An official website of the United States government
Here's how you know
Official websites use .gov
A
.gov website belongs to an official
government organization in the United States.
Secure .gov websites use HTTPS
A lock (
) or https:// means you've safely
connected to the .gov website. Share sensitive
information only on official, secure websites.
As a library, NLM provides access to scientific literature. Inclusion in an NLM database does not imply endorsement of, or agreement with,
the contents by NLM or the National Institutes of Health.
Learn more:
PMC Disclaimer
|
PMC Copyright Notice
1Massachusetts General Hospital Cancer Center, Harvard Medical School
2Princess Margaret Hospital, University of Toronto
✉
Correspondence: Andrew Zhu, M.D., Ph.D., Massachusetts General Hospital, 55 Fruit Street, Cancer Center POB Room 232, Boston, Massachusetts 02114, USA. Telephone: 617-724-3853; Fax: 617-724-3166; e-mail: azhu@partners.org. Jennifer J. Knox, M.D., M.Sc., FRCPC, Princess Margaret Hospital, 5th Floor Room 218, 610 University Avenue, Toronto, Ontario, Canada M5G 2M9. Telephone: 416-946-2399; Fax: 416-946-6546; e-mail: jennifer.knox@uhn.ca
Received 2012 Nov 8; Accepted 2012 Nov 9; Issue date 2012 Dec.
The role of adjuvant therapy in the treatment of intrahepatic cholangiocarcinoma is debated.
Abstract
Presentation of the Case
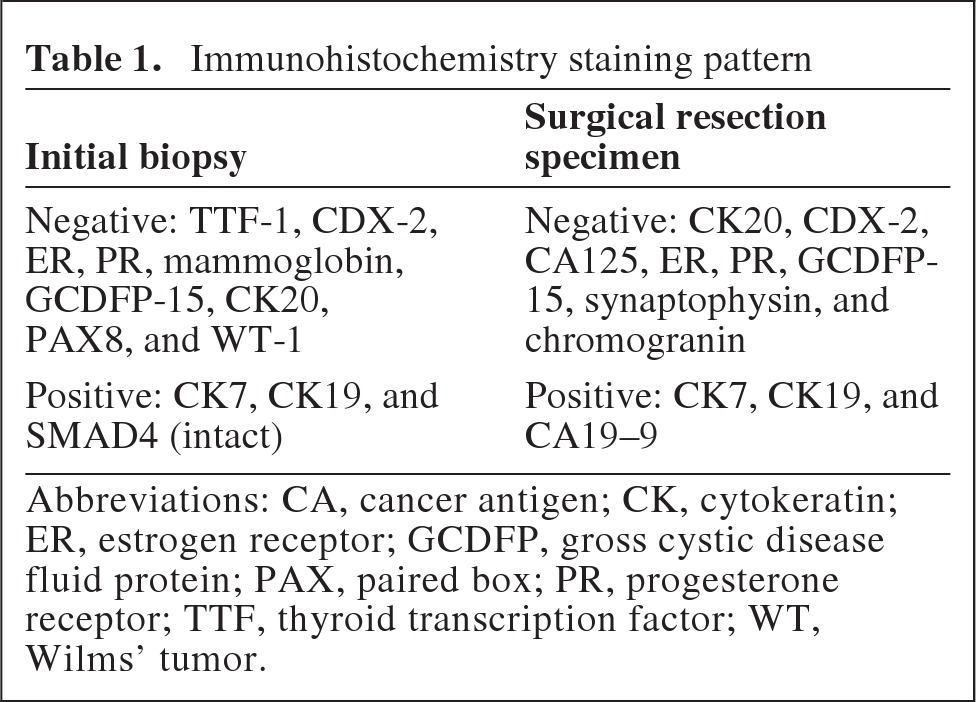
A 37-year-old woman presented at 35 weeks of gestation with her third child with failure to adequately gain weight and was noted by her obstetrician to have delay in the growth of her baby. Ultrasound of the abdomen incidentally revealed the presence of a liver lesion. After additional evaluation, she ultimately delivered her daughter at 36 weeks uneventfully. She subsequently underwent additional evaluation. Liver magnetic resonance imaging (MRI) revealed a 5-cm solitary solid mass in segment 4A of the liver, concerning for malignancy. Serum α-fetoprotein, carcinoembryonic antigen, cancer antigen (CA)19–9, CA15–3, and CA125 were all normal. Liver biopsy was positive for adenocarcinoma. The tumor cells demonstrated a phenotype suggesting a possible breast primary, although the immunohistochemistry did not support that diagnosis and the tumor was negative for mammaglobin, gross cystic disease fluid protein (GCDFP)-15, estrogen receptor (ER), and progesterone receptor (PR) (Table 1). The tumor was also CDX2 and cardiotrophin-1 negative, but cytokeratin (CK) 19 positive. Her endoscopic retrograde cholangiopancreatography, upper endoscopy, colonoscopy, breast mammogram, and breast MRI were completely normal. A positron emission tomography–computed tomography scan showed a fluorodeoxyglucose-avid 5.8-cm × 6.0-cm hypoattenuating lesion with peripheral enhancement involving segment 4 and segment 8 at the dome. In addition, central necrosis within the lesion was noted. The left main portal vein was mildly attenuated by the mass. She eventually underwent a left hepatectomy en bloc with caudate resection, portal lymphadenectomy, cholecystectomy, and omental pedicle flap. On exploration of the abdomen, no additional disease was noted. The final pathology revealed a 9.4-cm moderately to poorly differentiated adenocarcinoma of the intrahepatic bile ducts. Venous invasion was present. Perineural invasion was absent. The margins were negative. Thirteen lymph nodes were obtained, all of which were negative, consistent with a stage T2, N0, MX intrahepatic cholangiocarcinoma. The tumor was positive for CK7, CK19, and CA19–9 and negative for CK20, CDX2, CA125, ER, PR, GCDFP-15, synaptophysin, and chromogranin (Table 1). The uninvolved liver was unremarkable and a trichrome stain showed no fibrosis. Following an uneventful postoperative recovery, she was referred for consideration of adjuvant therapy.
Biliary tract cancers (BTCs) encompass a spectrum of invasive adenocarcinomas including both cholangiocarcinoma (CC), which has been used to refer to cancers arising in the intrahepatic, perihilar, or distal biliary tree, and carcinoma arising from the gallbladder [1]. They are characterized by early lymph node (LN) and distant metastasis. Because of the incomplete understanding of the risk factors and the lack of screening strategies for most BTCs [2], only 10%–20% of patients present with early-stage disease and are considered candidates for surgical resection, which offers the only chance for cure [3, 4]. Whereas combined gemcitabine and cisplatin has become the standard treatment for patients with unresectable or metastatic BTC based on the Advanced Biliary Cancer (ABC)-02 trial [5], clinicians continue to face the dilemma of whether or not adjuvant therapy should be considered for patients undergoing definitive surgical resection, as highlighted in the case presented here.
Intrahepatic CC (ICC) represents a unique clinical entity. It constitutes the second most common form of liver malignancy, and incidence as well as mortality rates have been steadily increasing [6]. Recent research has also highlighted the different molecular profiles of ICC in comparison with other BTCs, as evidenced by the newly identified mutations in the gene encoding isocitrate dehydrogenase (IDH)1 and IDH2 in ICC [7–9]. Why would clinicians consider the use of adjuvant therapy for ICC? It is well known that the recurrence rate is very high for patients undergoing definitive surgical resection for ICC. The 5-year overall survival rate after surgical resection for ICC is in the range of 14%–40% in reported series [1]. The liver is the most common site of recurrence either alone or in combination with one or more extrahepatic sites [10]. Factors that most influence recurrence are the presence of multiple tumors and LN metastasis. In one report [10], in patients with solitary tumors with no LN metastasis, the recurrence rate was 47%, whereas in patients with multiple tumors or LN metastasis this rate was higher, at 93%. Analysis of an international multi-institutional cohort of 449 patients demonstrated a median survival time of 27 months and 5-year survival rate of 31% [11]. For patients undergoing lymphadenectomy, 30% had LN metastasis, and this group had a poorer outcome (median survival time: N0, 30 months; N1, 24 months; p = .03). Although tumor size provides no prognostic information, the presence of multiple tumors, vascular invasion, and LN metastasis are associated with a poorer survival outcome. Other studies have also indicated the poor prognostic significance of lymphovascular and perineural invasion [12]. Interestingly, the presence of either lymphovascular or perineural invasion in node-negative patients was associated with a shorter overall survival duration, similar to that of node-positive patients (12.1 months vs. 10.7 months; p = .541). The high rate of lymphovascular and perineural invasion and nodal and distant metastasis, and the associated adverse outcomes, highlight the importance of developing effective adjuvant chemotherapy for ICC.
The rationale of delivering adjuvant therapy is based on the premise that there are microscopic cancer cells escaping the primary tumor site either at presentation or not completely removed by resection, and that administration of additional effective therapy following surgery will improve the chance of eradicating these cells, leading to better disease-free survival and overall survival outcomes. In general, there are two patterns of recurrence: local recurrence and systemic metastases. Because of the unique features of ICC, the surgical resection margin is usually adequate and recurrence is usually in the form of intrahepatic, nodal, and distant metastasis. Therefore, the role of adjuvant therapy for ICC is more relevant for systemic therapy in an attempt to decrease the risk for metastasis.
What is the evidence supporting the use of adjuvant therapy in BTC patients? Because of their traditionally poor response to systemic chemotherapy and the relative rarity of these tumors, conducting adjuvant clinical trials has been challenging. Therefore, the role of adjuvant therapy in patients with BTCs of all sites (intrahepatic, hilar, distal bile duct, and gallbladder) is not established, and no level 1 evidence exists based on randomized phase III studies. The recently published European Study Group for Pancreatic Cancer (ESPAC)-3 study examined the use of adjuvant chemotherapy with 5-fluorouracil (5-FU) plus folinic acid or gemcitabine versus observation in patients with periampullary cancer in a randomized trial [13]. Based on the primary analysis, that study failed to demonstrate that adjuvant chemotherapy, compared with observation, conferred a survival benefit for patients with resected periampullary adenocarcinoma; however, after adjusting for the independent prognostic variables of age, bile duct cancer, poor tumor differentiation, and positive LNs and after conducting a multiple regression analysis, a statistically significant survival benefit was observed with adjuvant chemotherapy. Horgan and colleagues performed a systematic review and meta-analysis of >6,000 patients and examined the benefits of adjuvant chemotherapy, radiation, or chemoradiation for patients with resected BTC [14]. In that study, patients receiving adjuvant chemotherapy or chemoradiation derived statistically greater benefit than those treated with radiation alone (odds ratio [OR], 0.39, 0.61, and 0.98, respectively; p = .02). The greatest benefits for adjuvant chemotherapy were in those with LN+ disease (OR, 0.49; p = .004) and R1 disease (OR, 0.36; p = .002). The lack of definitive benefits of adjuvant therapy in ICC patients is reflected by the National Comprehensive Cancer Network guideline: those with R0 resection would be recommended for observation or participation in clinical trials [15]. With the development of more effective systemic chemotherapy and the well-recognized high recurrence rate, there is an urgent need to conduct clinical trials to define the role of adjuvant therapy in this setting. Currently, several phase III adjuvant trials in BTC patients are ongoing. In France, a multicenter study is examining the combination of gemcitabine and oxaliplatin for 6 months versus observation in patients with resected BTC (ClinicalTrials.gov identifier, NCT01313377). The value of adjuvant capecitabine given for 24 weeks versus observation in patients with resected BTC is under investigation in a randomized phase III study in the U.K. (ClinicalTrials.gov identifier, NCT00363584). The optimal regimen and duration for adjuvant chemotherapy in BTC patients should also be examined in the future. Before the evidence is available, however, it is reasonable to consider adjuvant therapy in selected circumstances, such as in patients with nodal metastasis, vascular invasion, or margin positivity. Despite the known toxicity, the tolerability of gemcitabine given either alone or in combination with cisplatin is favorable based on the ABC-02 trial and extensive clinical experience.
In conclusion, for this patient with a large tumor and vascular invasion, I recommended the use of adjuvant therapy with the combination of gemcitabine and cisplatin for 12 weeks (four cycles).
Supplementary Material
Click Here to Access Challenging Cases and Participate in the Discussion
5.Valle J, Wasan H, Palmer DH, et al. Cisplatin plus gemcitabine versus gemcitabine for biliary tract cancer. N Engl J Med. 2010;362:1273–1281. doi: 10.1056/NEJMoa0908721. [DOI] [PubMed] [Google Scholar]
6.Shaib YH, Davila JA, McGlynn K, et al. Rising incidence of intrahepatic cholangiocarcinoma in the United States: A true increase? J Hepatol. 2004;40:472–477. doi: 10.1016/j.jhep.2003.11.030. [DOI] [PubMed] [Google Scholar]
7.Borger DR, Tanabe KK, Fan KC, et al. Frequent mutation of isocitrate dehydrogenase (IDH)1 and IDH2 in cholangiocarcinoma identified through broad-based tumor genotyping. The Oncologist. 2012;17:72–79. doi: 10.1634/theoncologist.2011-0386. [DOI] [PMC free article] [PubMed] [Google Scholar]
8.Kipp BR, Voss JS, Kerr SE, et al. Isocitrate dehydrogenase 1 and 2 mutations in cholangiocarcinoma. Hum Pathol. 2012;43:1552–1558. doi: 10.1016/j.humpath.2011.12.007. [DOI] [PubMed] [Google Scholar]
9.Wang P, Dong Q, Zhang C, et al. Mutations in isocitrate dehydrogenase 1 and 2 occur frequently in intrahepatic cholangiocarcinomas and share hypermethylation targets with glioblastomas. Oncogene. 2012 Jul 23; doi: 10.1038/onc.2012.315. [Epub ahead of print]. doi: 10.1038/onc.2012.315. [DOI] [PMC free article] [PubMed] [Google Scholar]
10.Endo I, Gonen M, Yopp AC, et al. Intrahepatic cholangiocarcinoma: Rising frequency, improved survival, and determinants of outcome after resection. Ann Surg. 2008;248:84–96. doi: 10.1097/SLA.0b013e318176c4d3. [DOI] [PubMed] [Google Scholar]
11.de Jong MC, Nathan H, Sotiropoulos GC, et al. Intrahepatic cholangiocarcinoma: An international multi-institutional analysis of prognostic factors and lymph node assessment. J Clin Oncol. 2011;29:3140–3145. doi: 10.1200/JCO.2011.35.6519. [DOI] [PubMed] [Google Scholar]
12.Fisher SB, Patel SH, Kooby DA, et al. Lymphovascular and perineural invasion as selection criteria for adjuvant therapy in intrahepatic cholangiocarcinoma: A multi-institution analysis. HPB (Oxford) 2012;14:514–522. doi: 10.1111/j.1477-2574.2012.00489.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
13.Neoptolemos JP, Moore MJ, Cox TF, et al. Effect of adjuvant chemotherapy with fluorouracil plus folinic acid or gemcitabine vs observation on survival in patients with resected periampullary adenocarcinoma: The ESPAC-3 periampullary cancer randomized trial. JAMA. 2012;308:147–156. doi: 10.1001/jama.2012.7352. [DOI] [PubMed] [Google Scholar]
14.Horgan AM, Amir E, Walter T, et al. Adjuvant therapy in the treatment of biliary tract cancer: a systematic review and meta-analysis. J Clin Oncol. 2012;30:1934–1940. doi: 10.1200/JCO.2011.40.5381. [DOI] [PubMed] [Google Scholar]
15.Benson AB, 3rd, Abrams TA, Ben-Josef E, et al. NCCN clinical practice guidelines in oncology: Hepatobiliary cancers. J Natl Compr Canc Netw. 2009;7:350–391. doi: 10.6004/jnccn.2009.0027. [DOI] [PMC free article] [PubMed] [Google Scholar]
The strongest arguments against recommending adjuvant therapy for this case are both the lack of evidence supporting clear benefit for such a patient and the lack of evidence refuting its potential harm. When we are faced with such a patient, whom we know is at high risk for recurrence, oncologists generally prefer to rely on recommendations drawing from level 1 evidence. We don't have this luxury when it comes to adjuvant therapy for CC and, in particular, for the intrahepatic variant as in this case. Although some patients can appreciate an ambiguous risk–benefit discussion with their oncologist and perhaps even help you come to the best informed decision for them, most are waiting for their oncologist to explicitly advise them clearly on what they need to do in order to stay alive. This situation often biases us toward supporting adjuvant therapy in the absence of known benefit. “It probably won't do any harm and may well help, after all it does in so many other types of cancer.” This is certainly an approach I have taken with patients. In his Pro discussion, Dr. Zhu recommended gemcitabine plus cispatin doublet (GemCis) adjuvant chemotherapy in this case.
The case describes an ICC, moderate to poorly differentiated, with vascular invasion, resected with clear margins and a negative nodal status. It also describes the patient as young and having recently given birth to a child as an added level of emotional charge to the decision. We appreciate that ICC patients are at high risk for recurring either within the liver or at distal metastatic sites. The 5-year overall survival rate is in the range of 14%–40%, favoring those with clear margins and node negativity, but all odds are generally poor [1]. And, of course, recurrence with this cancer is likely to be unresectable and the patient's survival duration in that setting would be short. With advanced disease, chemotherapy such as GemCis has been shown to result in a longer median survival time, 11.7 months versus 8.1 months with gemcitabine alone (hazard ratio, 0.64; p < .001) [2]. GemCis treatment-related toxicities are moderate in that palliative setting. Therefore, asking if this doublet could have greater impact if offered earlier in the adjuvant setting is very tempting, with the premise that micrometastatic disease can be eradicated with active chemotherapy. Let us examine the evidence for this approach in biliary cancer patients.
Perhaps the most relevant report is the recent meta-analysis cited by Dr. Zhu in his Pro argument. Horgan and colleagues [3] reviewed the best prospective and retrospective comparative data on adjuvant therapy for biliary cancer and drew some reasonable conclusions. Data from >6,000 patients comparing surgery alone with some form of adjuvant therapy (chemotherapy, radiation, or combined therapy) demonstrated a nonsignificant overall survival benefit with any form of adjuvant therapy over surgery alone. Those receiving chemotherapy (mainly 5-FU based) or chemoradiation did better than those receiving radiotherapy alone (OR, 0.39, 0.61, and 0.98, respectively; p = .02), but the greatest benefit was seen in those higher risk patients with LN+ disease (OR for 5-year survival; 0.49; p = .004) or R1 resections (OR, 0.36; p = .002.) The analysis, however, did not support a benefit for adjuvant therapy in the relatively lower risk groups, such as patients with node-negative disease. Prospective trials are anxiously awaited to confirm these findings. It is also important to point out that, although this review may provide some of the best data to date to recommend adjuvant chemotherapy in biliary cancer patients, it is noteworthy that, in all included studies, spanning some 40 years and >6,700 patients, only one study included patients with ICC, for a total of 11 ICC patients. So, really, no recommendations from this meta-analysis can apply directly to ICC cases, which may well be biologically distinct from the extrahepatic and gallbladder cancers reviewed here. Similarly, the trend for a longer survival time with adjuvant chemotherapy (single-agent gemcitabine or 5-FU) in the periampullary subset of the ESPAC-3 trial provides indirect support in a related tumor site but nothing specific to ICCs [4]. Nor could either of these studies evaluate the impact of adjuvant therapy in patients with tumors with vascular invasion.
Recently, a study from China examined adjuvant transarterial chemoembolization (TACE) after resected ICC in 147 patients [5], favoring a survival benefit with adjuvant TACE for patients with ICCs >5 cm. The methodology and the retrospective design of that study limit its interpretation. However, it does suggest that this approach should be studied further in a randomized study.
The other argument used to recommend adjuvant therapy in the absence of evidence is that the adjuvant chemotherapy would likely cause no harm. Experience with GemCis in the metastatic setting suggests that it is well tolerated, although there are issues of fatigue, myleosuppression, and declining creatinine clearance that is occasionally challenging. However, the risk–benefit ratio of an adjuvant therapy needs to be at its most optimal in order to preserve any modest benefits gained. It is reasonable that some form of chemotherapy, once properly studied in the adjuvant setting, will turn out to improve recurrence rates by a small but real absolute value, say by an estimate of 5%–10%. So what about the acute and long-term toxicities in this setting competing with the small benefits?
One potential problem to consider: we know from cancer series using cisplatin-based chemotherapy regimens that the risk for thromboembolic events (TEEs) can be very high, and in addition to general morbidity, some of these events are fatal. In one recent large series [6] reviewing 932 patients treated with any cisplatin-based chemotherapy across the early, locally advanced, and metastatic settings, treatment-related TEEs were seen in 18% of cases, with the majority occurring in the first 100 days of starting cisplatin. Rates were even higher in patients with certain malignancies, such as CC (28%), gallbladder or ampullary cancer (30%), and pancreatic cancer (37%). This is an unacceptable incidence rate. Clear recommendations for prophylactic anticoagulation are not available, and the rates appear considerably higher than with other noncisplatin regimens in the same populations. Given that the therapeutic index is expected to be tight in the adjuvant setting, we cannot assume that GemCis adjuvant therapy is at all optimal. The U.K. trial currently evaluating single-agent capecitabine versus observation in patients with curatively resected biliary cancer (including ICC) could be quite informative on this single-agent approach. Consider also that the advancement of 5-FU, leucovorin, and oxaliplatin chemotherapy over single-agent 5-FU as an adjuvant therapy for stage 3 colon cancer is real and clinically meaningful, but the “lion's share” of the adjuvant benefit is derived from the 5-FU–based chemotherapy.
My best recommendation for this patient would include enrollment in an adjuvant clinical trial that includes an observation alone arm (if available) or observation alone outside a trial. If this patient could not accept that recommendation and was clearly motivated to undergo adjuvant therapy in the absence of specific supporting data, and understood the potential low therapeutic benefit, I would recommend a single-agent regimen for six cycles, such as gemcitabine or capecitabine, in the hope that this had the benefit she requires.
2.Valle J, Wasan H, Palmer DH, et al. Cisplatin plus gemcitabine versus gemcitabine for biliary tract cancer. N Engl J Med. 2010;362:1273–1281. doi: 10.1056/NEJMoa0908721. [DOI] [PubMed] [Google Scholar]
3.Horgan AM, Amir E, Walter T, et al. Adjuvant therapy in the treatment of biliary tract cancer: A systematic review and meta-analysis. J Clin Oncol. 2012;30:1934–1940. doi: 10.1200/JCO.2011.40.5381. [DOI] [PubMed] [Google Scholar]
4.Neoptolemos JP, Moore MJ, Cox TF, et al. Effect of adjuvant chemotherapy with fluorouracil plus folinic acid or gemcitabine vs observation on survival in patients with resected periampullary adenocarcinoma: The ESPAC-3 periampullary cancer randomized trial. JAMA. 2012;308:147–156. doi: 10.1001/jama.2012.7352. [DOI] [PubMed] [Google Scholar]
5.Wu ZF, Zhang HB, Yang N, et al. Postoperative adjuvant transcatheter arterial chemoembolisation improves survival of intrahepatic cholangiocarcinoma patients with poor prognostic factors: Results of a large monocentric series. Eur J Surg Oncol. 2012;38:602–610. doi: 10.1016/j.ejso.2012.02.185. [DOI] [PubMed] [Google Scholar]
6.Moore RA, Adel N, Riedel E et L. High incidence of thromboembolic events in patients treated with cisplatin-based chemotherapy: A large retrospective analysis. J Clin Oncol. 2011;29:3466–3473. doi: 10.1200/JCO.2011.35.5669. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Click Here to Access Challenging Cases and Participate in the Discussion