

Summary
Background:
Persistent left superior vena cava is a rare but important congenital vascular anomaly. However, PLSVC with absent RSVC (isolated PLSVC) is a very rare venous malformation We report on a rare case of persistent left superior vena cava (PLSVC) with absent right superior vena cava (RSVC).
Case Report:
This venous malformation was identified incidentally in a 69-year-old woman during chest multi-detector computed tomography (MDCT). On chest MDCT, the SVC was noted on the left side. A bridging vein drained the right jugular and right subclavian veins and joined the left brachiocephalic vein in order to form the PLSVC, which descended on the left side of the mediastinum and drained into the left atrium (LA). The patient had no additional cardiac anomaly.
Conclusions:
Isolated PLSVC is usually asymptomatic but it can pose difficulties for establishing central venous access, pacemaker implantation and cardiothoracic surgery. This condition is also associated with an increased incidence of congenital heart disease, arrhythmias and conduction disturbances. A wide spectrum of clinicians should be aware of this anomaly, its variations and possible complications.
Keywords: vascular malformation, persistent left superior vena cava, computed tomography
Background
Persistent left superior vena cava (PLSVC) is the most common congenital malformation of the thoracic venous system and it affects about 0.3 to 0.5% of the general population [1]. The prevalence is estimated to be approximately 0.3% in individuals with a normal heart and 4.5% in individuals with congenital heart disease [1,2]. Nearly half of the patients with isolated PLSVC have other cardiac malformations, such as atrial septal defect, endocardial cushion defect or tetralogy of Fallot [2]. It is usually asymptomatic and is detected when cardiovascular imaging is performed for unrelated reasons. In this case we present a patient with isolated PLSVC draining to left atrium, diagnosed incidentally during thoracic computed tomography.
Case Report
A 69-year-old woman admitted to the clinic of chest diseases complaining of cough. After physical examination patient was referred to the radiology clinic for chest CT. A contrast-enhanced 64-row multi-detector computed tomography (MDCT) was performed. MDCT showed a bridging vein draining the right jugular and right subclavian veins; it joined the left brachiocephalic vein and formed the PLSVC, which descended at the left side of the mediastinum leftward of the pulmonary artery and left atrium (LA) before draining into the LA (Figures 1, 2). The RSVC was not present and the PLSVC drained all venous blood from the head, neck and upper extremities into the LA. Visceral organs were normally positioned. There was no lung condition detected to explain patient’s complaint and the patient was referred back to the chest diseases outpatient clinic.
Figure 1.
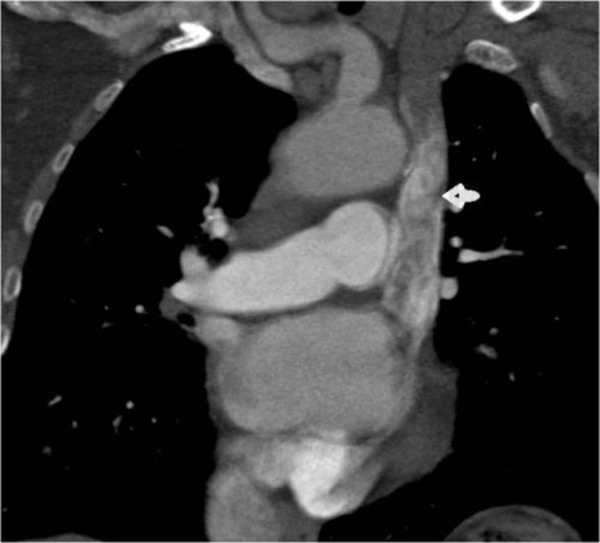
Coronal CT image shows a left superior vena cava draining into the left atrium (arrow).
Figure 2.
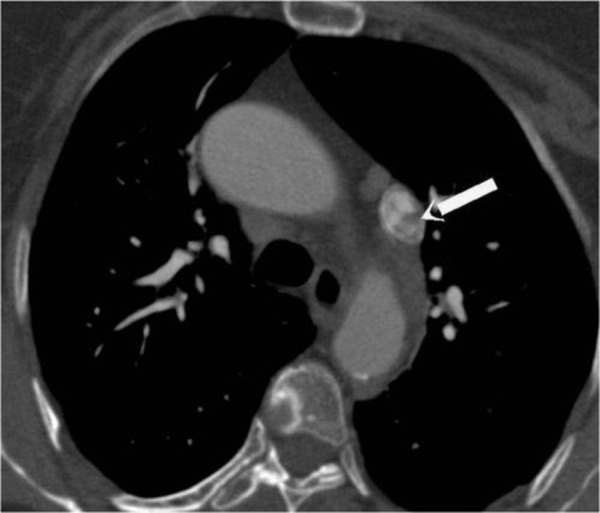
Axial CT image shows a left superior vena cava (arrow).
Discussion
Persistent left superior vena cava is a rare but important congenital vascular anomaly [1]. However, PLSVC with absent RSVC (isolated PLSVC) is a very rare venous malformation [2]. Usually, PLSVC is associated with RSVC and drains into the RA via a dilated CS (coronary sinus). If developmental arrest occurs at an earlier stage, the CS is absent and the PLSVC drains into the LA. Whether it is isolated or associated with RSVC, this venous malformation itself causes no hemodynamic disturbances and is usually diagnosed incidentally [2,3]. However, it has several clinical implications. A PLSVC can cause problems during establishing central venous access (catheterization of the CS can cause hypotension, angina, perforation of the heart, tamponade and arrest), pacemaker implantation (due to the tortuous course of the electrode, it can be difficult to fix the electrode into position and obtain stable capture), or cardiopulmonary bypass (isolated PLSVC impairs the use of retrograde cardioplegia) [4]. In 10% of patients, PLSVC may drain into the RA either directly or via an unroofed CS. This creates a right-to-left shunt and the risk of paradoxical embolism is markedly increased. In addition, drugs directly enter the systemic circulation when they are applied from the left brachiocephalic vein [2]. A final clinical implication of PLSVC (especially when isolated) is a high incidence of accompanying congenital heart defects, for example ventricular septal defect, atrial septal defect, endocardial cushion defect or tetralogy of Fallot [3,5]. Therefore associated congenital heart disease should be meticulously searched for. In the absence of an RSVC, central venous access should be made through the femoral vein in patients with PLSVC. During right-sided, open-heart surgical procedures PLSVC has to be drained by inserting a separate cannula into it. If the PLSVC drains into the LA and creates a large right-to-left shunt, surgical correction should be performed. Again, central venous access via the femoral vein is a safer choice in case of this anatomical variation. When implanting permanent pacemakers, the left subclavian vein is preferred, as lead manipulation is easier. There is an acute angle between the CS ostium and the tricuspid valve, therefore the lead should be looped in the RA in order to enter the right ventricle [6]. Hand-shaped stylets and active fixation leads are also helpful in overcoming technical difficulties [6,7]. Finally, a wide spectrum of clinicians (radiologists, sonographers, interventional and intensive care specialists, anaesthesiologists, cardiothoracic surgeons) should be aware of PLSVC and its variations in order to avoid possible complications.
References:
- 1.Buirski G, Jordan SC, Joffe HS, et al. Superior vena caval abnormalities: Their occurrence rate, associated cardiac abnormalities and angiographic classification in a paediatric population with congenital heart disease. Clin Radiol. 1986;37:131–38. doi: 10.1016/s0009-9260(86)80382-8. [DOI] [PubMed] [Google Scholar]
- 2.Sarodia B, Stoller J. Persistent left superior vena cava: case report and literature review. Respir Care. 2000;45(4):411–16. [PubMed] [Google Scholar]
- 3.Perloff JK. The Clinical Recognition of Congenital Heart Disease. 4th ed. Philadelphia: WB Saunders Company; 1994. Congenital anomalies of vena caval connection; pp. 703–14. [Google Scholar]
- 4.Birnie D, Tang AS. Permanent pacing from a left ventricular vein in a patient with persistent left and absent right superior vena cava. Pacing Clin Electrophysiol. 2000;23:2135–37. doi: 10.1111/j.1540-8159.2000.tb00790.x. [DOI] [PubMed] [Google Scholar]
- 5.Webb WR, Gamsu G, Speckman JM, et al. Computed tomographic demonstration of mediastinal venous anomalies. AJR Am J Roentgenol. 1982;139:157–61. doi: 10.2214/ajr.139.1.157. [DOI] [PubMed] [Google Scholar]
- 6.Rose M, Gross L, Protos A. Transvenous pacemaker implantation by way of an anomalous left superior vena cava. J Thorac Cardiovasc Surg. 1971;62(6):965–66. [PubMed] [Google Scholar]
- 7.Meijboom W, Vanderheyden M. Biventricular pacing and persistent left superior vena cava. Case report and review of the literature. Acta Cardiol. 2002;57(4):287–90. doi: 10.2143/AC.57.4.2005428. [DOI] [PubMed] [Google Scholar]