

Abstract
Automated analyses of full-day recordings were used to determine whether young children who are hard-of-hearing (HH) received similar levels of exposure to adult words and conversational interactions as age-matched peers with normal-hearing (NH). Differences in adult input between children in this study and in a normative database were considered. Finally, factors were examined that may have contributed to individual differences in the input characteristics of families. Results indicated that the NH and HH groups were exposed to similar numbers of adult words and conversational turns. However, both the NH and HH groups were exposed to more adult words and engaged in more conversational turns than the NH children in the normative sample. Considering only the HH group, both quantity of adult words and conversational exchanges were correlated with children’s auditory characteristics. Children’s receptive language ability was correlated with conversational exchanges but not with adult word counts.
Children’s exposure to language during the early language-learning period plays a critical role in shaping their linguistic development. Most children spend the majority of this period being cared for by their family members (Belsky et al., 2007), and parents are key contributors to the amount of talk to which children are exposed (Hart & Risley, 1995). However, parents vary in terms of how talkative they are and in terms of how much talk they direct to their children (Gilkerson & Richards, 2009; Hart & Risley, 1995). These differences in quantity of parent talk have significant implications for linguistic outcomes in children who are typically developing, because quantity of parent talk is linked to children’s later lexical proficiency, with children of talkative parents demonstrating stronger linguistic abilities than children of less talkative parents (Hoff & Naigles, 2002; Hurtado, Marchman, & Fernald, 2008; Huttenlocher, Haight, Bryk, Seltzer, & Lyons, 1991).
There are a number of reasons why high rates of linguist input from parents may contribute to children’s linguistic outcomes. First, children of talkative parents are exposed to instances of individual words more frequently than children of less talkative parents. This provides children with more opportunities to make connections between the phonological form of a word and its meaning (Huttenlocher et al., 1991). Evidence of this is found in research indicating that typically developing children command lexical and phonological forms earlier when those words are more frequent in their auditory environment, as compared with items that are less frequent in the adult talk to which they are exposed (Blackwell, 2005; Goodman, Dale, & Li, 2008; Schwartz & Terrell, 1983). Second, there are some features of linguistic input that are known to be especially important for children’s linguistic growth, such as exposure to past tense verbs, modifiers (i.e., adjective and adverbs), and function words (i.e., pronouns, prepositions, demonstratives, and articles). Although some parents use these linguistic features more often in their utterances than other parents, overall, the more talk children are exposed to, the more frequently they are exposed to these features (Hart & Risley, 1995, 1999). Third, frequency of parent talk is predictive of how frequently typically developing children talk by the time they are 2–3 years of age (Hart & Risley, 1999). This influence of frequency of parent input is important because children who talk more frequently accumulate more practice with language than less talkative children, which may further advance their linguistic development. Finally, Hurtado, Marchman, and Fernald (2008) have shown that the quantity and quality of maternal speech directed to a child is strongly related to the speed of lexical processing in typically developing children, even for words that are well known.
The tendency of parents to be talkative or taciturn appears to be relatively stable over time (Huttenlocher et al., 1991; Huttenlocher, Vasilyeva, Waterfall, Vevea, & Hedges, 2007; Olsen-Fulero, 1982) and may be related to factors such as parents’ socioeconomic status (SES; Hart & Risley, 1995; Hoff, 2003; Hoff-Ginsberg, 1994; Huttenlocher et al., 2007; Rowe, 2008; Rowe, Pan, & Ayoub, 2005). The majority of studies examining the relationships between SES and parent talkativeness indicate that less advantaged parents (i.e., less educated parents or parents in low-income homes) talk to their children less frequently than more advantaged parents (Fernald & Weisleder, 2011; Hoff, 2003; Huttenlocher et al., 2007; Rowe, 2008; Rowe et al., 2005). This may be a result of inherent differences between parents of different social classes in their general talkativeness or verbal abilities, the amount of time they have to talk with their children, or their knowledge and beliefs regarding the importance of their role in facilitating their child’s language development (Hoff-Ginsberg, 1994; Rowe, 2008). Regardless of the reason, the reduced input provided by low-SES parents to their children puts these children at a disadvantage for later linguistic achievement (Fernald & Weisleder, 2011; Hoff, 2003).
Although the influence of parent talk on child language abilities in typically developing children has been well established, research is more varied on whether child language abilities influence the amount of adult talk to which children are exposed. Some studies indicate that parents talk more to older children (Fraser & Roberts, 1975; Rowe et al., 2005; Snow, 1972), who presumably have more advanced language skills than younger children, and others find that parents do not increase their amount of talk in response to their child’s advancing language skills (Huttenlocher et al., 1991, 2007). Thus, the question arises as to whether the direction of influence between amount of parent talk and children’s linguistic abilities is from parent to child or child to parent. It may be that as children become more proficient language users, they become more skilled at initiating or participating in conversations, resulting in responsive parents providing more linguistic input within conversational interactions. For example, Hoff-Ginsberg (1987, 1994) reported that typically developing children with more advanced language abilities, especially those who were good turn-takers or who had stronger conversational skills, elicited more talk from their mothers. Thus, although a parent’s tendency to be talkative or taciturn likely is not dependent on their child’s linguistic abilities, the quantity of conversational exchanges and the amount of talk within these interactions may increase as children develop stronger language skills.
High rates of conversational exchanges may play a special role in promoting the language development of young children because of the joint attention shared between parents and children during these interactions and the potential for parents to provide contingent responses to children’s utterances. Joint attention refers to interactions in which the parent and child attend to the same target and are aware of this shared focus. These episodes have been argued to provide an optimal environment for word learning, given that joint attention increases the likelihood that children will understand that the parent’s intent is to refer to the shared target (Scofield & Behrend, 2011). Tomasello and Farrar’s (1986) work supports this premise, given their finding that maternal language provided within joint attention episodes, but not outside of joint attention episodes, was related to later child vocabulary knowledge. Importantly, they also found that mothers and children talked more and engaged in longer conversations during periods of joint attention than outside of these periods. In line with these findings, a number of other studies have indicated that parents who engage their children in more or lengthier joint attention episodes have infants who develop stronger language abilities than parents who engage their children in fewer joint attention episodes (Carpenter, Nagell, & Tomasello, 1998; Tomasello & Todd, 1983). Zimmerman et al. (2009) provided evidence of the importance of conversational exchanges, showing that the number of conversational turns that occurred between parents and their 2- to 48-month-old children was robustly and positively correlated with children’s language abilities approximately 18 months later, even when controlling for the children’s language abilities at the earlier time point.
Children With Hearing Loss and Quantity of Linguistic Exposure
Although several studies have examined the amount of language to which typically developing children are exposed, only a limited number of studies have examined quantitative aspects of parental communication for children who are deaf and hard-of-hearing (HH). Findings from these studies have been inconsistent. Although a number of studies have pointed toward decreased communicative interactions between hearing mothers and their deaf children (Lederberg & Mobley, 1990; Meadow, 1981; Wedell-Monnig & Lumley, 1980), other similar studies did not find between-group differences for quantity of communicative input (Lederberg & Everhart, 1998, 2000; Spencer, 1993). However, these studies were all completed with populations of children with hearing loss who are very different from children with hearing loss today as they were born prior to the implementation of universal newborn hearing screening programs and did not have access to current advances in hearing technology. More recent studies on linguistic input have focused exclusively on parents of children who are deaf, the majority of whom use cochlear implants. These studies have not made comparisons to parents of children with normal hearing (NH) and have generally focused more on qualitative rather than quantitative aspects of linguistic input (DesJardin, Ambrose, & Eisenberg, 2009; DesJardin & Eisenberg, 2007; Farran, Lederberg, & Jackson, 2009; Nicholas & Geers, 2007). In one of these studies, DesJardin and Eisenberg (2007) reported that the sheer number of words used by mothers in a mother–child book-reading interaction was not significantly correlated with children’s language skills. However, the length of maternal utterances, the number of different words used by mothers, and maternal use of facilitative language techniques were positively correlated with children’s linguistic abilities. This work indicates that maternal input can influence language outcomes for children who are deaf and utilize cochlear implants.
Of interest in the current study is whether quantity of linguistic input is altered in the home environments of children with mild to severe hearing loss who utilize hearing aids. Quantity of language input may be especially important for these HH children, as they typically communicate through the auditory-oral modality and thus rely on auditory input for language learning. However, their sensorineural hearing losses typically result in inconsistent and degraded access to the speech signal. Although this can be partially ameliorated through early and consistent use of hearing aids, hearing aids do not render the speech signal fully audible to the majority of HH children. This is evident in studies reporting on the proportion of speech that is audible to children through their hearing aids (represented by Speech Intelligibility Index [SII] values). SII values range from 0 to 1, where 0 relates to the entire speech spectrum being inaudible and 1 relates to complete audibility. Bagatto et al. (2011) reported that the average SII value of the 62 children with hearing loss in their study was .662 (range: .11–.96). Similarly, Stiles, Bentler, and McGregor (2012) reported that the average SII value of the 18 children in their study was .699 (range: .23–.96). Although children with less significant hearing losses demonstrated higher audibility levels, hearing aids did not render speech completely audible for any child in either study. Children’s access to linguistic information is further reduced during periods without amplification and in difficult listening environments (e.g., listening to distant speech or in noisy or highly reverberant environments). Although other assistive listening technologies, such as frequency modulation (FM) systems, may be used to provide children with higher quality access to linguistic input in these difficult listening environments, these devices cannot overcome the audibility issues associated with hearing aid use.
To compensate for limitations in access to the speech signal, children who are HH may need increased exposure to language input to achieve the same linguistic outcomes as their peers with NH. Evidence of this can be found in studies indicating that children who are HH require more exposures to a word than children with NH to add it to their lexicon (Lederberg, Prezbindowski, & Spencer, 2000; Lederberg & Spencer, 2009; Pittman, Lewis, Hoover, & Stelmachowicz, 2005; Stelmachowicz, Pittman, Hoover, & Lewis, 2004). Additionally, children with hearing loss have difficulty hearing conversation from a distance, which results in having less access to overheard speech than children with NH, who utilize this route for word learning by 2.5 years of age (Akhtar, Jipson, & Callanan, 2001). Thus, input within conversational exchanges may be especially important for the linguistic development of children who are HH. Research is needed to further knowledge about the quantity of linguistic input available to children who are HH and whether that input differs from the input available to children with NH.
Despite the potential importance of high rates of linguistic input for children with hearing loss, reduced speech perception, speech production, and oral language skills may further inhibit language interactions between these children and their parents. For example, limitations in speech perception and/or audibility may result in children with hearing loss being less responsive to the input their parents provide, especially in difficult listening environments. This may prompt parents to limit their talk to situations in which they can ensure the child’s access to the auditory input. Additionally, speech production limitations and oral language delays may contribute to conversational breakdowns between children with hearing loss and their parents. These conversational breakdowns may lead to fewer conversational turns being taken between parents and children with hearing loss, thus reducing linguistic input within conversational interactions.
Professionals working with young children with hearing loss have long been aware of the importance of linguistic input for children who are HH and the potential for communicative interactions between children with hearing loss and their parents to be reduced in quantity or quality as compared to dyads in which the child has NH (Lederberg & Mobley, 1990; Meadow, 1981; Wedell-Monnig & Lumley, 1980). As a result, early interventionists who are educated in best practices for children with hearing loss and their families often directly target parental communication as a means of improving the linguistic outcomes of children who are HH, with a special emphasis on promoting linguistic input within conversational interactions (Cole & Flexer, 2008). These techniques are supported by work indicating that maternal communication style can be facilitative of communication development for children with hearing loss (DesJardin et al., 2009; Farran et al., 2009; Pressman, Pipp-Siegel, Yoshinaga-Itano, & Deas, 1999). The changes in parental communication style that occur as a result of early intervention may be partially responsible for the positive correlations seen between parent participation in early intervention and the later linguistic abilities of young children with hearing loss (Holzinger, Fellinger, & Beitel, 2011; Moeller, 2000). In addition, early intervention services are designed to reduce the language delays typically evidenced by children with hearing loss, potentially decreasing the frequency of conversational breakdowns in these dyads. Thus, intervention factors may help to moderate the effects of child hearing status on parental input.
There are two primary reasons for the limited research examining the amount of talk that parents provide to their young children with hearing loss. First, prior to the past decade children with hearing loss were not identified until approximately 2 years of age on average, with children with milder degrees of hearing loss often being identified even later (Mace, Wallace, Whan, & Stelmachowicz, 1991; Stein, Jabaley, Spitz, Stoakley, & McGee, 1990). Given that many children were not identified with hearing loss until the third year of life or later, researchers were unable to examine the contributions of parent talk to children’s early linguistic development. However, with universal newborn hearing screenings now in place, the average age of identification for children with hearing loss has dropped to approximately 3 months, with enrollment in early intervention services typically occurring shortly thereafter (Halpin, Smith, Widen, & Chertoff, 2010; Sininger et al., 2009; Spivak, Sokol, Auerbach, & Gershkovich, 2009). This has opened the possibilities for research examining the variables that influence the early language development of this population. A second barrier to these types of investigations in the past has been the extensive resources (e.g., time, money, and personnel) necessary for carrying out a study documenting the amount of adult words spoken to children with hearing loss, especially in a natural setting as opposed to a clinical setting. A new system, the LENA (Language ENvironment Analysis), is now available that allows for automated analyses of all-day recordings of children’s auditory environments (Gilkerson & Richards, 2008b). This system, which can be worn unobtrusively by young children to collect full-day recordings of their natural environments, dramatically reduces the costs previously associated with this type of research. The recorded samples have high ecological validity and are not influenced by the presence of unfamiliar adults (e.g., researchers) or bulky equipment. The technology provides estimates of linguistic and nonlinguistic variables such as the number of words spoken by adults in the child’s vicinity, the number of conversational turns taken between the child and adults, the extent to which audible television is present in the child’s environment, and the duration of noise and silence in the recordings. Normative data are available on the aforementioned linguistic measures for 2- to 48-month-old children with NH (Gilkerson & Richards, 2008b; Xu, Yapanel, & Gray, 2009).
Objectives
In this study, full-day recordings and automated analyses were used to address three objectives in HH and NH children. The first objective was to determine whether young children with hearing loss receive similar levels of exposure to adult words and conversational interactions as age-matched peers with NH. The second objective was to determine if adult output differs between children in the current study and children in the LENA normative database and the possible implications of using the normative database in future research or clinical endeavors with young children who are HH. The third objective was to examine the factors that may contribute to individual differences in the quantity of talk for families who have a child with hearing loss, including SES, receptive language abilities, and audiological variables.
Method
Participants
All participating children and families were part of a larger, multicenter, longitudinal study aimed at investigating outcomes of children with mild to severe hearing loss. The sample for the larger outcomes study comprises a broad cross-section of children intended to represent the population of children who are HH and a NH control cohort. The families consented to participate in annual evaluations that included collection of demographic information, assessment of audiological variables, and evaluation of children’s communication development. A subset of families with children enrolled in the larger study were also invited to participate in this substudy, in which they collected monthly recordings of children’s auditory environments as described in the Procedures section. The current analysis is focused on examination of one recording for each child, collected in the age range of 24–36 months. There were a total of 30 families1 from six U.S. states (Nebraska [n = 8], Iowa [n = 13], North Carolina [n = 6], Kansas [n = 1], Illinois [n = 1], and Georgia [n = 1]) who participated; 22 of the families had a HH child. Additional details of the sample are given in Table 1.
Table 1 .
Demographic details of participants
| Characteristic | HH (n = 22 children) | NH (n = 8 children) | NLS-Age (n = 804 recordings) | NLS-Age/SES (n = 454 recordings) |
|---|---|---|---|---|
| Age recording | ||||
| Mean (months) | 29.4 | 30.1 | 30.2 | 30.0 |
| SD | 2.9 | 3.8 | 3.4 | 3.3 |
| Range | 24–35 | 25–36 | 25–36 | 25–36 |
| Maternal education | ||||
| Some high school | 0% | 0% | 12% | 0% |
| High school | 14% | 0% | 32% | 0% |
| Some college | 18% | 25% | 30% | 53% |
| College | 64% | 75% | 26% | 47% |
| Not provided | 5% | 0% | 0% | 0% |
| Race | ||||
| Caucasian | 86% | 87% | ||
| Black | 9% | 0% | ||
| Other | 5% | 0% | ||
| Did not report | 0% | 13% | ||
| Ethnicity | ||||
| Hispanic | 9% | 0% | ||
| Not Hispanic | 91% | 87% | ||
| Not provided | 0% | 13% | ||
| Sex | ||||
| Male | 36% | 75% | ||
| Female | 74% | 25% | ||
| Age HL confirmed | ||||
| Mean (months) | 4.8 | |||
| SD | 5.7 | |||
| Range | 0.5–21 | |||
| Age HA fit | ||||
| Mean (months) | 6.5 | |||
| SD | 6.0 | |||
| Range | 1.5–22 | |||
| BEPTA | ||||
| Mean (dB SPL) | 51.7 | |||
| SD | 13.9 | |||
| Range | 27.5–82.5 | |||
| BESII | ||||
| Mean | 0.72 | |||
| SD | 0.15 | |||
| Range | 0.30–0.92 | |||
Note: BEPTA = better ear pure tone average; BESII = better ear speech intelligibility index; HA = hearing aid; HH = hard of hearing; HL = hearing loss; NH = normal hearing; NLS = natural language study; SES = socioeconomic status; SD = standard deviation.
Children with NH passed an audiological screening at 20 dB HL across the frequencies of 500–4000 Hz. For HH children, parent interviews confirmed that children had no major disabilities other than hearing loss, and all families used spoken English with their children, although one family reported using minimal signing at home. Age of identification of hearing loss in the HH group averaged 4.8 months (standard deviation [SD] = 5.7 months), and 17 of the 22 HH children were identified with hearing loss through newborn hearing screening. On the days that recordings were collected, parental reports indicate that children were using their hearing aids, on average, 78.4% of the hours reported. Nine of the 22 HH children were FM users, but FM usage is unknown during the recordings collected for this study. Full audiological evaluations were completed for each HH child an average of 1.18 months before recordings were collected (SD = 5 months). As part of the evaluation, better ear pure tone averages (PTA) were calculated (or interpolated for the youngest children) based on thresholds obtained at 500, 1000, 2000, and 4000 Hz. Additionally, hearing aid and real ear measurements were obtained using the Audioscan Verifit following ANSI protocol S3.22 (2003). Following these measurements, Audioscan Verifit software was used to calculate an aided audibility measurement (Bentler, Hu, & Cole, 2011), based on the SII (ANSI S3.5-1997), to estimate the proportion of the amplified speech spectrum that was audible to HH children when wearing their hearing aids. SII does not take into account specific acoustic situations encountered by children in the course of a day, thus leaving open the question of auditory access in specific listening situations. Stimuli were presented at 65 dB SPL and measures from the better ear are reported in Table 1. To calculate SII, the speech spectrum is divided into frequency bands and assigned individual frequency-importance weights based on each band’s contribution to the intelligibility of speech. The weighted amount of audible information in each band is then summed to determine the SII. SII is reported on a scale from 0 to 1 in which 0 represents the entire speech spectrum as inaudible and 1 as completely audible.
The language abilities of HH children were evaluated using the receptive language scale of the Mullen Scales of Early Learning (MSEL; Mullen, 1995). The MSEL combines clinician-elicited and parent-reported items, resulting in a standardized t-score with mean of 50 and a SD of 10. A total of 19 of the 22 children in the HH group contributed MSEL scores. The MSEL was not collected for three children because they were unable to be evaluated before the daylong recording was collected. MSEL scores were collected an average of 4.1 months (SD = 2.6) before the daylong recording was made. The HH group’s mean t-score was within 1 SD of the normative mean (M = 48.2, SD = 13.7, range: 20−66). The LittlEars Auditory Questionnaire (LEAQ; Kühn-Inacker et al., 2004) was also administered to HH children at the same time point. The LEAQ is a parent-report measure designed to assess the auditory behaviors of young children. HH children in the present study achieved scores indicating that the majority were demonstrating at least basic perception of environmental sounds and short phrases (n = 19, M = 31.6, Mdn = 33.0, SD = 6.3) and those values correspond to the expected values for children in the 19- to 24-month age range.
Maternal education level, categorized on a scale from 1 to 4 (1 = some high school, 2 = high school, 3 = some college, and 4 = college), was collected. Maternal education was higher in the NH group than in the HH group (z mat. ed. = 0.49, p mat. ed. = .62). Tests of differences between groups here and elsewhere are computed using the Wilcoxon signed-rank test and are reported in terms of the z-statistic (Friedman, 1937; Wilcoxon, 1945). Further examination of demographic data collected during recruitment and intake revealed no outlier data that suggest selective grouping by race, income, marital or family status, occupation, or geographical region.
In addition to the HH and NH groups, the present study results are compared to the LENA natural language study (NLS) normative sample to be described in more detail below.
Materials
The present work relies on the system developed and made available by the LENA Research Foundation (Boulder, CO). This technology consists broadly of the physical recording apparatus hardware and the associated computer software packages.
Apparatus. The self-contained LENA recording device weighs about 70g and measures about 1.3×5.6×8.6cm. It has a single microphone, two operator buttons, a monochrome display, and a USB port for data transfer and to charge the internal power supply. The recording device is activated by depressing the power button for a few seconds (to prevent accidental or child-initiated operation) followed by depressing the record button to begin recording. Technical details are given in Ford, Baer, Xu, Yapanel, and Gray (2008).
The LENA device is worn on the child’s body by inserting it into a specially designed pocket on an outer piece of clothing worn by the child. The clothing allows for the recorder to be worn comfortably and unobtrusively for the whole day while maintaining the microphone at a relatively fixed distance (7–10cm) from the child’s mouth.
Software and normative sample. The LENA device records up to 16hr of audio in encrypted format to onboard solid state memory, which is uploaded to a computer via USB connection after the recording is complete. LENA software then analyzes the audio recording using unsupervised maximum likelihood Gaussian mixture models (described in Ford et al., 2008; Oller et al., 2010). A primary goal of the analysis is to assign labels to segments of the audio file. Segments are assigned exactly one of nine primary label classes: male adult, female adult, target child, other child, noise, overlapping vocals, electronic media (e.g., TV and radio), silence, and uncertain/fuzzy. The results of the labeling procedure are reported in summary statistics accessible via a graphical user interface or may be exported to a data table for further analyses. Descriptive statistics accessible via the user interface include estimates of the numbers of adult words and conversational turns in raw value and in percentile rank (based on population estimates from the NLS sample).
Adult word estimate. The adult word count (AWC) is estimated for each segment identified as an adult talker based on analyses of specific acoustic features of the signal (see Oller et al., 2010 for a description of the acoustic parameters evaluated). The software does not attempt to segment or label specific words or word boundaries; instead, the software uses statistical models to estimate the number of words per talker segment. The sum of all segment estimates is reported as the AWC.
Conversational turns. After talkers are identified in segments as adult male, adult female, target child, etc., conversational turns are counted for exchanges between an adult and the target child with no more than 5 s of intervening nonspeech segments and no intervening speech segments of any duration from another talker (such as another adult or a nontarget child). Thus, a conversational turn is defined as the co-occurrence of adult and child speech (with either initiating) with no intervening talkers. Nonspeech segments such as noise or silence may occur between talkers, providing that they are less than 5 s in duration. All instances are summed over the course of an entire recording to produce a conversational turn count (CTC).
Reliability of adult word estimates and conversational turns. Several studies have addressed the issue of LENA software coding reliability (e.g., Christakis et al., 2009; Ford et al., 2008; Zimmerman et al., 2009). Xu et al. (2009) trained professional transcribers who analyzed and coded 70hr of audio that was recorded by the LENA system. Using these data, Christakis et al. (2009) report talker identification agreement with the LENA coding system in 67%–82% of segments with κ values in the moderate to good range, from .43 to .70.
The NLS normative database. The NLS normative database is based on the LENA NLS of 329 families contributing 2,682 twelve-hour recordings of children 2–48 months of age (Gilkerson & Richards, 2008b). All the children in the normative corpus have NH and are also otherwise typically developing. Gilkerson and Richards (2008b) give summary statistics of the education level of mothers in the families used to compute the normative sample in the NLS study. Participants in the current sample are from a more restricted age range and from homes with higher mean SES than the NLS sample. To facilitate relevant comparisons, two subsamples were compiled from the NLS study. The first subgroup, NLS-Age, was age matched and consisted of all NLS recordings of children between 25 and 36 months of age (n = 804 recordings; M = 30.2 months, SD = 3.4). The second subgroup, NLS-Age/SES, was approximately matched for both age and SES and consisted of all NLS recordings of children between 25 and 36 months of age (n = 454 recordings; M = 30.0 months, SD = 3.3) whose mothers completed some college (53%) and college (47%). In both subgroups, multiple recordings were collected from individual children at several time points, but data were not available to select individual observations. Summary characteristics for all groups considered here are given in Table 1.
The normative database produced from the NLS sample includes raw mean values and percentile ranks for AWCs and CTCs (and other variables not discussed here). Gilkerson and Richards (2008b) demonstrate that the mean and SD of CTCs increase with age up to 25 months of age and then remain steady through 48 months of age. They report that AWCs do not vary as a function of child age. Thus, normative mean and SD estimates are provided at monthly intervals for CTCs from 2 to 25 months of age. However, a single mean and SD is provided for CTCs for children 26–48 months of age and AWCs for children 2–48 months of age.
The NLS samples are fixed to a 12-hr recording duration. However, the recording duration of the samples of children reported here were variable, ranging from 8.67 to 14.60hr (M = 11.89hr, SD = 1.39). Thus, hourly rates of adult words (AWC/hr) and conversational turns (CTC/hr) were calculated for both data sets by dividing the observed daily value by the number of hours in the recording for that day. For the NLS samples, AWC/hr and CTC/hr were calculated by dividing the observed values by 12. As a result of this transformation, all groups are compared in the same terms.
Procedure
After informed consent was obtained, families were shipped the recording device, two custom shirts with a pocket to hold the recording device, paperwork including detailed instructions on device use, and return packaging. Parents were instructed to begin recording as soon as the child awoke in the morning and turn the device off when the child went to sleep for the final time in the evening, resulting in a daylong, uninterrupted recording. During times the shirt could not be worn (e.g., bath time), families were asked to place the recording device as near to the child as possible, such as on a nearby chair. Similar recording procedures were followed in previous studies with LENA hardware, including the NLS normative sample (Gilkerson & Richards, 2008b; Oller et al., 2010; Warren et al., 2010).
Results
Groups (HH, NH, NLS-Age, and NLS-Age/SES) were compared on the primary adult speech variables. The continuous dependent variables, AWCs and CTCs, are expressed in average occurrences per hour and, for the families of the HH and NH groups, as z scores with reference to the normative values of NLS-Age and NLS-Age/SES groups. Relationships of the dependent variables with SES (maternal education) and child age were considered for the HH and NH groups and, due to limited availability of data, more generally for the two NLS subgroups. Additionally, relationships between the dependent variables and the audiological variables (PTA, SII, and age at amplification) were considered for the HH group.
AWC and CTC for the Current Samples
For AWC/hr, there were no significant differences between adults in HH and NH families in the current study (M HH = 1249 AWC/hr, SD HH = 326; M NH = 1397 AWC/hr, SD NH = 386; z = 0.63, p = .526). Similarly, for CTC/hr, there were no significant differences between adults in HH and NH families in the current study (M HH = 61 CTC/hr, SD HH = 17; M NH = 66 CTC/hr, SD NH = 17; z = 0.65, p = .511).
Present Sample Compared With the Normative Sample
Because there were no significant differences between the HH and NH groups, those groups were pooled for the next analysis. For AWC/hr, adults in the NLS-Age and NLS-Age/SES groups were different from each other (M NLS-Age = 1055 AWC/hr, SD NLS-Age = 198; M NLS-Age/SES = 1164 AWC/hr, SD NLS-Age/SES = 144; z = 2.01, p < .05). For CTC/hr, adults in the NLS-Age and NLS-Age/SES groups were also different from each other (M NLS-Age = 43 CTC/hr, SD NLS-Age = 10; M NLS-Age/SES = 50 CTC/hr, SD NLS-Age/SES = 7; z = 3.02, p < .01). For AWC/hr, the pooled HH/NH group was significantly different from the NLS-Age group (z = 3.13, p < .002), but was not significantly different from the NLS-Age/SES group (z = 1.48, p = .13). For CTC/hr, the pooled HH/NH group was significantly different from both the NLS-Age and the NLS-Age/SES groups (z = 4.90, p < .001; z = 3.00, p < .003, respectively). Means and standard error of AWC/hr and CTC/hr are shown for HH, NH, NLS-Age, and NLS-Age/SES groups in Figure 1.
Figure 1 .

Adult word count (AWC) and conversational turn count (CTC) for the hard-of-hearing (HH), normal-hearing (NH), natural language study (NLS)-Age, and NLS-Age/socioeconomic status (SES) samples. Bars represent the standard error of the mean.
z Scores of AWC/hr and CTC/hr were computed for each individual in the HH and NH groups with reference to the both the NLS-Age and NLS-Age/SES groups. z Scores in the range of +1 to −1 indicate performance within the average range, with a score equal to zero indicating performance at the normative average. A z score greater than +1 or less than −1 indicates performance above or below the average range, respectively. As seen in the left panel of Figure 2, for participants in the current study compared with the NLS-Age sample, 23% (7/30) of AWC/hr scores and 40% (12/30) of CTC/hr scores were above the average range. The remaining scores were in the average range, with no individual scores below the average range. The right panel in Figure 2 shows that for participants in the current study compared with the NLS-Age/SES sample, 20% (6/30) of AWC/hr scores and 30% (9/30) of CTC/hr scores were above the average range. The majority of the remaining scores were in the average range, with a few scores falling slightly below the average range for both AWC/hr and CTC/hr.
Figure 2 .
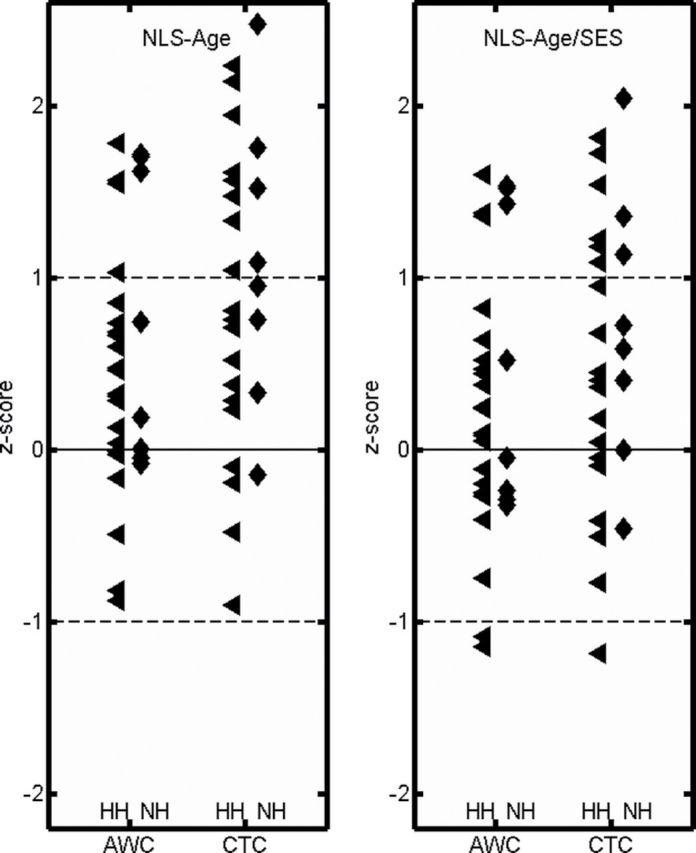
Individual z scores for adult word count and conversational turn count are shown with respect to the natural language study (NLS)-Age sample in the left panel and the NLS-Age/socioeconomic (SES) status sample in the right panel. The solid line indicates mean performance of each sample. Dashed lines indicate the range from +1 to −1 standard deviations from the NLS mean, typically understood as within the average range. Hard-of-hearing (HH) and normal-hearing (NH) children are plotted in triangle and diamond markers, respectively. AWC = adult word count; CTC = conversational turn count.
Relationships of Quantity of Adult Language With SES and Child Age
For the NH and HH groups, AWC/hr and CTC/hr were not correlated with SES (maternal education) or age of child (all ps > .5). It is possible that the lack of a correlation between SES and the dependent variables in the current study is due to a restriction in range in maternal education scores (see Table 1). For the NLS sample, Gilkerson and Richards (2008a) report significantly higher numbers of AWCs and CTCs for families with mothers who have completed college than mothers in the three categories with lower education levels.
Relationships of Quantity of Adult Language With Audiological Variables and Child Language
For the HH group, AWC/hr and CTC/hr were correlated with both unaided and aided auditory measures; PTA (r AWC = −.54, p < .01; r CTC = −.47, p < .03) and SII (r AWC = .56, p < .01; r CTC = .66, p < .01), respectively. Figure 3 shows individual participants’ PTA (upper panels) and SII (lower panels) in relation to AWC/hr (left panels) and CTC/hr (right panels).
Figure 3 .

Relationships of better ear pure tone average (PTA) and aided audibility (SII) with the two test variables, adult word count (AWC) and conversational turn count (CTC).
PTA and SII are expected to be correlated with one another, because threshold information is incorporated in both measures (Sininger, Grimes, & Christensen, 2010; Stiles et al., 2012). Children with worse PTA scores typically have worse aided SII scores, because limits of amplification prevent more audibility for greater degrees of hearing loss. As anticipated, these variables are highly correlated (r = −.93, p < .001) in the current study and likely share some degree of explained variance in AWC and CTC. However, because SII is a measure of aided hearing for speech, it may provide a more realistic index of how much access children have to adult speech than PTA, which represents unaided thresholds (see Stiles et al., 2012). To explore the possibility of unique contributions of individual auditory measures (PTA or SII), two multiple regression analyses were conducted, with AWC/hr and CTC/hr as the dependent variables in the respective models. Results of the models are summarized in Table 2. For AWC/hr, the combined effects of PTA and SII were significant (p < .02), accounting for 27.7% of the variance. However, the predictor variables did not make significant independent contributions to the explanation of AWC/hr (p > .1). For CTCs, the model also was significant (p < .01), accounting for 38.0% of the variance. Examination of the semipartial correlations revealed that the predictor variable SII made a significant independent contribution to the explanation of CTC/hr (p < .02), accounting for 21.7% of the variance after controlling for the effects of PTA in the model. The results suggest that PTA and SII make shared contributions to variance in AWC/hr but SII contributes uniquely to variance in CTC/hr.
Table 2 .
Results of simultaneous multiple regression analyses predicting adult word count and conversational turn count for the hard-of-hearing group
| Predictor | Regression 1: Adult words (R 2 = .277, p = .018) | Regression 2: Conversational turns (R 2 = .380, p = .004) | ||||||
|---|---|---|---|---|---|---|---|---|
| β | t | p | sr 2 | β | t | p | sr 2 | |
| PTA | –.273 | –0.95 | .350 | –.031 | .070 | –.26 | .793 | .002 |
| SII | .354 | 1.24 | .228 | .053 | .714 | 2.71 | .014 | .217 |
Note. sr2 is the squared semipartial correlation coefficient, which represents the percentage of variance in the criterion variable accounted for by each individual predictor variable with the other variable controlled. PTA = pure tone average; SII = speech intelligibility index.
Children with better unaided hearing (i.e., lower PTA scores) and/or better aided audibility (i.e., higher SII scores) have more access to the speech spectrum and potentially to adult language models than children with less hearing or audibility. It is possible that children with more access to adult language have the opportunity to develop stronger auditory perceptual abilities and language skills than children with less access to adult language. In turn, children’s perceptual and language abilities may influence the amount of language adults direct toward them or the number of conversational turns in which they are engaged. If so, the effects of the audiological variables may be mediated by child language abilities. To assess this possibility, mediation analyses were conducted in which PTA and SII were the independent variables, receptive language ability2 (represented by children’s MSEL scores) was tested as a mediator variable, and both AWC and CTC were treated as dependent or outcome variables (Baron & Kenny, 1986; Judd & Kenny, 1981). To proceed with mediation analysis, the initial variables (PTA and SII) must be correlated with the proposed mediator (MSEL) and with the outcome variables (AWC/hr and CTC/hr). For the subset of 19 participants with MSEL scores, MSEL scores were correlated with both PTA and SII (r PTA = −.59, p < .01; r SII = .71, p < .01). Additionally, PTA was correlated with both AWC/hr and CTC/hr (r AWC = −.61, p < .01; r CTC = −.58, p < .001) and SII was correlated with both AWC/hr and CTC/hr (r AWC = .60, p < .01; r CTC = .55, p < .02). Thus, according to Baron and Kenny (1986), the potentially mediating effect of MSEL can be examined for both PTA and SII on both AWC and CTC.
With PTA as the independent variable, the indirect and direct effects of MSEL scores were not significant for AWC or CTC (p > .05), but the total effect was significant (z AWC = −3.46, p < .01; z CTC = −2.20, p < .03). This result indicates that receptive language did not mediate the effects of PTA on AWC or CTC. With SII as the independent variable, the indirect and direct effects of MSEL scores were not significant for AWC or CTC (p > .05), but the total effect was significant (z AWC = 2.95, p < .01; z CTC = 1.89, p < .05). This result indicates that receptive language did not mediate the effects of SII on AWC or CTC. Thus, audiological variables (PTA and SII) appear to influence the outcome variables of parent language use (AWC and CTC), and these relationships are not fully explained by receptive language.
Finally, finding that receptive language ability does not mediate the audiological variables’ influence on AWC or CTC, it is of interest to examine whether receptive language ability is independently related to either AWC or CTC. The relationship between MSEL and AWC was not significant (p > .05), but the relationship between MSEL and CTC was significant (r = .62, p < .01). This result indicates that increases in children’s receptive language ability are related to increases in conversational turns, but not increased adult words.
Discussion
This study asked if young children who are HH are exposed to similar levels of adult words and conversational turns as age-matched peers with NH. Comparable performance between groups was observed for both AWC and CTC, suggesting that child hearing status had limited influence on the average quantity of parent talk around 2.5 years of age. However, for the HH group, audiological variables (PTA and SII) were associated with levels of parental talk, suggesting that parents may be sensitive to the degree to which their HH children are able to access environmental talk. Further, children with more auditory access (as measured by PTA and SII) may develop stronger auditory perceptual and receptive language abilities than children with more limited auditory access. Children’s language skills do not appear to contribute to the quantity of adult words to which they are exposed, but child language abilities are positively related to the number of conversations engaged in by parents and children.
This appears to be the first published study to use whole-day, natural recordings to explore quantitative aspects of parental talk in the homes of children who are HH. Automated analysis of the recordings proved to be a useful tool for examining characteristics of the language environment of this group. A better description of the language environment of HH children may advance the understanding of individual differences in language outcomes and the role of early interventions in promoting the most effective forms of parental talk. This study represents a preliminary step toward these objectives.
Group Comparisons: Amount of Parent Talk
Results indicated that parents of HH and NH children were similarly talkative. Parents of these children used an average of about 1,300–1,400 words per hour, which is equivalent to 15,000–17,000 words over a 12-hr period. Previous studies using automated recordings report AWCs in homes with typically developing children in a similar range, on the order of 13,000–15,400 words in a 12-hr period (Greenwood, Thiemann-Bourque, Walker, Buzhardt, & Gilkerson, 2011; Warren et al., 2010; Zimmerman et al., 2009). At first glance, the finding that parents of HH children expose their children to a similar amount of adult words as parents of children with NH appears favorable for language development; previous studies associate amount of parental talk with children’s later language skills (Hart & Risley, 1995; Hoff & Naigles, 2002; Hurtado et al., 2008; Huttenlocher et al., 1991; Tomasello & Farrar, 1984). However, similar levels of exposure to words may not equate to similar levels of access to the adult words, especially for children with hearing loss.
Interpretation of the AWC measure in relation to children with hearing loss is not straightforward. AWC is defined as an estimate of the number of adult words spoken near a child per unit of time (e.g., hour or day). AWC is calculated from those segments of the recording that the software has judged to contain “meaningful” adult speech (i.e., vocalizations by adults that are not faint or distant and that do not overlap with other speech). In essence, the AWC reflects words spoken by the adult that are conceivably within “earshot” of the child (i.e., near the microphone). However, defining what is within “earshot” of children with hearing loss is complex and may vary as a function of degree of loss, aided audibility, and characteristics of their acoustic environments (e.g., background noise). Currently, a quantitative account of language outside the audible range of the child is not possible with this technology. Due to these various factors, it has been suggested that LENA may overestimate the number of adult words that are audible to a child with hearing loss (Yoshinaga-Itano et al., 2011). This is of concern because children who are HH may require more than typical amounts of exposure due to the effects of inconsistent access to language models. Additional research is needed to explore this hypothesis.
Further, all words spoken by parents in proximity to the child’s microphone are included in the AWC measure, so both adult-to-adult talk and talk directed to the child that occur near the microphone contribute to the count. As such, the AWC is not exclusively measuring child-directed speech. Fernald and Weisleder (2011) have explored the unique contributions of child-directed talk to language learning by conducting analyses that go beyond the automated LENA analyses. The authors obtained automated recordings from 28 Latino families communicating with infants at 18 and 24 months of age. By listening to the automated recordings, the researchers separated adult utterances into mutually exclusive categories of child-directed talk and overheard talk (i.e., talk in the near environment not directed to the child). They found large individual differences in the amount and proportions of child-directed versus overheard talk in this group of families. Importantly, they also found that child-directed speech, but not overheard speech, was correlated with children’s later expressive vocabularies and language processing efficiency. Child-directed speech may be particularly important in promoting the language skills of HH children, who are likely to have more difficulty than typically developing peers in accessing talk through overhearing. These issues suggest the need to be cautious in interpreting the AWC measure and the need to empirically examine the relative influence of amount of adult-directed talk versus amount of child-directed talk on the language outcomes of children who are HH.
Group Comparisons: Number of Conversational Turns
Parents of HH children in the present study engaged their children in conversational turns at comparable levels to the parents of children with NH, with the groups averaging 60 and 67 CTC/hr, respectively. This finding is in contrast to studies that found differences in CTC frequency between parents of typically developing children and children with disabilities, including those with language delay (Oller et al., 2010) and those with autism spectrum disorders (Oller et al., 2010; Warren et al., 2010). The lack of a difference between parents of HH and NH children suggests that child hearing status did not influence the frequency of CTCs. This is an encouraging finding, given that conversations are considered prime opportunities for children to advance their language skills (Tomasello & Farrar, 1984). Speech within conversational interactions is typically child directed and may be focused on topics of interest to the child. The conversational context also is one where adults provide feedback to children on their language use, often within a context of joint attention.
Although LENA measures do not verify the presence of joint attention episodes, these are more likely to be found during conversational exchanges than in monologues. Zimmerman et al. (2009) found that the number of conversational exchanges between parents and young children was predictive of the children’s later language development. This identified relationship may be reflecting the facilitative features of joint attention and contingent responding that typically occur in conversations with young children. Given the importance of engagement in joint attention for children’s language development (Carpenter et al., 1998; Tomasello & Todd, 1983), it is positive to note that the families with HH children were similar in CTC to fairly advantaged families with age-matched NH children.
All of the HH children in the current study had access to newborn hearing screenings, modern hearing aid technology, and family intervention services. Additionally, most of the children (16/22) received their hearing aids prior to 6 months of age, which is considered relatively early. Four of the remaining children received their hearing aids within the first year of life and the final two children received their hearing aids prior to the onset of the study. Thus, the result suggesting no differences in CTCs between NH and HH groups may reflect contributions of modern hearing aid technologies and early service provision. It is interesting to note that 36% of the parents of HH children were above the average range for CTCs established by the NLS-Age sample and 27% of those parents were above the CTCs established by the NLS-Age/SES sample (see Figure 2). However, the effects of intervention in the present study are challenging to analyze, because there was not a direct measure of the intervention context, and intervention effects may be confounded by degree of hearing loss. Further research is needed to gain an understanding of the potential influence of intervention on parental language and conversational participation. Automated recordings from natural settings may be useful in pursuing these questions.
Child language abilities, including children’s responsiveness to parents’ attempts to engage them in conversations, children’s own initiations of conversations, and children’s abilities to maintain conversations, are likely to contribute to the quantity of CTCs. Similarly, HH children’s auditory perceptual abilities are expected to contribute to understanding of and responsiveness to conversational bids. Results from the LEAQ (Kühn-Inacker et al., 2004) verified that the vast majority of HH participants in this study demonstrated basic perception of short phrases, suggesting that their auditory development status was sufficient for at least simple conversational interaction. It is beyond the scope of the present paper to explore the effects of child contributions to the quantity of CTCs. However, previous research documents that children who are HH, even when early identified, demonstrate more varied early language outcomes than NH peers and some may be at risk of developing the initial lexicon at a slower rate than typically developing peers (Mayne, Yoshinaga-Itano, Sedey, & Carey, 2000; Moeller et al., 2007). Given these findings, the lack of a difference between groups in rate of CTCs is somewhat reassuring; conversations are occurring at fairly typical levels in spite of children’s auditory limitations and possible language delays. This conclusion is tentative, however, given that the automated analyses count conversational turns but do not measure qualitative aspects of conversation (e.g., parental responsiveness and contingent remarks) that are known to promote children’s language development (Bornstein, Tamis-LeMonda, & Haynes, 1999; Rollins, 2003). Furthermore, complexity of conversational talk is not reflected in the CTC measure, meaning that comparability of the groups in this regard cannot be assumed.
Comparison With Normative Samples
Parents of children in both groups reported here produced more words and engaged in more conversational exchanges than the families comprising the LENA normative study (NLS-Age). Parents in the current study were more educated, on average, than the participants in the LENA normative study. Several studies have documented differences in quantity of words parents with higher versus lower education and SES direct toward their children (Huttenlocher et al., 2007; Rowe, 2008; Rowe et al., 2005). Studies using LENA technology report similar effects, showing higher levels of talk by parents in advantaged circumstances (higher education/income) compared to those with less income or education (Gilkerson & Richards, 2008a; Warren et al., 2010; Zimmerman et al., 2009). The NLS study was based on a population sample that was designed to reflect maternal education/SES characteristics of the general U.S. population. In contrast, the participants who consented to participate in this study were biased toward higher levels of maternal education, although the researchers made every effort to recruit a representative sample. The lack of comparability of the current sample and the NLS sample has important implications for clinical practice and research. If one compares the AWC and CTC for the families in the current study to the LENA normative data (Gilkerson & Richards, 2008b), the families appear to be functioning at the 70th to 80th percentiles. This could lead service providers to conclude that an intervention program has been effective in promoting increases in parental input. However, these higher levels of adult language input could be reflecting high parental education levels (Warren et al., 2010), rather than an effect of intervention. In general, our results suggest that caution must be exercised in comparing small, unmatched samples to the NLS normative data, as the conclusions may be misleading. This extends to the need to be careful when using LENA as a clinical tool and comparing children to the normative sample.
This concern was partially confirmed by comparison of the NLS-Age sample to the NLS-Age/SES matched group. The NLS-Age/SES group had significantly higher AWCs and CTCs than the broader sample (NLS-Age), suggesting a role for SES in these measures. The results also suggest that the NLS-Age/SES subgroup provides a better comparison group for the present study. Results showed that the pooled HH/NH group was comparable to the NLS-Age/SES matched group on AWC. However, in the current study, the pooled HH/NH group had significantly higher CTCs than either of the NLS normative samples. This finding was unexpected and is challenging to explain. It may be that there are important differences between these families that are not reflected in the maternal education score. The groups were not able to be matched perfectly on SES dimensions. Further, it is possible that methodological differences between the studies (e.g., collecting samples on weekends vs. weekdays) may contribute meaningful differences that affect the results.
Individual Differences: Predictors of Parental Talk
For the HH group, regression analyses revealed that the auditory variables (PTA and SII) together accounted for a small but significant amount of variance in AWC (28%) and in CTC (38%). Both SII and PTA gave similar explanations of the AWC and CTC measures. At first glance, these findings suggest that parents talk more and engage in more conversational turns with children who have better hearing thresholds and more aided audibility than those with less hearing/audibility (see Figure 3). Although previous studies with deaf children indicate that adults make adjustments in their linguistic input in relation to hearing status and/or degree of hearing loss (Lloyd, Lieven, & Arnold, 2001; Nienhuys & Horsborough, 1984), it is unclear how applicable these findings are to early identified children who are HH. It is conceivable that parents might refrain from talking to a HH child if they are not in close enough proximity for their child to hear and understand, and this behavior may vary in relation to degree of loss and audibility factors.
It was found, however, that children with better hearing or better aided audibility also have better receptive language abilities, and stronger language abilities may allow these children to be more easily engaged in conversations. The analyses suggest that both audiological factors and child language abilities influence conversational turns. Parents might talk more to children with more sophisticated language abilities, or children with more sophisticated language abilities may elicit more interactive talk from their parents (Hoff-Ginsberg, 1994). In the current study, the contribution of hearing ability to CTCs is reasonably transparent; access to language and the frequency of engagement in conversations with others positively vary with each other for HH children.
There are several limitations to the present study that reduce its generalizability to other groups. The samples of NH and HH participants, although matched with each other, are more advantaged (maternal education) than the general population. In addition, the numbers of participants are small, especially in the NH group (n = 8), and may be influenced by family interactions on the specific day of recording. Although the full-day recordings provided robust samples of talk for all participants, their use in this preliminary study was limited to automated counts of the frequency of adult words and conversational turns. Factors such as parental provision of visual information (e.g., gesture and sign) and complexity of semantic context, for example, are not encoded by the LENA device, and those factors may be especially important for children with hearing loss. Additionally, LENA software has been extensively examined and validated, but it makes some errors in classifying speakers. However, if this biased the results in some way, both groups would be biased similarly.
Summary
This work demonstrates that whole-day recordings and automated analyses may be profitably employed to examine the natural language use of families, in particular, families with HH children. This extends the literature using large sampling acoustic recordings and automated analyses to examine the auditory environments of young children (Oller et al., 2010; Warren et al., 2010).
An important result of the present work is the lack of between-group differences in NH and HH children matched for SES. However, differences were observed between the current study sample and an NLS sample, which was matched on age but not maternal education. This study reinforces the need to cautiously interpret LENA normative data when using small, unmatched samples or when using these measures in clinical applications. This concept was supported by the finding that AWCs for the current study samples were comparable to the NLS-Age/SES sample. However, CTCs for the current study samples were higher than both NLS samples. This study also found that auditory variables (PTA and SII) were correlated with both AWC and CTC, but receptive language abilities were positively associated only with CTC, not AWC. In general, this study suggests the need for further research exploring specific ways in which the linguistic environments of HH children may be optimized to support language learning.
Funding
National Institutes of Health (NIDCD DC009560 and DC009560-01S1 to M.P.M. and J. Bruce Tomblin).
Conflicts of Interest
No conflicts of interest were reported.
Acknowledgments
The authors express appreciation to the families who participated in this research. We thank Lisa Burton, Stephanie Nielsen, Aneesha Pretto, Jaimie Horning, Wendy Fick, and Rick Arenas for data management and/or for their work with the families. We also thank J. Bruce Tomblin, PhD, and two anonymous reviewers for their comments on an earlier version of this manuscript. Helpful discussion was also contributed by Jake Oleson and Ryan McCreery, and the LENA Research Foundation kindly made data available for this project. The content of this project is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute on Deafness and Other Communication Disorders or the National Institutes of Health.
Notes
In all, 31 families contributed data. After the data for this study were collected, one participant was identified with global developmental delays, and this participant was removed from the data set and is not reported here.
There was insufficient variance in LEAQ scores due to a ceiling effect. Therefore, auditory perceptual skills were not examined as part of the regression models.
References
- Akhtar N., Jipson J., Callanan M. A. (2001). Learning words through overhearing. Child Development 72 416–430 doi:10.1111/1467-8624.00287. [DOI] [PubMed] [Google Scholar]
- ANSI (1997). Methods for calculation of the speech intelligibility index (Technical Report S3.5-1997) New York, NY: American National Standards Institute; [Google Scholar]
- ANSI (2003). Specification of hearing aid characteristics (Technical Report S3.22-2003) New York, NY: American National Standards Institute; [Google Scholar]
- Bagatto M. P., Moodie S. T., Malandrino A. C., Richert F. M., Clench D. A., Scollie S. D. (2011). The University of Western Ontario Pediatric Audiological Monitoring Protocol (UWO PedAMP) Trends in Amplification 15 57–76 doi:10.1177/1084713811420304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baron R. M., Kenny D. A. (1986). The moderator-mediator variable distinction in social psychological research: Conceptual, strategic and statistical considerations. Journal of Personality and Social Psychology 51 1173–1182 doi:10.1037/0022-3514.51.6.1173. [DOI] [PubMed] [Google Scholar]
- Belsky J., Vandell D. L., Burchinal M., Clarke-Stewart K. A., McCartney K., Owen M. T. (2007). Are there long-term effects of early child care? Child Development 78 681–701 doi:10.1111/j.1467-8624.2007.01021.x. [DOI] [PubMed] [Google Scholar]
- Bentler R., Hu Y. H., Cole B. Deriving an audibility index for frequency-lowered hearing aids. Poster presented at the American Auditory Society; Scottsdale, AZ. (2011). [Google Scholar]
- Blackwell A. A. (2005). Acquiring the English adjective lexicon: Relationships with input properties and adjectival semantic typology. Journal of Child Language 32 535–562 doi:10.1017/S0305000905006938. [DOI] [PubMed] [Google Scholar]
- Bornstein M. H., Tamis-LeMonda C. S., Haynes O. M. (1999). First words in the second year: Continuity, stability, and models of concurrent and predictive correspondence in vocabulary and verbal responsiveness across age and context. Infant Behavior and Development 22 65–85 doi:10.1016/S0163-6383(99)80006-X. [Google Scholar]
- Carpenter M., Nagell K., Tomasello M. (1998). Social cognition, joint attention, and communicative competence from 9 to 15 months of age Monographs of the Society for Research in Child Development 63 doi:10.2307/1166214. [PubMed] [Google Scholar]
- Christakis D. A., Gilkerson J., Richards J. A., Zimmerman F. J., Garrison M. M., Xu D. … Yapanel U. (2009). Audible television and decreased adult words, infant vocalizations, and conversational turns: A population-based study Archives of Pediatrics and Adolescent Medicine 163 554–558 doi:10.1001/archpediatrics.2009.61. [DOI] [PubMed] [Google Scholar]
- Cole E. B., Flexer C. A. (2008). Children with hearing loss: Developing listening and talking, birth to six (2nd ed.). San Diego, CA: Plural Publishing; [Google Scholar]
- DesJardin J. L., Ambrose S. E., Eisenberg L. S. (2009). Literacy skills in children with cochlear implants: The importance of early oral language and joint storybook reading Journal of Deaf Studies and Deaf Education 14 22–43 doi:10.1093/deafed/enn011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DesJardin J. L., Eisenberg L. S. (2007). Maternal contributions: Supporting language development in young children with cochlear implants Ear and Hearing 28 456–469 doi:10.1097/AUD.0b013e31806dc1ab. [DOI] [PubMed] [Google Scholar]
- Farran L. K., Lederberg A. R., Jackson L. A. (2009). Maternal input and lexical development: The case of deaf pre-schoolers International Journal of Language & Communication Disorders 44 145–163 doi:10.1080/13682820801973404. [DOI] [PubMed] [Google Scholar]
- Fernald A., Weisleder A. How and why early experience is so crucial in learning language. Paper presented at the LENA Users Conference; Denver, CO. (2011). [Google Scholar]
- Ford M., Baer C. T., Xu D., Yapanel U., Gray S. (2008). The LENATM language environment analysis system: Audio specifications of the DLP-0121 (Technical Report LTR-03-2). Boulder, CO: LENA Foundation; [Google Scholar]
- Fraser C., Roberts N. (1975). Mothers’ speech to children of four different ages Journal of Psycholinguistic Research 4 9–16 [DOI] [PubMed] [Google Scholar]
- Friedman M. (1937). The use of ranks to avoid the assumption of normality implicit in the analysis of variance Journal of the American Statistical Association 32 675–701 [Google Scholar]
- Gilkerson J., Richards J. A. (2008a). Gender, birth order and SES: Analyzing the natural language environment. Paper presented at the Inter Mountain Area Speech and Hearing Convention Salt Lake City, UT [Google Scholar]
- Gilkerson J., Richards J. A. (2008b). The LENA foundation natural language study (Technical Report LTR-02-2). Retrieved from: http://www.lenafoundation.org/TechReport.aspx/Natural_Language_Study/LTR-02-2
- Gilkerson J., Richards J. A. (2009). The power of talk: Impact of adult talk, conversational turns, and TV during the critical 0-4 years of child development (Technical Report LTR-01-2). Retrieved from: http://www.lenababy.com/pdf/The_Power_of_Talk.pdf
- Goodman J. C., Dale P. S., Li P. (2008). Does frequency count? Parental input and the acquisition of vocabulary Journal of Child Language 35 515–531 doi:10.1017/S0305000907008641. [DOI] [PubMed] [Google Scholar]
- Greenwood C. R., Thiemann-Bourque K., Walker D., Buzhardt J., Gilkerson J. (2011). Assessing children’s home language environments using automatic speech recognition technology Communication Disorders Quarterly 32 83 doi:10.1177/1525740110367826. [Google Scholar]
- Halpin K. S., Smith K. Y., Widen J. E., Chertoff M. E. (2010). Effects of universal newborn hearing screening on an early intervention program for children with hearing loss, birth to 3 yr of age Journal of the American Academy of Audiology 21 169–175 doi:10.3766/jaaa.21.3.5. [DOI] [PubMed] [Google Scholar]
- Hart B., Risley T. R. (1995). Meaningful differences in the everyday experience of young American children Baltimore, MD: Paul H. Brookes Publishing; [Google Scholar]
- Hart B., Risley T. R. (1999). The social world of children: Learning to talk Baltimore, MD: Paul H. Brookes Publishing; [Google Scholar]
- Hoff E. (2003). The specificity of environmental influence: Socioeconomic status affects early vocabulary development via maternal speech Child Development 74 1368–1378 doi:10.1111/1467-8624.00612. [DOI] [PubMed] [Google Scholar]
- Hoff E., Naigles L. (2002). How children use input to acquire a lexicon Child Development 73 418–433 doi:10.1111/1467-8624.00415. [DOI] [PubMed] [Google Scholar]
- Hoff-Ginsberg E. (1987). Topic relations in mother-child conversation First Language 7 145–158 doi:10.1177/ 014272378700702006. [Google Scholar]
- Hoff-Ginsberg E. (1994). Influences of mother and child on maternal talkativeness Discourse Processes 18 105–117 doi:10.1080/01638539409544886. [Google Scholar]
- Holzinger D., Fellinger J., Beitel C. (2011). Early onset of family centred intervention predicts language outcomes in children with hearing loss International Journal of Pediatric Otorhinolaryngology 75 256–260 doi:10.1016/j.ijporl.2010.11.011. [DOI] [PubMed] [Google Scholar]
- Hurtado N., Marchman V. A., Fernald A. (2008). Does input influence uptake? Links between maternal talk, processing speed and vocabulary size in Spanish learning children Developmental Science 11 31–39 doi:10.1111/j.1467-7687.2008.00768.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Huttenlocher J., Haight W., Bryk A., Seltzer M., Lyons T. (1991). Early vocabulary growth: Relation to language input and gender Developmental Psychology 27 236–248 doi:10.1037/0012-1649.27.2.236. [Google Scholar]
- Huttenlocher J., Vasilyeva M., Waterfall H. R., Vevea J. L., Hedges L. V. (2007). The varieties of speech to young children Developmental Psychology 43 1062–1083 doi:10.1037/0012-1649.43.5.1062. [DOI] [PubMed] [Google Scholar]
- Judd C. M., Kenny D. A. (1981). Process analysis: Estimating mediation in treatment evaluations Evaluation Review 5 602–619 doi:10.1177/0193841X8100500502. [Google Scholar]
- Kühn-Inacker H., Weichbold V., Tsiakpini L., Coninx S., D’Haese P., Almadin S. (2004). LittlEars auditory questionnaire Innsbruck, Austria: MED-EL; [Google Scholar]
- Lederberg A. R., Everhart V. S. (1998). Communication between deaf children and their hearing mothers: The role of language, gesture, and vocalizations Journal of Speech, Language, and Hearing Research 41 887–899 [DOI] [PubMed] [Google Scholar]
- Lederberg A. R., Everhart V. S. (2000). Conversations between deaf children and their hearing mothers: Pragmatic and dialogic characteristics Journal of Deaf Studies and Deaf Education 5 303–322 doi:10.1093/deafed/5.4.303. [DOI] [PubMed] [Google Scholar]
- Lederberg A. R., Mobley C. E. (1990). The effect of hearing impairment on the quality of attachment and mother-toddler interaction Child Development 61 1596–1604 doi:10.2307/1130767. [DOI] [PubMed] [Google Scholar]
- Lederberg A. R., Prezbindowski A. K., Spencer P. E. (2000). Word-learning skills of deaf preschoolers: The development of novel mapping and rapid word-learning strategies Child Development 71 1571–1585 doi:10.1111/1467-8624.00249. [DOI] [PubMed] [Google Scholar]
- Lederberg A. R., Spencer P. E. (2009). Word-learning abilities in deaf and hard-of-hearing preschoolers: Effect of lexicon size and language modality Journal of Deaf Studies and Deaf Education 14 44–62 doi:10.1093/deafed/enn021. [DOI] [PubMed] [Google Scholar]
- Lloyd J., Lieven E., Arnold P. (2001). Oral conversations between hearing-impaired children and their normally hearing peers and teachers First Language 21 83–107 doi:10.1177/014272370102106104. [Google Scholar]
- Mace A. L., Wallace K. L., Whan M. Q., Stelmachowicz P. G. (1991). Relevant factors in the identification of hearing loss Ear and Hearing 12 287–293 doi:10.1097/00003446-199108000-00008. [DOI] [PubMed] [Google Scholar]
- Mayne A., Yoshinaga-Itano C., Sedey A. L., Carey A. (2000). Expressive vocabulary development in infants and toddlers who are deaf or hard of hearing Volta Review 100 1–28 [Google Scholar]
- Meadow K. P. (1981). Interactions of deaf mothers and deaf preschool children: Comparisons with three other groups of deaf and hearing dyads American Annals of the Deaf 126 454–468 [DOI] [PubMed] [Google Scholar]
- Moeller M. P. (2000). Early intervention and language development in children who are deaf and hard of hearing Pediatrics 106E43. doi:10.1542/peds.106.3.e43. [DOI] [PubMed] [Google Scholar]
- Moeller M. P., Hoover B., Putman C., Arbataitis K., Bohnenkamp G., Peterson B. … Stelmachowicz P. (2007). Vocalizations of infants with hearing loss compared with infants with normal hearing: Part II—transition to words Ear and Hearing 28 628–642 doi:10.1097/AUD.0b013e31812564c9. [DOI] [PubMed] [Google Scholar]
- Mullen E. M. (1995). Mullen scales of early learning Circle Pines, MN: American Guidance Service; [Google Scholar]
- Nicholas J. G., Geers A. E. (2007). Will they catch up? The role of age at cochlear implantation in the spoken language development of children with severe to profound hearing loss. Journal of Speech, Language, and Hearing Research 50 1048–1062 doi:10.1044/1092-4388(2007/073). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nienhuys T. G., Horsborough K. M. (1984). Child variables influencing maternal speech style: Deaf and hearing children Journal of Communication Disorders 17 189–207 doi:10.1016/0021-9924(84)90011-X. [DOI] [PubMed] [Google Scholar]
- Oller D. K., Niyogi P., Gray S., Richards J. A., Gilkerson J., Xu D. … Warren S. F. (2010). Automated vocal analysis of naturalistic recordings from children with autism, language delay, and typical development Proceedings of the National Academy of Sciences 107 13354–13359 doi:10.1073/pnas.1003882107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Olsen-Fulero L. (1982). Style and stability in mother conversational behaviour: A study of individual differences Journal of Child Language 9 543–564 doi:10.1017/S0305000900004906. [DOI] [PubMed] [Google Scholar]
- Pittman A. L., Lewis D. E., Hoover B. M., Stelmachowicz P. G. (2005). Rapid word-learning in normal-hearing and hearing-impaired children: Effects of age, receptive vocabulary, and high-frequency amplification Ear and Hearing 26 619–629 doi:10.1097/01.aud.0000189921.34322.68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pressman L., Pipp-Siegel S., Yoshinaga-Itano C., Deas A. (1999). Maternal sensitivity predicts language gain in preschool children who are deaf and hard of hearing Journal of Deaf Studies and Deaf Education 4 294–304 doi:10.1093/deafed/4.4.294. [DOI] [PubMed] [Google Scholar]
- Rollins P. R. (2003). Caregivers’ contingent comments to 9-month-old infants: Relationships with later language Applied Psycholinguistics 24 221–234 doi:10.1017/S0142716403000110. [Google Scholar]
- Rowe M. L. (2008). Child-directed speech: Relation to socioeconomic status, knowledge of child development and child vocabulary skill Journal of Child Language 35 185–205 doi:10.1017/S0305000907008343. [DOI] [PubMed] [Google Scholar]
- Rowe M. L., Pan B. A., Ayoub C. (2005). Predictors of variation in maternal talk to children: A longitudinal study of low-income families Parenting 5 259–283 doi:10.1207/s15327922par0503_3. [Google Scholar]
- Schwartz R. G., Terrell B. Y. (1983). The role of input frequency in lexical acquisition Journal of Child Language 10 57–64 doi:10.1017/S0305000900005134. [DOI] [PubMed] [Google Scholar]
- Scofield J., Behrend D. A. (2011). Clarifying the role of joint attention in early word learning First Language 31 326–341 doi:10.1177/0142723710395423. [Google Scholar]
- Sininger Y. S., Grimes A., Christensen E. (2010). Auditory development in early amplified children: Factors influencing auditory-based communication outcomes in children with hearing loss Ear and Hearing 31 166–185 doi:10.1097/AUD.0b013e3181c8e7b6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sininger Y. S., Martinez A. S., Eisenberg L. S., Christensen E., Grimes A., Hu J. (2009). Newborn hearing screening speeds diagnosis and access to intervention by 20-25 months Journal of the American Academy of Audiology 20 49–57 doi:10.3766/jaaa.20.1.5. [DOI] [PubMed] [Google Scholar]
- Snow C. E. (1972). Mothers’ speech to children learning language Child Development 53 549–565 doi:10.2307/1127555. [Google Scholar]
- Spencer P. E. (1993). Communication behaviors of infants with hearing loss and their hearing mothers Journal of Speech and Hearing Research 36 311–321 [DOI] [PubMed] [Google Scholar]
- Spivak L., Sokol H., Auerbach C., Gershkovich S. (2009). Newborn hearing screening follow-up: Factors affecting hearing aid fitting by 6 months of age American Journal of Audiology 18 24–33 doi:10.1044/1059-0889(2008/08-0015). [DOI] [PubMed] [Google Scholar]
- Stein L. K., Jabaley T., Spitz R., Stoakley D., McGee T. (1990). The hearing-impaired infant: Patterns of identification and habilitation revisited Ear and Hearing 11 201–205 doi:10.1097/00003446-199006000-00006. [DOI] [PubMed] [Google Scholar]
- Stelmachowicz P. G., Pittman A. L., Hoover B. M., Lewis D. E. (2004). Novel-word learning in children with normal hearing and hearing loss Ear and Hearing 25 47–56 doi:10.1097/01.AUD.0000111258.98509.DE. [DOI] [PubMed] [Google Scholar]
- Stiles D. J., Bentler R. A., McGregor K. K. (2012). The speech intelligibility index and the pure-tone average as predictors of lexical ability in children fit with hearing aids Journal of Speech, Language, and Hearing Research. Advance online publication. doi:10.1044/1092-4388(2011/10-0264). [DOI] [PubMed] [Google Scholar]
- Tomasello M., Farrar M. J. (1984). Cognitive bases of lexical development: Object permanence and relational words Journal of Child Language 11 477–493 [DOI] [PubMed] [Google Scholar]
- Tomasello M., Farrar M. J. (1986). Joint attention and early language Child Development 57 1454–1463 doi:10.2307/1130423. [PubMed] [Google Scholar]
- Tomasello M., Todd J. (1983). Joint attention and lexical acquisition style First Language 4 197–211 doi:10.1177/014272378300401202. [Google Scholar]
- Warren S. F., Gilkerson J., Richards J. A., Oller D. K., Xu D., Yapanel U., Gray S. (2010). What automated vocal analysis reveals about the vocal production and language learning environment of young children with autism Journal of Autism and Developmental Disorders 40 555–569 doi:10.1007/s10803-009-0902-5. [DOI] [PubMed] [Google Scholar]
- Wedell-Monnig J., Lumley J. M. (1980). Child deafness and mother-child interaction Child Development 766–774 doi:10.2307/1129463. [PubMed] [Google Scholar]
- Wilcoxon F. (1945). Individual comparisons by ranking methods Biometrics Bulletin 1 80–83 [Google Scholar]
- Xu D., Yapanel U., Gray S. (2009). Reliability of the LENA Language Environment Analysis system in young children’s natural home environment. (Technical Report LTR-05-2). Retrieved from: http://www.lenafoundation.org/TechReport.aspx/Reliability/LTR-05-2
- Yoshinaga-Itano C., Gilkerson J., Cantle Moore R., Uhler K., Baca R., Wiggins M. LENA: Exploring novel approaches to language assessment and intervention. Paper presented at the Listening and Spoken Language Symposium; Washington, DC. (2011). [Google Scholar]
- Zimmerman F. J., Gilkerson J., Richards J. A., Christakis D. A., Xu D., Gray S., Yapanel U. (2009). Teaching by listening: The importance of adult-child conversations to language development Pediatrics 124 342–349 doi:10.1542/peds.2008-2267. [DOI] [PubMed] [Google Scholar]