

Summary
Background:
Takayasu arteritis is an inflammatory disease of large-diameter arteries. Aorta and its branches are most frequently affected. Takayasu arteritis occurs mainly in young women and, if left untreated, leads to fatal complications. Digital subtraction angiography (DSA) is considered the gold standard in imaging of Takayasu arteritis.
Case Report:
A thirty-five-year-old woman was admitted to the hospital with transient loss of consciousness, effort-associated vertigo, upper limb weakness and temporary vision problems. On admission, there was no pulse on the left radial artery while there were bruits over subclavian arteries. Imaging of the aortic arch (computed tomography angiography, DSA) revealed stenoses of its main branches, indicating Takayasu arteritis.
Conclusions:
Computed tomography angiography (CTA) performed with a 64-slice unit revealed high effectiveness in localization of vascular wall and lumen pathologies resulting from Takayasu arteritis. Thanks to this fast diagnostic method, it is now possible to perform successful monitoring of patients with Takayasu arteritis and to plan possible interventional treatment.
Keywords: Takayasu arteritis, computed tomography angiography (CTA), digital subtraction angiography (DSA)
Background
Takayasu arteritis, also known as “pulseless disease” or Martorell syndrome, is a chronic inflammatory disease of large arteries. The name comes from a Japanese ophthalmologist, Mikito Takayasu, who described characteristic symptoms of this disease in 1908 [1].
Etiology of this disorder is unknown, but its background is most likely autommunological. It begins with formation of inflammatory infiltrates in tunica adventitia and vasa vasorum. Subsequently, the process involves the middle layer of a vascular wall, leading to proliferation of fibrous connective tissue. At a later stage, it leads to hypertrophy of tunica intima. Narrowing of vascular lumen and blood flow disruption appear as a consequence of changes taking place throughout all layers of the vascular wall (panarteritis). In the chronic phase, vascular wall becomes fibrotic and calcified. Symptomatology of the disease may vary depending on localization of vascular lesions, e.g. impaired cerebral blood flow may be a sign of involvement of arteries supplying the head [1–4].
Conservative treatment of Takayasu arteritis consists of corticosteroids or immunosuppressants. Therapy should be supplemented with oral anticoagulants. Surgical, including endovascular, treatment should be commenced in order to prevent severe complications [3,4].
Case Report
A 35-year-old woman was hospitalized due to a short-lasting episode of syncope. In her medical history, she reported upper limb weakness and vertigo on exertion. Moreover, she reported low blood pressure on both arms in manual measurements. She complained of periodically blurred vision.
On admission, patient was in good general condition, with good logical contact, oriented to person, time and space. In physical examination, we found weak pulse on the right radial artery and absence of pulse on the left side. Bruit could be heard over the right cervical artery and bilaterally over the subclavian arteries.
Apart from microcytic anemia (Hb 9.2 g/dl, MCV 76.1 fl), laboratory studies revealed the presence of elevated inflammatory markers (OB 57 mm/h, hsCRP 55.53 mg/l, fibrinogen 6.9 g/l).
Color Doppler ultrasonography (CDUS) examination of cephalad arteries visualized bilateral, concentric, hypoechogenic thickening of proximal common carotid artery (CCA) walls causing a >75% stenosis and elevated flow rates. The right vessel was 12 mm in diameter; its canal was 2.4 mm and wall thickness was 4.8 mm. On the left side, vessel diameter was 10 mm, its canal was 2.8 mm and wall thickness was 4 mm. There was turbulent flow noted in the distal parts of CCA. Internal and external carotid arteries were unremarkable bilaterally. A 50–75% stenosis of brachiocephalic trunk was also visualized. On the left side, we noted narrowed arterial canal in the proximal part of subclavian artery and its occlusion distally to the point of origin of vertebral artery.
Computed tomography angiography (CTA) of thoracic aorta demonstrated narrowing of aortic lumen in the aortic arch area. Lumen diameter was 27 mm and vascular wall was thickened to 5 mm. In the descending part, aortic lumen was 20 mm wide. Wall of the brachiocephalic trunk was thickened to 6 mm and its lumen in the proximal part was 4 mm in diameter. Stenosis of the trunk extended beyond the origin of right CCA, which was critically narrowed at a 17-mm distance and exhibited concentric wall thickening. Similarly, the left CCA was critically stenosed in the proximal part, at a 43-mm distance, with a 4-mm-thick wall (Figure 1). We noted a 19-mm-long proximal left subclavian artery occlusion.
Figure 1.
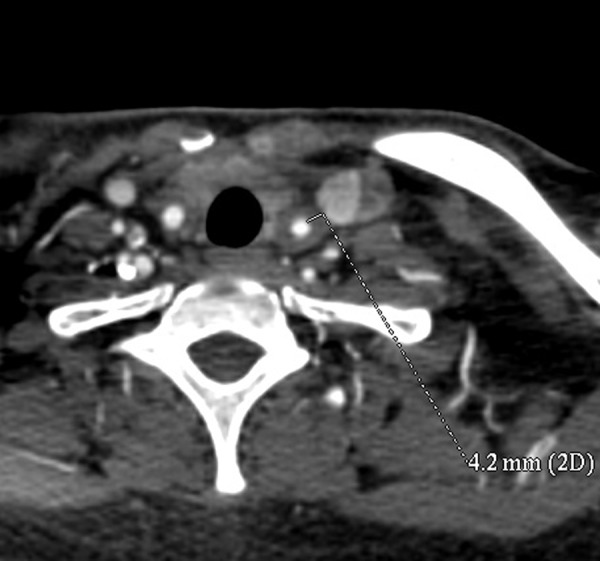
CTA of cephalad arteries visualized critical stenosis of the proximal left CCA caused by thickening of vascular wall to 4 mm.
Patient received treatment with pulses of methylprednizolone at four-week intervals, together with long-term prednizone therapy (with intention to tamper the doses) and acetylsalicilic acid. During the following 6 months we observed gradual regression of changes noted in CDUS, reduction of left CCA wall thickness to 2 mm, normalization of ESR (6 mm/h) and hsCRP (0.1 mg/l) levels.
Before the planned sixth pulse of steroids, patient suffered from an ischemic stroke with right-sided hemiparesis and motor aphasia. We decided to administer another pulse of methylprednizolone, after which we observed gradual improvement of patient’s neurological state. Repeated CDUS examination of cephalad arteries showed left CCA occlusion without signs of wall thickness progression. In order to verify the ultrasound image, we broadened the diagnostics by CTA, which confirmed regression of wall thickness of involved vessels (most likely an effect of corticosteroid treatment), but also revealed length-wise progression of critical stenosis in the left CCA from 43 to 58 mm (Figure 2A, B).
Figure 2.

(A) Baseline CTA of cephalad arteries showed a 43-mm-long critical stenosis of left CCA. (B) Follow-up CTA of cephalad arteries performed after an ischemic stroke incident visualized lengthwise progression of left CCA critical stenosis from 43 to 58 mm.
A digital subtraction angiography (DSA) was performed in order to plan potential endovascular treatment. It showed a long fragment of critical left CCA stenosis (Figure 3).
Figure 3.
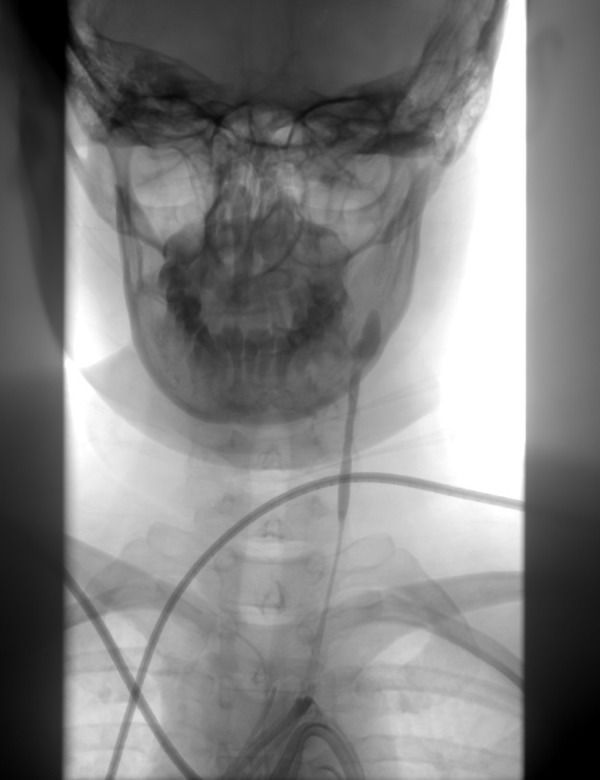
Selective DSA of left CCA showed a long, critical stenosis in the proximal part of the artery.
When inflammatory process subsided, we considered revascularization therapy. Patient was consulted with several national and foreign vascular centers. One of them accepted her for surgical revascularization of cephalad vessels. Family reported that the patient had suffered an extensive, left-sided hemorrhagic stroke on the second day after aorto-carotid bypass surgery, resulting in her death.
Discussion
Takayasu disease is a large-vessel arteritis of unknown etiology, rarely encountered in Europe. The disease involves aorta and its branches, rarely including pulmonary or smaller arteries (e.g. coronary). The time from first clinical symptoms to diagnosis varies and is usually 2 to 36 months (mean 24 months) [1,2,4].
The disease is most prevalent in women aged 15–40 years. The greatest incidence was observed in Japan – 30 cases per million per year compared to 1–3 cases per million per year in Europe and North America. Female-to-male ratio in Japan is 8:1, in America 3:1, while in India it is 1.6:1 [2–5].
Takayasu arteritis presents with diverse symptomatology, although it may be asymptomatic for a long time. It can be divided depending on the duration of illness. In the initial period, there are non-specific, general symptoms resulting from an inflammatory state (e.g. fever, fatigue, headaches and dizziness). Subsequently, symptoms associated with disruption of blood flow through narrowed vessels may appear, including blurry vision, syncope, convulsions, limb pain on exertion, postprandial abdominal pain. In the chronic phase of the disease, accompanied by weight loss, symptoms result from complete occlusion of vascular lumen or its critical stenosis, which may cause an ischemic stroke, retinopathy, secondary renovascular hypertension, myocardial infarction, limb and intestinal ischemia. Some patients may present with anemia and hyperglobulinemia. Elevation of inflammatory markers such as CRP and ESR is not pathognomonic for this disease, but may be a marker of its activity [1,3,4,6].
Takayasu disease should be differentiated with giant cell arteritis (GCA), also known as Horton’s disease or temporal arteritis. GCA, similar to Takayasu disease, is more prevalent in women, but it is most frequent in the age group >50 years old and most often involves temporal, vertebral, posterior ciliary or ophthalmic arteries. Main symptoms involve blurry vision, new-onset pain in the temporal region with erythema and tenderness, balance disturbances and general symptoms of systemic inflammation. The gold standard of diagnosis of GCA is ultrasound-guided temporal artery biopsy. CTA or MRA imaging may aid in the diagnosis [7,8].
Clinical diagnosis of Takayasu disease is based on ACR (American College of Rheumatology) or Ishikawa criteria. Patient age (<40 years) is the most important criterion in both groups [2,4,5]. Separate ACR criteria for Takayasu disease and GCA allow for clinical differentiation between those two disorders. Our patient fulfilled all ACR and Ishikawa criteria necessary for clinical diagnosis of Takayasu disease.
According to Andrews et al., 5-year survival index in Takayasu disease is 65% [2], while Maffei et al. reports it at 91% and 10-year-survival at 84% [4]. Phillip and Luqmani report 5-year survival in Takayasu disease at a 70–93% level [9]. However, we must remember that prognosis depends on the type of disease.
According to the literature, indications for endovascular treatment are: hypertension associated with renal artery stenosis, severe intermittent claudication, brain ischemia or critical stenosis of at least three cephalad arteries, ischemic heart disease with coronary lesions and aortic regurgitation. All of the above indications must be confirmed with imaging studies. One must remember that effectiveness of interventional therapy depends on first-line administration of pharmacological therapy in order to reduce the levels of inflammatory markers and stabilize disease activity [2,5]. Radiological imaging should be performed both before and after endovascular treatment for identification of arterial lesions.
Nasu (1975) and Numano (1994) introduced radiological classification of Takayasu disease depending on localization of lesions in the aorta and its branches (Table 1) [10,11].
Table 1.
Comparison of radiological classifications of Takayasu disease according to Nasu and Numano. In Numano classification coronary or pulmonary artery involvement should be marked respectively as C(+) or P(+).
| Type | Nasu (1975) | Numano (1994) |
|---|---|---|
| I | Aortic arch and branches | Branches of aortic arch |
| II | Descending thoracic and abdominal aorta with branches |
|
| III | Entire aorta with branches | Descending thoracic and abdominal aorta and/or renal arteries |
| IV | Any part of aorta and pulmonary arteries | Abdominal aorta and/or renal arteries |
| V | Selected aortic segment and/or its branches |
Narrowing of aortic branches originating at the arch of the aorta confirmed the diagnosis of type I (acc. to Nasu) or type IIb (acc. to Numano) Takayasu disease in our patient.
To date, Takayasu disease was diagnosed with classical or digital angiography (DSA), which allows for accurate assessment of vessel morphology and lumen, without taking into account wall thickness and architecture. A great advantage of this method is the possibility of precise planning of endovascular treatment. However, patient is exposed to greater amount of ionizing radiation compared to computed tomography. Intra-arterial angiography is an effective modality and is considered the gold diagnostic standard in this disease but, due to its invasiveness, it is burdened with high risk of complications (e.g. thromboembolic incidents, dissection of arterial wall). One should remember about frequent false-negative results in patients at early stages of the disease as well as difficulties in imaging of vascular segments distal to the stenosis [3,6,8,11,12].
Color Doppler ultrasonography (CDUS) examination is a widely available and non-invasive diagnostic method. This modality allows to identify the presence of stenosis and estimate blood flow, facilitates evaluation of morphology of vessels available for assessment. The test is cheap and painless, although it may be impossible to perform in some patients due to technical reasons (e.g. due to bowel gasses, obesity, ascites, peritoneal signs). A variant of Takayasu involving the arch of aorta is poorly accessible in CDUS imaging. Transesophageal echocardiography (TEE) is an alternative way of thoracic vessel imaging [3,4,6,12–15]. In the described case, due to the limitation of this method and difficulties concerning accurate comparison of various CDUS imaging studies, we failed to visualize the progression of vascular lesions, which was clearly visible in CTA.
Magnetic resonance is another examination for visualizing vascular lumen and into vessel walls. It may be performed using two techniques. The first technique is a two-dimensional TOF (time-of-flight) without contrast, which enables imaging of high-flow vessels (before stricture), while low-flow vessels (segments distal to the stricture) are poorly visible. The second method is three-dimensional MR angiography (MRA) with application of gadolinium contrast. Performing MRA with gadolinium facilitates demonstration of pathological wall enhancement in T1-weighted images, although correlation of these lesions with disease activity is questionable and requires further studies in light of the fact that wall enhancement may be a physiological sign of angiogenesis. Edema is a sign of inflammation and it is possible to visualize in T2-weighted images. However, according to Pipitone et al. wall edema is not correlated with disease progression, as some patients presented with progression of vascular lesions without accompanying edema [7]. In comparison to CTA, this modality is characterized by considerably weaker contrast between vascular wall and surrounding tissue as well as inability to identify calcifications within artery walls. This method is time-consuming and expensive, its results may be affected by movement artifacts (necessity of sedation in case of children) or presence of ferromagnetic materials in patient’s body (e.g. stents, implantable cardioverter). Additional disadvantage of this method is related to the fact that a unit with magnetic field strength of 3 Tesla is required for small-caliber vessel imaging, which is difficult to obtain. Because of the above-mentioned reasons, utilization of MR for diagnosis and monitoring of patients with Takayasu disease is difficult and limited to a few centers [3,6,10,13–16].
Because of the presence of ongoing active vascular inflammation, scintygraphy may be a potentially useful method of disease monitoring. However, due to its low resolution it is currently not applicable to functional imaging of vessels [10,16]. Positron emission tomography (PET) with radiolabelled glucose (18FDG) allows for assessment of metabolic activity of vascular wall, which in turn facilitates diagnosis before the appearance of morphological changes within arterial wall. Glucose uptake by the vascular wall is described according to a 4-point scale: no uptake (0), less than liver uptake (1), similar to liver uptake (2), greater than liver uptake (3), where grades 2–3 are associated with vasculitis. However, this modality is very expensive, poorly accessible and its diagnostic use in Takayasu disease is questionable due to absence of characteristic signs in early stages of the disease. PET may be potentially utilized for monitoring of vasculitis (disease activity) in patients with diagnosed Takayasu disease. However, as demonstrated by Yun et al., proper interpretation of this test can be hindered by the fact that observed arterial changes may be due to physiological modeling of vascular wall or age-related artery disease (e.g. atherosclerosis) instead of ongoing inflammatory process. Although it is an imaging modality, it does not bring any information regarding the anatomy of the studied vessel. Moreover, PET exposes patient to significant radiation and may be only used for evaluation of vessels larger than 4 mm in diameter, which constitutes another limitation [7,12,16–18].
Currently, computed tomography angiography (CTA) plays an increasingly larger role in diagnosis of Takayasu disease, especially since introduction of multi-slice, high (submillimeter) spacial resolution CT devices with excellent vascular contrast. Possibility to accurately compare various studies performed at time intervals and in various stages of the disease is an advantage of CTA (repeatability of assessment of vascular wall morphology). According to Khendelwal et al., CTA is characterized by a 95% sensitivity, 100% specificity and 96% accuracy in diagnostics of Takayasu disease [6]. Main benefits of CTA include short study time and minimal invasiveness. On the other hand, it has disadvantages such as exposure to ionizing radiation (lower dose compared to angiography) and risk of iodine contrast allergy or contrast-induced nephropathy. It should be also mentioned that the study might be diagnostically useless if contrast is distributed too early or too late in relation to the scanning time. Acquired vessel images are of high quality, enabling assessment of arterial wall thickness and long-axis vessel reconstruction for evaluation of the extent of excentric wall thickening, both proximally and distally to the stricture. Additional advantage of this method involves planning of interventional treatment and predicting disease progression through detection of minimal vascular changes as well as assessing prognosis with regard to high-risk small vessels, which is not possible in case of PET imaging. CTA enables early diagnosis of Takayasu disease. Due to inflammation, vascular wall undergoes contrast enhancement, which is referred to as a “double ring” (poorly enhanced internal ring corresponding to edema of tunica intima and strongly enhanced external ring corresponding to inflammation of tunica media and adventitia). CTA is particularly useful in the elderly, as it allows for differentiation between inflammatory and degenerative (e.g. calcifications) lesions, which may give false positive results in PET study. Moreover, it enables assessment of patient reaction to pharmacological treatment and quick diagnosis of late complications (e.g. critical stenosis of cephalad arteries). Also, correlation between levels of inflammatory markers and CTA images allows for effective evaluation of disease activity [3,6–8,10,12–14,19].
Conclusions
Multi-slice CTA allows for quick and precise diagnostic imaging in vascular diseases, enables accurate follow-up of vascular wall morphology and width of vascular canal regardless of localization of lesions.
CTA enables precise planning of interventional treatment and monitoring of patients’ response to treatment.
References:
- 1.Numano F. The story of Takayasu arteritis. Rheumatology. 2002;41:103–6. doi: 10.1093/rheumatology/41.1.103. [DOI] [PubMed] [Google Scholar]
- 2.Andrews J, Mason JC. Takayasu’s arteritis – recent advances in imaging offer promise. Rheumatology. 2007;46:6–15. doi: 10.1093/rheumatology/kel323. [DOI] [PubMed] [Google Scholar]
- 3.Gotway MB, Araoz PA, Macedo TA, et al. Imaging Findings in Takayasu’s Arteritis. AJR. 2005;184:1945–50. doi: 10.2214/ajr.184.6.01841945. [DOI] [PubMed] [Google Scholar]
- 4.Maffei S, Di Renzo M, Bova G, et al. Takayasu’s Arteritis: a review of the literature. Intern Emerg Med. 2006;1(2):105–12. doi: 10.1007/BF02936534. [DOI] [PubMed] [Google Scholar]
- 5.Zalewska J, Ignaczak P, Bilińska-Reszkowska H, et al. Choroba Takayasu. Reumatologia. 2009;47(6):376–80. [Google Scholar]
- 6.Khandelwal N, Kalra N, Garg MK, et al. Multidetector CT angiography in Takayasu arteritis. Eur J Radiol. 2011;77(2):369–74. doi: 10.1016/j.ejrad.2009.08.001. [DOI] [PubMed] [Google Scholar]
- 7.Pipitone N, Versari A, Salvarani C. Role of imaging studies in the diagnosis and follow-up of large-vessel vasculitis: an update. Rheumatology. 2008;47:403–8. doi: 10.1093/rheumatology/kem379. [DOI] [PubMed] [Google Scholar]
- 8.Restrepo CS, Ocazionez D, Suri R, et al. Imaging Spectrum of the Infectious and Inflammatory Conditions of the Aorta. RadioGraphics. 2011;31:435–51. doi: 10.1148/rg.312105069. [DOI] [PubMed] [Google Scholar]
- 9.Phillip R, Luqmani R. Mortality in systemic vasculitis: a systematic review. Clin Exp Rheumatol. 2008;26:94–104. [PubMed] [Google Scholar]
- 10.Nastri MV, Baptista LPS, Baroni RH, et al. Gadolinium-enhanced Three-dimensional MR Angiography of Takayasu Arteritis. RadioGraphics. 2004;24:773–86. doi: 10.1148/rg.243035096. [DOI] [PubMed] [Google Scholar]
- 11.Nasu T. Takayasu’s truncoarteritis in Japan. Pathol Microbiol. 1975;43:140–46. [PubMed] [Google Scholar]
- 12.Mishra A, Bhaktarahalli JN, Ehtuish EF. Takayasu arteritis diagnosed by 16-row multidetector CT angiography. Neurosciences. 2007;12(1):73–75. [PubMed] [Google Scholar]
- 13.Waliszewska M, Jakubiak A, Guziński M, et al. Application of the 64-slice computed tomography as a diagnostic method in acute posttraumatic ischemia of the upper limbs – 3 case reports. Pol J Radiol. 2010;75(2):94–97. [PMC free article] [PubMed] [Google Scholar]
- 14.Jakubiak A, Waliszewska M, Guziński M, et al. The value of 64-detector computed tomography angiography as a diagnostic method during emergency service in acute lower limbs ischemia. Pol J Radiol. 2009;74(3):37–41. [Google Scholar]
- 15.Canyigit M, Peynircioglu B, Hazirolan T, et al. Imaging Characteristics of Takayasu Arteritis. Cardiovasc Intervent Radiol. 2007;30:711–18. doi: 10.1007/s00270-007-9050-5. [DOI] [PubMed] [Google Scholar]
- 16.Gotthardt M, Bleeker-Rovers CP, Boerman OC, et al. Imaging of Inflammation by PET, Conventional Scintygraphy, and Other Imaging Techniques. J Nucl Med. 2010;51:1937–49. doi: 10.2967/jnumed.110.076232. [DOI] [PubMed] [Google Scholar]
- 17.Kobayashi Y, Ishii K, Oda K, et al. Aortic Wall Inframmation Due to Takayasu Arteritis Imaged with 18F-FDG PET Coregistered with Enhanced CT. J Nucl Med. 2005;46:917–22. [PubMed] [Google Scholar]
- 18.Yun M, Yeh D, Araujo LI, et al. F-18 FDG uptake in the large arteries: a new observation. Clin Nucl Med. 2001;26:314–19. doi: 10.1097/00003072-200104000-00007. [DOI] [PubMed] [Google Scholar]
- 19.Baran B, Kornafel O, Guziński M, et al. Dolichoectasia of the circle of Willis arteries and fusiform aneurysm of basilar artery – case report and review of the literature. Pol J Radiol. 2012;77(2):54–59. doi: 10.12659/pjr.882971. [DOI] [PMC free article] [PubMed] [Google Scholar]