. [Google Scholar]
- Clarke AE, Shim JK, Mamo L, Fosket JR, Fishman JR. Biomedicalization: Technoscientific transformations of health, illness, and U.S. biomedicine. American Sociological Review. 2003;68:161–194. [Google Scholar]
- Cowdry VE. Problems of aging: Biological and medical aspects. Williams and Wilkins; Baltimore, MD: 1939. [Google Scholar]
- Cozzens SE. Autonomy and power in science. In: Cozzens SE, Gieryn TF, editors. Theories of science in society. Indiana University Press; Bloomington, IN: 1990. pp. 164–184. [Google Scholar]
- Eisdorfer C. Patterns of federal funding for research in aging. Gerontologist. 1968;8:3–6. doi: 10.1093/geront/8.1_part_1.3. [DOI] [PubMed] [Google Scholar]
- Epstein S. Impure science. University of California Press; Berkeley, CA: 1996. [Google Scholar]
- Estes CL, Binney EA. The biomedicalization of aging: Dangers and dilemmas. Gerontologist. 1989;29:587–596. doi: 10.1093/geront/29.5.587. [DOI] [PubMed] [Google Scholar]
- Fox P. From senility to Alzheimer's disease: The rise of the Alzheimer's disease movement. Milbank Quarterly. 1989;67:58–102. [PubMed] [Google Scholar]
- Fujimura J. Crafting science: A sociohistory of the quest for the genetics of cancer. Harvard University Press; Cambridge, MA: 1996. [Google Scholar]
- Gieryn TF. Boundary-work and the demarcation of science from non-science: Strains and interests in professional ideologies of scientists. American Sociological Review. 1983;48:781–795. [Google Scholar]
- Gruman GJ. A history of ideas about the prolongation of life. Springer Publishing Company; New York: 2003. [Google Scholar]
- Guidestar Guidestar: The national database for nonprofit organizations. 2007 Retrieved September 26, 2007 from http://www.guidestar.org/pqShowGsReport.do? npoID=598448.
- Hackler C. Troubling implications of doubling the human lifespan. Generations. 2001/2002;25(4):15–19. [Google Scholar]
- Hayflick L. How and why we age. Ballantine Books; New York: 1994. [Google Scholar]
- Hayflick L. Anti-aging medicine: Hype, hope, and reality. Generations. 2001/2;25(4):20–26. [Google Scholar]
- Hayflick L. Anarchy in gerontological terminology. Gerontologist. 2002;42:416–421. [Google Scholar]
- Hedgecoe A. Terminology and the construction of scientific disciplines: The case of pharmacogenomics. Science, Technology, and Human Values. 2003;28:513–537. [Google Scholar]
- International Association of Gerontology and Geriatrics Longevity, health and wealth: First announcement. 2007 Retrieved September 18, 2007, from http://www.gerontologyparis2009.com/site/view8.php.
- Juengst ET, Binstock RH, Mehlman MJ, Post SG. Antiaging research and the need for public dialogue. Science. 2003;299:1323. doi: 10.1126/science.1083135. [DOI] [PubMed] [Google Scholar]
- Kass LR. L'chaim and its limits. Why not immortality? First Things. 2001;13:17–24. [PubMed] [Google Scholar]
- Kempner J, Perlis CS, Merz JF. Forbidden knowledge. Science. 2005;307:854. doi: 10.1126/science.1107576. [DOI] [PubMed] [Google Scholar]
- Klatz R. Anti-Aging medicine and why it must be part of your practice. 2007 Retrieved February 7, 2008, from http://findarticles.com/p/articles/mi_qa3987/is_20071105?ai_n21099430.
- Landzelius K. Patient organization movements and new metamorphoses in patienthood. Social Science and Medicine. 2006;62(3):529–537. doi: 10.1016/j.socscimed.2005.06.023. [DOI] [PubMed] [Google Scholar]
- Lockett BA. Aging, politics, and research: Setting the federal agenda for research on aging. Springer Publishing Company; New York: 1983. [Google Scholar]
- Masoro EJ. Caloric restriction's effects on aging: Opportunities for research on human implications. Journal of Gerontology: Biological and Medical Sciences. 2001;56A(special issue 1) doi: 10.1093/gerona/56.suppl_1.5. [DOI] [PubMed] [Google Scholar]
- Masoro EJ, Austad SN, editors. Handbook of the biology of aging. Academic Press; San Diego, CA: 2006. [Google Scholar]
- Merton RK. The normative structure of science. In: Merton RK, editor. The sociology of science: Theoretical and empirical investigations. University of Chicago Press; Chicago: 1973. pp. 267–278. [Google Scholar]
- Miller RA. Extending life: Scientific prospects and political obstacles. Milbank Quarterly. 2002;80:155–174. doi: 10.1111/1468-0009.00006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moody HR. Who's afraid of life extension? Generations. 2001/2;25(4):33–37. [Google Scholar]
- Mykytyn CE. Anti-aging medicine: A patient/practitioner movement to redefine aging. Social Science and Medicine. 2006;62:643–653. doi: 10.1016/j.socscimed.2005.06.021. [DOI] [PubMed] [Google Scholar]
- Mykytyn CE. Anti-aging medicine: Predictions, moral obligations, and biomedical intervention. Anthropological Quarterly. 2006;79:5–31. [Google Scholar]
- NIA (National Institute on Aging) Action plan for aging research: Strategic plan for fiscal years 2001–2005. 2001 Retrieved May 31, 2005, from http://www.nia.nih.gov/AboutNIA/StrategicPlan/ResearchGoalB/Subgoal1.htm.
- Nyberg JP. ILC Policy Report. May 1, 2002. The importance of aging research. [Google Scholar]
- Olshansky SJ, Carnes BA. The quest for immortality: Science at the frontiers of aging. Norton; New York: 2001. [Google Scholar]
- Olshansky SJ, Hayflick L, Carnes BA. No truth to the fountain of youth. Scientific American. 2002;286:92–95. doi: 10.1038/scientificamerican0602-92. [DOI] [PubMed] [Google Scholar]
- Olshansky SJ, Hayflick L, Carnes BA. Position statement on human aging. Journal of Gerontology: Biological Sciences. 2002;57A:B292–B297. doi: 10.1093/gerona/57.8.b292. [DOI] [PubMed] [Google Scholar]
- Olshansky SJ, Perry D, Miller RA, Butler RN. In pursuit of the longevity dividend. The Scientist. 2006;20(3):28–32. [Google Scholar]
- Pope E. 51 top scientists blast anti-aging data. AARP Bulletin. 2002;23:3–5. [Google Scholar]
- Post SG, Binstock RH, editors. The fountain of youth: Cultural, scientific, and ethical perspectives on a biomedical goal. Oxford University Press; New York: 2004. [Google Scholar]
- President's Council on Bioethics . Beyond therapy: Biotechnology and the pursuit of happiness. Harper Collins Publishers; New York: 2003. [Google Scholar]
- Research on Aging Act of 1974 . U.S. Public Law Number 93-296. 1974. [Google Scholar]
- Robert L. The three avenues of gerontology: From basic research to clinical gerontology and anti-aging medicine. Another French paradox. Journal of Gerontology: Biological Sciences. 2004;59A:540–542. doi: 10.1093/gerona/59.6.b540. [DOI] [PubMed] [Google Scholar]
- Robinson J. Noble conspirator: Florence S. Mahoney and the rise of the National Institutes of Health. The Francis Press; Washington, D.C.: 2001. [Google Scholar]
- Roizen M, Oz MC. You: Staying young: The Owner's Manual for Extending Your Warranty. Simon and Schuster; New York: 2007. [Google Scholar]
- Seltzer M, editor. The impact of increased life expectancy: Beyond the gray horizon. Springer Publishing Company; New York: 1995. [Google Scholar]
- Shattuck R. Forbidden knowledge: From Prometheus to pornography. Harcourt Brace and Company; New York: 1996. [Google Scholar]
- Taylor CA. Defining science: A rhetoric of demarcation. University of Wisconsin Press; Madison, WI: 1996. [Google Scholar]
- University of Illinois at Chicago . Silver fleece awards target anti-aging hype. Office of Public Affairs; 2002. News Release, February 12. Retrieved June 12, 2002, from http://tigger.uic.edu/htbin/cgiwrap/bin/newsbureau. [Google Scholar]
- U.S. GAO (General Accounting Office) Health products for seniors: “Anti-aging” products pose potential for physical and economic harm. U.S. Government Printing Office GAO-01-1129; Washington, DC: 2001. [Google Scholar]
- U.S. Senate Subcommittee on Aging (of the Committee on Labor and Public Welfare) Research on Aging Act,1973. U.S. Government Printing Office; Washington, DC: 1973. [Google Scholar]
- van Lente H, Rip A. The rise of membrane technology: From rhetorics to social reality. Social Studies of Science. 1998;28:221–254. [Google Scholar]
- Vincent J. What is at stake in the “war on anti-aging medicine”? Ageing and Society. 2003;23:675–684. [Google Scholar]
- Warner H. Making the political case for biogerontology funding: A view from the trenches. Paper presented at the SENS 3 Conference; Cambridge, England. Sep 9, 2007. [DOI] [PubMed] [Google Scholar]
- Warner H, Andersen J, Austad S, Bergamini E, Bredsen D, Butler R, et al. Science fact and the SENS agenda. EMBO Reports. 2005;6:1006–1008. doi: 10.1038/sj.embor.7400555. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wilson D. Aging: Disease or business opportunity? 2007 New York Times Retrieved September, 17, 2007 from http://www.nytimes.com/2007/04/15/business/yourmoney/15aging.html?ex=1189483200&en=2b075b8de1c1b427&ei=5070.
- Youngevity The Youngevity story. 2003 Retrieved May 24, 2003, from http://www.youngevity.com/the_ygy_story_fs.htm.