

Abstract
Background:
Benign paroxysmal positional vertigo (BPPV) is a mechanical peripheral vestibular disorder which may involve any of the three semicircular canals but principally the posterior. In as much as the literature has described theories to explain the mechanism of BPPV and also contains scholarly works that elucidate BPPV; its management remains an enigma to most clinicians. To this end, this work was aimed at outlining an evidence-based best practice for most common form of BPPV.
Materials and Methods:
A systematic review of the literature was conducted between 1948 and June 2011 in PubMed, Embase, Ovid, and Cochrane database through the online Library of the University of Cape Town. Seventy-nine worthy articles that addressed the study were selected on consensus of the two authors.
Conclusion:
There is consensus for the use of canalith repositioning procedures as the best form of treatment for posterior canal canalolithiasis. However, successful treatment is dependent on accurate identification of the implicated canal and the form of lithiasis. Furthermore, clinicians should note that there is no place for pharmacological treatment of BPPV; unless it is to facilitate repositioning.
Keywords: Benign paroxysmal positional vertigo, canalith repositioning procedures, canalolithiasis, cupulolithiasis, nystagmus, vertigo
INTRODUCTION
Benign paroxysmal positioning vertigo (BPPV) is a peripheral vestibular disorder involving the semicircular canal usually but not exclusively the posterior semicircular canal (PSCC). Involvement of the lateral (LSCC) and superior (SSCC) semicircular canal has also been described. BPPV, with its characteristic, short-duration vertigo and accompanying nystagmus is provoked by critical provocative movements of the head relative to gravity, often lying down or turning over in bed. Indeed, if the word “bed” comes into the case history, the clinician should always consider BPPV. It should be noted that up to one third of patients will present with an atypical history, so all dizzy patients should undergo provocative positioning. In spite of the site of lesion being in the end-organ, BPPV is not associated with hearing loss or tinnitus; nor are there worrying neurologic symptoms.
Historically, Barany1 was the first to describe BPPV in a female patient, nine decades ago with typical representation of the above features. He simply attributed his observation to the malfunction of the otolith organ. However, the details in the diagnosis were later defined by Dix and Hallpike2 (Dix-Hallpike maneouvre) in 1952. Subsequently, efforts at better understanding the pathogenesis and management of the disease were made by Schuknecht3,4 and others, including Epley.5–9 Essentially, these authors outlined the cupulolithiasis theory, which prompted the first efforts at physiotherapeutic treatment; and then the canalolithiasis theory, which also resulted in new techniques aimed at repositioning.
Despite the scholarly contributions in elucidating BPPV, clinicians still find the management challenging and sometimes indulge in dogmatic practices essentially nonbeneficial to the patients. Following the foregoing, this work is focused on outlining the scientific-based best practices for the treatment of the most commonly encountered class of BPPV.
MATERIALS AND METHODS
The search strategy
A comprehensive literature search in PubMed, Embase, Ovid and the Cochrane data base were conducted (1948–June 2011) using the MeSH words “Benign paroxysmal positional vertigo” “Posterior vestibular canal” “Vertigo” and “management” combined in various modes. The initial hit for MEDLINE search yielded 975 and Cochrane library 19 articles. The two authors assessed the articles independently and selected 61 that were considered relevant to the study. A cross referencing of the articles yielded an additional 18 articles. Full articles were retrieved via the online library of the University of Cape Town.
Inclusion/exclusion criteria
All original and quality review articles that addressed one or more of these: “historical background,” “Epidemiology,” “pathopysiology” and “management” of the posterior canal BPPV were included. Quality illustrations were adapted following written permission from the publishers, whereas all animal studies (except for reference purposes) and Letters to the Editor were excluded.
Epidemiology
BPPV has been described as the most commonly diagnosed vestibular disorder with a life time prevalence of about 2.4%.10–13 It is possible that this may be an under estimation due to unreported cases of sporadic BPPV that resolve spontaneously. There is no evidence-based racial bias; however, there is a strong suggestion of female preponderance14,15 and predilection for older age group (5th and 6th decades of life). It is rare in childhood and those aged less than 35 years except for cases of BPPV associated with head trauma.16–18
Classification
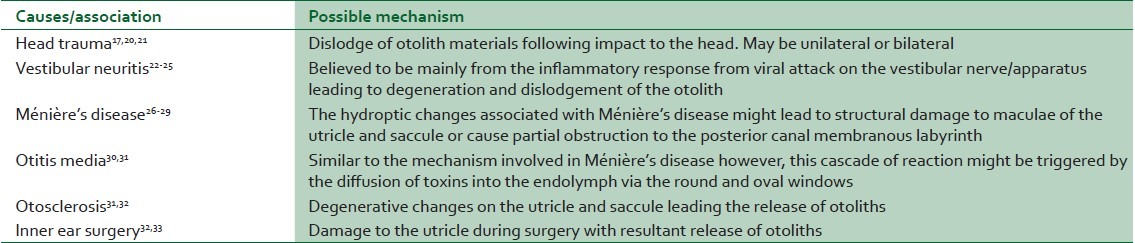
The classification of BPPV can be based on the anatomical location or the etiology. The most commonly involved semicircular canal is posterior, occasionally lateral canal and rarely the superior canal. Research from Korres and colleagues19 produced a typical distribution of implicated canals in 122 cases of diagnosed BPPV with 90% posterior, 8% lateral and 2% superior. LSSC BPPV may occur either with or without PSSC involvement and most often results from severe head trauma.17,20 However, as the type of BPPV that clinicians are most likely to encounter is in the PSSC, the focus of the discussion will be on this form. Primary or idiopathic BPPV is of unknown cause and by far the more common (about 50%–70%) presentation. In contrast, secondary BPPV is of established causes, as illustrated in Table 1.
Table 1.
Etio-pathological associations of secondary benign paroxysmal positioning vertigo
Pathogenesis of BPPV
In an attempt to explain the pathogenesis of BPPV, there is need for a brief description of the anatomical structure and spatial orientation of the vestibular organ [Figure 1].
Figure 1.
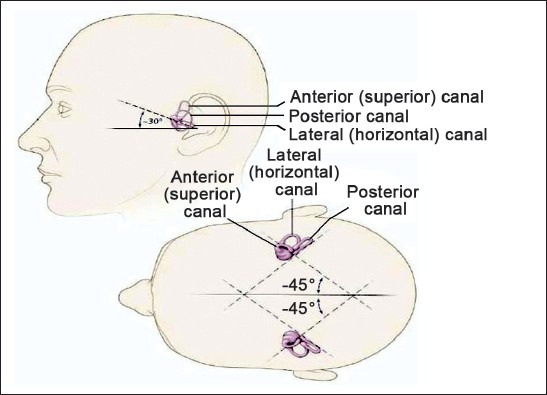
Schematic diagram of the vestibular system showing the anatomical and spatial orientation of the semi-circular canals relative to the head. (Adapted from Ref. 22 and reproduced with permission from Dr. L.S. Parnes parnes@uwo.ca)
The three semicircular canals are the LSSC (horizontal), PSSC, and SSCC. They lie in perpendicular (right angle) planes to one another thus representing the three dimensional spatial orientation, and sub serves for the angular acceleration. Each is encased in the bony labyrinth, and has a dilated anterior end (the ampulla) containing the patch of neuro-epithelium known as crista. The hair cell of the crista is embedded within the overlying gelatinous cupula and is displaced by the movement of the endolymph. The nonampullated ends of the posterior and superior canals fuse into a common channel (crus commune).Thus the three canals open into the vestibule via five openings specifically into the utricle which lies within the bony vestibule and communicates with the saccule through the utriculosaccular duct. Both the utricle and the saccule contain sensory elements called macula which sub serves for linear acceleration and deceleration. The details of the functional anatomy of the vestibular system could be obtained from standard otoneurology text books.34
Two main theories, namely cupulolithiasis and canalolithiasis have been propounded over time in an attempt to explain the pathogenesis of BPPV.
(a) Cupulolithiasis theory: This marked the first attempt by Schuknecht at explaining the phenomenon of BPPV in 1969.4 He opined that the degeneration of the utricular otolithic membrane occurs following trauma, ischemia, infections, and other insults of the vestibular organ which results in the release of “otoconia” which gets deposited at the PSSC. This alters the specific gravity of cupula thus converting it to a gravity receptor and thereby provoking a rotatory nystagmus on rapid change of the head position.
(b) Canalolithiasis theory: Described by Hall et al.35 in 1979 and given further prominence by Brandt and Steddin8 (1993), who disputed the cupulolithiasis and other theories. They proposed that otoconial debris floats freely in the PSSC rather than getting attached to the cupula. Rapid changes in the head position in respect to gravity causes downwards movement of this otoconial “clots” of debris and this induces the endolymphatic flow and cupular deflection resulting in the typical features of BPPV. The time lag in the aggregation of the otoconial floaters into ‘clots’ could account for the latent period elicited in BPPV.
Currently, it is believed that canalolithiasis theory explains most of the classical features of BPPV and coexists with cupulolithiasis. Therefore, both theories are thought to be relevant in the pathogenesis of BPPV.
Natural history, course, and diagnosis of BPPV
Case history of BPPV
Patients describe repeated, positionally-induced, sudden onset, brief episodes of vertigo, usually lasting thirty seconds or less in duration. Movements which may trigger episodes include turning over in bed; getting in and out of bed; bending over and then straightening up; extending the neck to look up, such as reaching for an item from a shelf (top-shelf vertigo); or hanging up washing.36 Turning the head from side to side while standing does not provoke symptoms, as the PSSC is not stimulated by this action.37 Associated symptoms may include nausea and vomiting if the BPPV is severe; and nonspecific dizziness similar to motion sickness that may last throughout the day.37–39 A fear of falling backward is an almost unique complaint associated with BPPV.40 Patients may also complain of unsteadiness of gait and postural instability during the active and inactive phases of BPPV, and occasionally after treatment.41 The description given is often one of “walking on pillows” and may be classified as otolithic vertigo.40
The presence of vertigo may become a psychologically disabling symptom for several reasons. First, vertigo is difficult to identify or to see physically, leaving patients unable to locate its source, and thus prone to somatization. 42 Second, attacks of BPPV may be frightening and potentially dangerous, for instance should an attack occur when climbing a ladder.40,41 Furthermore, episodes may be unpredictable, and thus fear of an attack and a tendency to anxiety and panic is well established.42–44 Third, research has suggested that a significant decline in the quality of life occurs with the onset of BPPV.45–48
Natural course of BPPV
It is thought that clinicians do not appreciate the natural course of BPPV, in particular its recurring nature.49,50 BPPV tends to present with clusters of episodes in a limited period of time (the “active” phase), followed by an interval of no attacks (the ‘inactive’ period) before recurring again.40,51,52 Periods of remission may be variable over many years.
Epley (1993) suggested that awaiting spontaneous resolution was not desirable as the nature of BPPV may be severely incapacitating. As BPPV may be concomitant with, and perhaps mask, other otologic or neurologic disease, which may only be revealed once the BPPV has been resolved; treatment of BPPV should occur as soon as possible.53 Finally, with research suggesting that 30% of untreated cases of BPPV were still symptomatic one year after diagnosis, the likelihood of spontaneous remission is not so high as to withhold other treatment options.51
Diagnosis of BPPV: Dix Hallpike Maneuver
Diagnosis of PSSC BPPV rests on recognition of characteristic positioning nystagmus in a patient with a typical history of positional vertigo.37 The Dix Hallpike Maneuver (DHM) is the test most commonly used to induce signs and symptoms of BPPV, and is regarded as the gold standard and critical for accurate diagnosis.54 It is illustrated in Figure 2. Note that the head is positioned prior to assuming a supine position.
Figure 2.

Dix-Hallpike maneuver to the left. (Reproduced with permission from Dr. A. K. Vats, http://dizziness.webs.com/bppv.htm)
However, there are issues with the DHM's use as gold standard.9 The DHM is not 100% sensitive due to the nature of BPPV which cycles through acute and clinically silent phases. If a patient is examined during a sub-clinical period, symptoms and signs may not be provoked.54,55 In addition, an appraisal of the literature has revealed that estimates of specificity are lacking.54 In spite of some concerns regarding the use of the DHM as gold standard, it is mandatory in cases with a strong history of BPPV.54 Due to BPPV's common association with other vestibular lesions;26 and the fact that up to one third of patients with BPPV may present with an atypical history;56,57 it is argued that careful examination including a DHM is essential in all patients who complain of dizziness or imbalance. Moreover, in complex cases with more than one subtype of dizziness, successful treatment of BPPV with a canalith repositioning maneuver (CRP), may resolve one aspect of the symptomatology.
The response to a DHM reveals the key features of canalolithiasis. As the patient reclines with the head hyper-extended over the end of the table, the clot of canaliths will move in an ampullofugal direction, which in turn displaces the cupula due to a plunger effect created by the clot moving in the narrow semi-circular canal.58,59 The inertia of the canaliths, in addition to the time taken for them to settle in the most dependent part of the canal, helps to explain the latent period for the onset of symptoms and signs noted after having assumed the supine position.20,59 Cupular deflection produces an excitatory response, which in turn leads to vertigo and torsional nystagmus in the plane of the posterior canal20 . The nystagmus builds up to a crescendo and then declines quickly as the endolymph drag stops when the canalith mass reaches the limit of its descent and the cupula moves back to its neutral position.40 Upon the patient assuming a seated position at the end of the Dix-Hallpike maneuver, reversal nystagmus occurs as the mass of particles has moved in the opposite direction, creating nystagmus in the same plane, but opposite direction.40 The torsional nystagmus, which is the result of the neural firing in response to gravity, is difficult to suppress with fixation; so simple observation of the patient's eyes will confirm the response.60–62 However, in mild cases Frenzel's lenses may allow better visualization of the nystagmus and infrared video goggles are suggested if they are available.60,63–70 Patients who have a history of BPPV with a negative DHM should be tested with the supine roll in order to exclude lateral semicircular canal BPPV.9 However, note that a subset of patients will have a history of BPPV but will test negative for both the DHM and supine roll.54 These patients should be evaluated on another occasion, preferably when they are complaining of symptoms.
Differential diagnosis
Positioning testing establishes the diagnosis and also helps differentiate BPPV from positional vertigo of central origin and other forms of vertigo. Classically positive results from the DHM suggesting a peripheral site of lesion will meet the following criteria: Linear-rotatory nystagmus with fast phase toward the undermost ear; reversal of direction of the nystagmus on sitting; duration of nystagmus and accompanying vertigo is usually less than 1 min. The nystagmus and vertigo will present in a crescendo-decrescendo pattern. The duration of the latent period prior to the onset of signs of nystagmus and symptoms of vertigo will vary depending on the type of lesion; cupulolithiasis (about 2 s) and canalolithiasis (up to 30s).
Positional vertigo is nearly always a benign condition that can be treated easily at the bedside, but in rare cases it can be a symptom of a central lesion, particularly one near the fourth ventricle. Central positional nystagmus is nearly always purely vertical (either up-beating or down-beating), and there are usually associated neurologic findings. The lesions in central PPV are often found dorsolateral to the fourth ventricle or in the dorsal vermis. This localization, together with other clinical features (associated cerebellar and oculomotor signs), generally allows for differentiation between central PPV from BPPV.35
Contraindications to DHM
Humphriss and colleagues71 raised concerns about possible contraindications to the DHM. Examples of pathologies which could have serious consequences include atlantoaxial subluxation and occipito-atlantal instability; in which the application of the DHM may result in compression of the medulla and brainstem and possible vascular compromise. In patients with neck pain, the clinician should hold the patient's head securely with both hands and avoid moving the patient by the shoulders in order to avoid neck injury.70 Prepositioning the head at a 45° angle from the sagittal plane before any downward movement is essential and reduces the risk of injury.70 It is standard clinical practice to ask the patient for a brief history of neck or spinal problems prior to performing the DHM. Clinicians testing obese patients or those with limited mobility may require assistance in order to fully support the patient.9 Humphriss et al., suggested that there is good evidence that the DHM is a safe procedure. The side-lying test71 is an effective alternative for patients unable to undergo the standard DHM; although it has not been subject to as much research as the DHM.
Treatment modalities of BPPV
Management options range from counseling the patient, but not giving any treatment while spontaneous resolution is awaited; physical exercises and repositioning maneuvers and in intractable cases, surgery (posterior canal occlusion procedure or singular neurectomy).51 Counseling is an important first step in treatment. Many patients, due to the frightening nature of the attacks, have marked serious illness worry and require extensive reassurance about the essentially benign nature of their disorder.37 Whatever the treatment option selected, more than half of the patient population will have at least one exacerbation after their initial remission.37,51 The likelihood of relapse should be discussed with the patient in order to reduce anxiety should a relapse occur.40 Indeed, repositioning procedures should be presented to the patient as a treatment and not a cure of their BPPV.
Clinical guidelines do not support the use of medication to treat BPPV as there is no evidence that they are effective.9,72,73 It should be noted that vestibular suppressants may retard central processes of compensation as well as increase the risk of falling.9 However, medication such as promethazine HCI (Phenergan) may be indicated prior to treatment by repositioning maneuvers in patients with severe nausea or vomiting.74
Brandt-Daroff exercises
A sequence of exercises designed by Brandt and Daroff were the first effective physical therapy exercises specifically designed for the treatment of BPPV.41 Brandt-Daroff exercises are a sequence of rapid, lateral head and trunk tilts that are repeated serially to diminish vertigo. Although the precise mechanism for relief of BPPV is not clear, it is thought that debris may be dislodged or dispersed into an area where it can no longer trigger symptoms.75 Exercises are demonstrated to the patient who follows a program at home over a period of time (usually 10–12 days) until s/he becomes asymptomatic.75 Self-administered Brandt-Daroff exercises are less effective than a canalith repositioning procedure in the treatment of posterior canal BPPV; have a low success rate and should not be used as initial treatment.46,73
Semont's Liberatory maneuver
The Semont's Liberatory maneuver for cupulolithiasis is characterized by extremely rapid movement as the patient is moved in a cart-wheeling motion from the dependent Dix-Hallpike position to the opposite side through sitting [Figure 3].46 The speed of the movement is necessary as both inertia and gravity act to remove any particles adhering to the cupula and to prevent the particles falling back toward the ampulla.46,51
Figure 3.
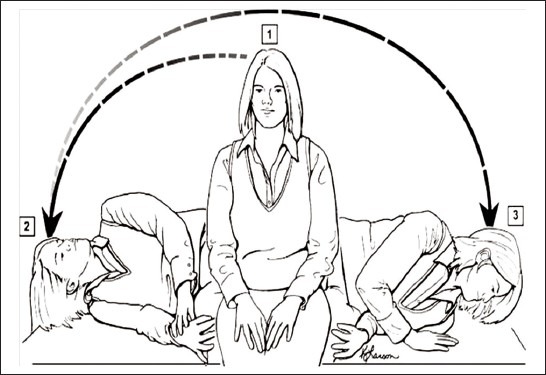
The Semont's manoeuver for right-sided BPPV. Steps: (1) Patient is seated in the upright position; then the head is turned 45° toward the left side, and the patient is then rapidly moved to the side-lying position as shown in position (2) This position is held for approximately 30 s, and then the patient is rapidly moved to the opposite side-lying position without pausing in the sitting position and without changing the head position relative to the shoulder, resulting in position (3) This position is maintained for 30 s and then the patient gradually resumes the upright sitting position. (Adapted from Ref. 75 and reproduced by permission from Gwen Johnson, Wolter Kluwer Health Imprints, www.LWW.com)
The maneuver is aggressive and potentially distressing and harmful to patients, especially those with mobility problems.74,76 Evidence-based reviews have suggested that the Semont is possibly effective or more effective than no treatment or Brandt-Daroff exercises treatment for BPPV. The authors noted that there is not enough evidence to establish the relative efficacy of the Semont to the canalith repositioning procedure.9,73
The remaining ranges of therapeutic maneuvers designed to settle BPPV all rest on acceptance of the canalolithiasis hypothesis; that is, that the canaliths are free-floating in the posterior semi-circular canal and are thus able to move freely when the canal is orientated appropriately.40,51 Treatment of choice for BPPV is the use of repositioning maneuvers in order to achieve complete remission from attacks of vertigo [Figure 4]; improve quality of life and reduce fall risk.9,38,77,78 While treatment strategies for BPPV were hailed as the most important breakthrough in the field of neurotology in the past twenty five years;58 others have queriedwhether the progress made in the successful diagnosis and treatment of BPPV has been reflected in medical practice.48
Figure 4.
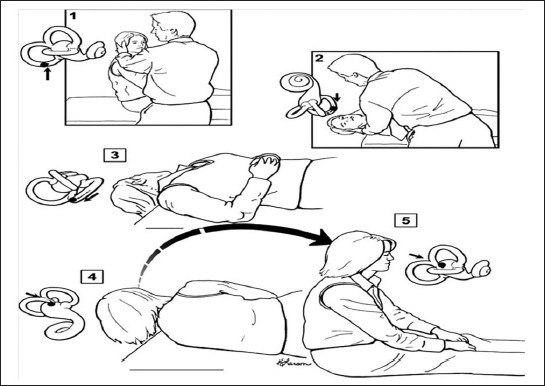
Epley's Canalith repositioning procedure. (Adapted from Ref. 75 and reproduced with the permission of Gwen Johnson, Wolter Kluwer Health Imprints, www.LWW.com)
Epley's Canalith repositioning procedure
The CRP uses gravity to settle cases of posterior canal canalolithiasis. The procedure starts in the supine Dix-Hallpike position with the affected ear undermost. The head is slowly rolled through moderate extension to the unaffected side and maintained in this position briefly, before the patient is rolled into a side-lying position with the head turned 45° down toward the floor [Figure 4]. In the final position, the patient may develop a brief episode of vertigo and nystagmus, which is indicative of debris moving inside the PSSC. With the head deviated to the unaffected side, and the head pitched down, the patient is slowly brought to the sitting position.74 Following Epley's pioneering work; subsequent researchers adopted a single treatment approach and did not perform multiple repositioning within one session.79,80 Further modifications have included the abandonment of vibration, premedication and post-CRP movement restrictions.81
CRP is a safe and effective procedure that is recommended to patients with PSSC BPPV.9,73 However, practitioners are cautioned to ensure proper training in order to perform a DHM as well as treatment procedures for BPPV.81 Complications can result in the form of a canal conversion in between 2.5% and 6% of cases– where the BPPV moves from the PSSC to the LSSC. Thus, clinicians should be able to recognize and treat these variants.46,82 Another event that may occur during the CRP is “canalith jam.” This occurs as a transient burst of nystagmus that persists irrespective of head position, accompanied by intense vertigo.40 It is assumed that the canaliths jam as they migrate from the wider ampulla to the narrower segment of the canal. Treatment is given immediately by repositioning the crus by inversion, allowing gravity to reverse dense debris out of the jam.83,84
Self-treatment strategies
New self-treatment strategies based on the CRP and Semont's maneuvers have been developed.85 Analysis has shown that self-treatment with a CRP is more effective than self-treatment with the Semont, and the patients had difficulty in performing the Semont correctly at home. In spite of suggestions that self-treatment strategies based on the CRP would be appropriate as an adjunct to office-based procedures,86 clinicians should ensure that patients are appropriate candidates and are able to perform the exercises correctly.
CONCLUSION
Benign paroxysmal positional vertigo is a peripheral vestibular disorder first described by Barany (1921), which theoretically involves any of the three semicircular canals but principally the posterior. Several attempts have been made at explaining the mechanism/pathogenesis of the disease; however, none appears to be all inclusive. Most cases of BPPV are idiopathic and the rest associated with some secondary disorders.
Although BPPV is a common disorder and there are excellent prescribed guidelines for its diagnosis and treatment; practitioners should avoid using a “shotgun” approach and ensure treatment is tailored specifically to the type of BPPV and the canal in which it occurs. Furthermore, the only way to assess the outcome of treatment and lack of complications is to perform a repeat DHM after treatment. Therefore, there is no rationale to treat and discharge BPPV patients without further follow-up.
Finally, evidence has shown that canalith repositioning procedure remains gold standard in the treatment of BPPV except for very occasional intractable cases that might require surgery. The best clinical practice counsels strongly against the use of medications in management of primary BPPV except for treatment of associated pathologies or symptomatic management of nausea/emesis.
ACKNOWLEDGMENTS
We hereby acknowledge the Association of African Universities through which platform this collaboration was made possible. In addition, we are grateful to the authorities of the University of Cape Town South Africa and University of Abuja Nigeria for their support.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Bárány R. In the areas of diagnosis krankheitserschernungen otolithenapparates. Acta Otolaryngol (Stockh) 1921;2:434–7. [Google Scholar]
- 2.Dix MR, Hallpike CS. The pathology, symptomatology and diagnosis of certain common disorders of the vestibular system. Ann Otol Rhinol Laryngol. 1952;61:987–1016. doi: 10.1177/000348945206100403. [DOI] [PubMed] [Google Scholar]
- 3.Schuknecht HF. Positional vertigo: Clinical and experimental observations. Trans Am Acad Ophthalmol Otolaryngol. 1962;66:319–32. [PubMed] [Google Scholar]
- 4.Schuknecht HF. Cupulolithiasis. Arch Otolaryngol. 1969;90:765–78. doi: 10.1001/archotol.1969.00770030767020. [DOI] [PubMed] [Google Scholar]
- 5.Gacek RR. Further observations on posterior ampullary nerve transection for positional vertigo. Ann Otol Rhinol Laryngol. 1978;87:300–5. doi: 10.1177/000348947808700301. [DOI] [PubMed] [Google Scholar]
- 6.Epley JM. New dimensions of benign paroxysmal positional vertigo. Otolaryngol Head Neck Surg. 1980;88:599–605. doi: 10.1177/019459988008800514. [DOI] [PubMed] [Google Scholar]
- 7.Semont A, Freyss G, Vitte E. Curing the BPPV with a liberatory maneuver. Adv Otorhinolaryngol. 1988;42:290–3. doi: 10.1159/000416126. [DOI] [PubMed] [Google Scholar]
- 8.Brandt T, Steddin S. Current view of the mechanism of benign paroxysmal positional vertigo: Cupulolithiasis or canalolithiasis? J Vestib Res. 1993;3:373–82. [PubMed] [Google Scholar]
- 9.Parnes LS, McClure JA. Free-floating endolymph particles: A new operative finding during posterior semicircular canal occlusion. Laryngoscope. 1992;102:988–92. doi: 10.1288/00005537-199209000-00006. [DOI] [PubMed] [Google Scholar]
- 10.Bhattacharyya N, Baugh RF, Orvidas L, Barrs D, Bronston LJ, Cass S, et al. Clinical practice guideline: Benign paroxysmal positional vertigo. Otolaryngol Head Neck Surg. 2008;139(5 Suppl 4):S47–81. doi: 10.1016/j.otohns.2008.08.022. [DOI] [PubMed] [Google Scholar]
- 11.von Brevern M, Radtke A, Lezius F, Feldmann M, Ziese T, Lempert T, et al. Epidemiology of benign paroxysmal positional vertigo: A population based study. J Neurol Neurosurg Psychiatry. 2007;78:710–5. doi: 10.1136/jnnp.2006.100420. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Somefun OA, Giwa OS, Bamgboye BA, Okeke-Igbokwe II, Azeez AA. Vestibular disorders among adults in a tertiary hospital in Lagos, Nigeria. Eur Arch Otorhinolaryngol. 2010;267:1515–21. doi: 10.1007/s00405-010-1272-5. [DOI] [PubMed] [Google Scholar]
- 13.Neuhauser HK, Lempert T. Vertigo: Epidemiologic aspects. Semin Neurol. 2009;29:473–81. doi: 10.1055/s-0029-1241043. [DOI] [PubMed] [Google Scholar]
- 14.Salvinelli F, Firrisi L, Casale M, Trivelli M, D’Ascanio L, Lamanna F, et al. Benign paroxysmal positional vertigo: Diagnosis and treatment. Clin Ter. 2004;155:395–400. [PubMed] [Google Scholar]
- 15.Neuhauser H, Lempert T. Vertigo and dizziness related to migraine: A diagnosticchallenge. Cephalalgia. 2004;24:83–91. doi: 10.1111/j.1468-2982.2004.00662.x. [DOI] [PubMed] [Google Scholar]
- 16.Suarez H, Alonso R, Arocena M, Suarez A, Geisinger D. Clinical characteristics ofpositional vertigo after mild head trauma. Acta Otolaryngol. 2011;131:377–81. doi: 10.3109/00016489.2010.534113. [DOI] [PubMed] [Google Scholar]
- 17.Andaz C, Whittet HB, Ludman H. An unusual cause of benign paroxysmal positional vertigo. J Laryngol Otol. 1993;107:1153–4. doi: 10.1017/s0022215100125538. [DOI] [PubMed] [Google Scholar]
- 18.Pollak L, Kushnir M, Goldberg HS. Physical inactivity as a contributing factor for onset of idiopathic benign paroxysmal positional vertigo. Acta Otolaryngol. 2011;131:624–7. doi: 10.3109/00016489.2011.552524. [DOI] [PubMed] [Google Scholar]
- 19.Korres S, Balatsouras DG, Kaberos A, Economou C, Kandiloros D, Ferekidis E. Occurrence of semicircular canal involvement in benign paroxysmal positional vertigo. Otol Neurotol. 2002;23:926–32. doi: 10.1097/00129492-200211000-00019. [DOI] [PubMed] [Google Scholar]
- 20.Katsarkas A. Benign paroxysmal positional vertigo (BPPV): Idiopathic versus post-traumatic. Acta Otolaryngol. 1999;119:745–9. doi: 10.1080/00016489950180360. [DOI] [PubMed] [Google Scholar]
- 21.Baloh RW, Honrubia V, Jacobson K. Benign positional vertigo: Clinical and oculographic features in 240 cases. Neurology. 1987;37:371–8. doi: 10.1212/wnl.37.3.371. [DOI] [PubMed] [Google Scholar]
- 22.Parnes LS, Agrawal SK, Atlas J. Diagnosis and management of benign paroxysmal positional vertigo (BPPV) CMAJ. 2003;169:681–93. [PMC free article] [PubMed] [Google Scholar]
- 23.Mandalà M, Santoro GP, Awrey J, Nuti D. Vestibular neuritis: Recurrence and incidence of secondary benign paroxysmal positional vertigo. Acta Otolaryngol. 2010;130:565–7. doi: 10.3109/00016480903311278. [DOI] [PubMed] [Google Scholar]
- 24.Wu ZM, Zhang SZ, Liu XJ, Chen X, Ji F, Chen AT, et al. Benign paroxysmal positioning vertigo related to inner ear disorders. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2007;42:821–5. [PubMed] [Google Scholar]
- 25.Pulec JL, Patterson MJ. Vestibular nerve pathology in cases of intractable vertigo: An electronmicroscopic study. Am J Otol. 1997;18:475–83. [PubMed] [Google Scholar]
- 26.Gross EM, Ress BD, Viirre ES, Nelson JR, Harris JP. Intractable benign paroxysmal positional vertigo in patients with Ménière's disease. Laryngoscope. 2000;110:655–9. doi: 10.1097/00005537-200004000-00022. [DOI] [PubMed] [Google Scholar]
- 27.Warninghoff JC, Bayer O, Ferrari U, Straube A. Co-morbidities of vertiginous diseases. BMC Neurol. 2009;9:29. doi: 10.1186/1471-2377-9-29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Lee NH, Ban JH, Lee KH, Kim SM. Benign paroxysmal positional vertigo secondary to inner ear disease. Otolaryngol Head Neck Surg. 2010;143:413–7. doi: 10.1016/j.otohns.2010.06.905. [DOI] [PubMed] [Google Scholar]
- 29.Li P, Zeng XL, Li YQ, Zhang GH, Ye J. The clinical characteristics of the benign paroxysmal positional vertigo associated with Meniere's disease. Zhonghua Yi Xue Za Zhi. 2010;90:1921–3. [PubMed] [Google Scholar]
- 30.Babić B, Arsović N. Assessment of senses of hearing and balance in chronic suppurative otitis media. Srp Arh Celok Lek. 2008;136:307–12. doi: 10.2298/sarh0806307b. [DOI] [PubMed] [Google Scholar]
- 31.Crossland G, De R, Axon P. Far advanced otosclerosis and intractable benign paroxysmal positional vertigo treated with combined cochlear implantation and posterior semicircular canal occlusion. J Laryngol Otol. 2004;118:302–4. doi: 10.1258/002221504323012076. [DOI] [PubMed] [Google Scholar]
- 32.Collison PJ, Kolberg A. Canalith repositioning procedure for relief of post-stapedectomy benign paroxysmal positional vertigo. S D J Med. 1998;51:85–7. [PubMed] [Google Scholar]
- 33.Seo T, Hashimoto M, Saka N, Sakagami M. Hearing and vestibular functions after plugging surgery for the posterior semicircular canal. Acta Otolaryngol. 2009;129:1148–52. doi: 10.3109/00016480802609582. [DOI] [PubMed] [Google Scholar]
- 34.Baloh RW, Kerber KA. Clinical Neurophysiology of vestibular system. 4th ed. New York: Oxford University Press; 2010. [Google Scholar]
- 35.Hall SF, Ruby RR, McClure JA. The mechanics of benign paroxysmal vertigo. J Otolaryngol. 1979;8:151–8. [PubMed] [Google Scholar]
- 36.Fife TD, Iverson DJ, Lempert T, Furman JM, Baloh RW, Tusa RJ, et al. Practice parameter: Therapies for benign paroxysmal positional vertigo (an evidence-based review): Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 2008;70:2067–74. doi: 10.1212/01.wnl.0000313378.77444.ac. [DOI] [PubMed] [Google Scholar]
- 37.Gordon AG. Benign paroxysmal positional vertigo (BPPV) or bubble provoked positional vertigo? J Neurol Sci. 1992;111:229–33. doi: 10.1016/0022-510x(92)90076-w. [DOI] [PubMed] [Google Scholar]
- 38.Büttner U, Helmchen C, Brandt T. Diagnostic criteria for central versus peripheral positioning nystagmus and vertigo: A review. Acta Otolaryngol. 1999;119:1–5. doi: 10.1080/00016489950181855. [DOI] [PubMed] [Google Scholar]
- 39.Baloh RW, Honrubia V. Clinical neurophysiology of the vestibular system. 3rd ed. New York: Oxford University Press; 2001. [PubMed] [Google Scholar]
- 40.Hilton M, Pinder D. The Epley maneuver for benign paroxysmal positional vertigo–a systematic review. Clin Otolaryngol Allied Sci. 2002;27:440–5. doi: 10.1046/j.1365-2273.2002.00613.x. [DOI] [PubMed] [Google Scholar]
- 41.Koelliker P, Summers RL, Hawkins B. Benign paroxysmal positional vertigo: Diagnosis and treatment in the emergency department–a review of the literature and discussion of canalith-repositioning maneuvers. Ann Emerg Med. 2001;37:392–8. doi: 10.1067/mem.2001.112250. [DOI] [PubMed] [Google Scholar]
- 42.Brandt T. Vertigo: Its multisensory syndromes. 2nd ed. New York: Springer; 1999. [Google Scholar]
- 43.Blatt PJ, Georgakakis GA, Herdman SJ, Clendaniel RA, Tusa RJ. The effect of the canalith repositioning maneuver on resolving postural instability in patients with benign paroxysmal positional vertigo. Am J Otol. 2000;21:356–63. doi: 10.1016/s0196-0709(00)80045-9. [DOI] [PubMed] [Google Scholar]
- 44.Monzani D, Casolari L, Guidetti G, Rigatelli M. Psychological distress and disability in patients with vertigo. J Psychosom Res. 2001;50:319–23. doi: 10.1016/s0022-3999(01)00208-2. [DOI] [PubMed] [Google Scholar]
- 45.Squires TM, Weidman MS, Hain TC, Stone HA. A mathematical model for top-shelf vertigo: The role of sedimenting otoconia in BPPV. J Biomech. 2004;37:1137–46. doi: 10.1016/j.jbiomech.2003.12.014. [DOI] [PubMed] [Google Scholar]
- 46.Honrubia V, Bell TS, Harris MR, Baloh RW, Fisher LM. Quantitative evaluation of dizziness characteristics and impact on quality of life. Am J Otol. 1996;17:595–602. [PubMed] [Google Scholar]
- 47.Chang AK, Schoeman G, Hill M. A randomized clinical trial to assess the efficacy of the Epley Maneuver in the treatment of acute benign positional vertigo. Acad Emerg Med. 2004;11:918–24. doi: 10.1197/j.aem.2004.06.001. [DOI] [PubMed] [Google Scholar]
- 48.Helminski JO, Zee DS, Janssen I, Hain TC. Effectiveness of particle repositioning maneuvers in the treatment of benign paroxysmal positional vertigo: A systematic review. Phys Ther. 2010;90:663–78. doi: 10.2522/ptj.20090071. [DOI] [PubMed] [Google Scholar]
- 49.López-Escámez JA, Fiñana, Fernandez AJ, Gámiz MJ, Sanchez-Canet I. Impact of treatment on Benign Positional Vertigo - related quality of life. Int Congr Ser. 2003;1240:1329–32. [Google Scholar]
- 50.von Brevern M, Lezius F, Tiel-Wilck K, Radtke A, Lempert T. Benign paroxysmal positional vertigo: Current status of medical management. Otolaryngol Head Neck Surg. 2004;130:381–2. doi: 10.1016/j.otohns.2003.07.007. [DOI] [PubMed] [Google Scholar]
- 51.López-Escámez JA. Role of vestibular testing in diagnosis of Benign Paroxysmal Positional Vertigo. Otolaryngol Head Neck Surg. 2009;141:7–9. doi: 10.1016/j.otohns.2009.03.016. author reply 10-1. [DOI] [PubMed] [Google Scholar]
- 52.Guidetti G, Trebbi M. The recurrences of Paroxysmal Positional Vertigo. Audiol Med. 2005;3:21–6. [Google Scholar]
- 53.Stockwell CW. Vestibular testing: Past, present, future. Br J Audiol. 1997;31:387–98. doi: 10.3109/03005364000000035. [DOI] [PubMed] [Google Scholar]
- 54.Beynon GJ. A review of management of benign paroxysmal positional vertigo by exercise therapy and by repositioning maneuvers. Br J Audiol. 1997;31:11–26. doi: 10.3109/03005364000000005. [DOI] [PubMed] [Google Scholar]
- 55.Giannoni B, Vannucchi P, Pagnini P. Definition and classification of paroxysmal positional vertigo. Audiol Med. 2005;3:4–6. [Google Scholar]
- 56.Halker RB, Barrs DM, Wellik KE, Wingerchuk DM, Demaerschalk BM. Establishing a diagnosis of benign paroxysmal positional vertigo through the dix-hallpike and side-lying maneuvers: A critically appraised topic. Neurologist. 2008;14:201–4. doi: 10.1097/NRL.0b013e31816f2820. [DOI] [PubMed] [Google Scholar]
- 57.Caruso G, Nuti D. Epidemiological data from 2270 paroxysmal positional vertigo patients. Audiol Med. 2005;3:7–11. [Google Scholar]
- 58.Furman JM, Jacob RC. A clinical taxonomy of dizziness and anxiety in the otoneurological setting. J Anxiety Disord. 2001;15:9–26. doi: 10.1016/s0887-6185(00)00040-2. [DOI] [PubMed] [Google Scholar]
- 59.Kentala E, Pyykkö I. Vertigo in patients with Benign Paroxysmal Positional Vertigo. Acta Otolaryngol. 2000;120(Suppl 543):20–2. doi: 10.1080/000164800453847. [DOI] [PubMed] [Google Scholar]
- 60.Baloh RW. Clinical features and pathophysiology of posterior canal Benign Paroxysmal Positional Vertigo. Audiol Med. 2005;3:12–5. [Google Scholar]
- 61.Korres SG, Balatsouras DG. Diagnostic, pathophysiologic and therapeutic aspects of benign paroxysmal positional vertigo. Otolaryngol Head Neck Surg. 2004;131:438–44. doi: 10.1016/j.otohns.2004.02.046. [DOI] [PubMed] [Google Scholar]
- 62.Bronstein AM. Vestibular reflexes and positional manœuvres. J Neurol Neurosurg Psychiatry. 2003;74:289–93. doi: 10.1136/jnnp.74.3.289. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Hamid MA. Contemporary neurovestibular physiologic assessment. Curr Opin Otolaryngol Head Neck Surg. 2000;8:391–7. [Google Scholar]
- 64.Ruckenstein MJ, Shepard NT. Balance function testing: A rational approach. Otolaryngol Clin North Am. 2000;33:507–18. doi: 10.1016/s0030-6665(05)70224-3. [DOI] [PubMed] [Google Scholar]
- 65.Eggers SD, Zee DS. Evaluating the dizzy patient: Bedside examination and laboratory assessment. Semin Neurol. 2003;23:47–58. doi: 10.1055/s-2003-40751. [DOI] [PubMed] [Google Scholar]
- 66.El-Kashlan HL, Telian SA. Diagnosis and initiating treatment for peripheral system disorders: Imbalance and dizziness with normal hearing. Otolaryngol Clin North Am. 2000;33:563–77. doi: 10.1016/s0030-6665(05)70227-9. [DOI] [PubMed] [Google Scholar]
- 67.Honrubia V, Baloh RW, Harris MR, Jacobson KM. Paroxysmal positional vertigo syndrome. Am J Otol. 1999;20:465–70. [PubMed] [Google Scholar]
- 68.Norré ME. Diagnostic problems in patients with benign paroxysmal positional vertigo. Laryngoscope. 1994;104:1385–8. doi: 10.1288/00005537-199411000-00012. [DOI] [PubMed] [Google Scholar]
- 69.Pollak L, Davies RA, Luxon LL. Effectiveness of the particle repositioning maneuver in benign paroxysmal positional vertigo with and without additional vestibular pathology. Otol Neurotol. 2002;23:79–83. doi: 10.1097/00129492-200201000-00018. [DOI] [PubMed] [Google Scholar]
- 70.Wolf M, Hertanu T, Novikov I, Kronenberg J. Epley's manoeuvre for benign paroxysmal positional vertigo: A prospective study. Clin Otolaryngol Allied Sci. 1999;24:43–6. doi: 10.1046/j.1365-2273.1999.00202.x. [DOI] [PubMed] [Google Scholar]
- 71.Humphriss RL, Baguley DM, Sparkes V, Peerman SE, Moffat DA. Contraindications to the Dix-Hallpike manoeuvre: A multidisciplinary review. Int J Audiol. 2003;42:166–73. doi: 10.3109/14992020309090426. [DOI] [PubMed] [Google Scholar]
- 72.Shepard NT, Telian SA. Practical management of the dizzy patient. San Diego: Singular Publishing; 1996. [Google Scholar]
- 73.Cohen HS. Side-lying as an alternative to the Dix Hallpike test of the posterior canal. Otol Neurotol. 2004;25:130–4. doi: 10.1097/00129492-200403000-00008. [DOI] [PubMed] [Google Scholar]
- 74.Epley JM. Benign Paroxysmal Positional Vertigo (Canalithiasis). Diagnosis and non-surgical management. In: Arenberg IK, editor. Dizziness and balance disorders. Amsterdam: Kugler Publishers; 1993. pp. 545–9. [Google Scholar]
- 75.Fife TD, Iverson DJ, Lempert T, Furman JM, Baloh RW, Tusa RJ, et al. Practice parameter: Therapies for benign paroxysmal positional vertigo (an evidence-based review): Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 2008;70:2067–74. doi: 10.1212/01.wnl.0000313378.77444.ac. [DOI] [PubMed] [Google Scholar]
- 76.Herdman SJ, Tusa RJ. Assessment and treatment of patients with Benign Paroxysmal Positional Vertigo. In: Herdman SJ, editor. Vestibular rehabilitation. 2nd ed. Philadelphia: F.A. Davis; 2000. pp. 451–75. [Google Scholar]
- 77.Epley JM. The canalith repositioning procedure: For treatment of benign paroxysmal positional vertigo. Otolaryngol Head Neck Surg. 1992;107:399–404. doi: 10.1177/019459989210700310. [DOI] [PubMed] [Google Scholar]
- 78.Herdman SJ. Advances in the treatment of vestibular disorders. Phys Ther. 1997;77:602–18. doi: 10.1093/ptj/77.6.602. [DOI] [PubMed] [Google Scholar]
- 79.Woodworth BA, Gillespie MB, Lambert PR. The canalith repositioning procedure for benign positional vertigo: A meta-analysis. Laryngoscope. 2004;114:1143–6. doi: 10.1097/00005537-200407000-00002. [DOI] [PubMed] [Google Scholar]
- 80.Herdman SJ, Tusa RJ, Zee DS, Proctor LR, Mattox DE. Single treatment approaches to Benign Paroxysmal Positional Vertigo. Arch Otolaryngol Head Neck Surg. 1993;119:450–4. doi: 10.1001/archotol.1993.01880160098015. [DOI] [PubMed] [Google Scholar]
- 81.Harvey SA, Hain TC, Adamiec LC. Modified Liberatory Maneuver: Effective treatment for Benign Paroxysmal Positional Vertigo. Laryngoscope. 1994;104:1206–12. doi: 10.1288/00005537-199410000-00004. [DOI] [PubMed] [Google Scholar]
- 82.Nuti D, Nati C, Passali D. Treatment of benign paroxysmal positional vertigo: No need for postmaneuver restrictions. Otolaryngol Head Neck Surg. 2000;122:440–4. doi: 10.1016/S0194-5998(00)70070-2. [DOI] [PubMed] [Google Scholar]
- 83.Gordon CR, Gadoth N. Benign paroxysmal positional vertigo: Who can diagnose it, should it be treated and where? Harefuah. 2005;144:567–71. 597. [PubMed] [Google Scholar]
- 84.Epley JM. The canalith repositioning procedure: For treatment of benign paroxysmal positional vertigo. Otolaryngol Head Neck Surg. 1992;107:399–404. doi: 10.1177/019459989210700310. [DOI] [PubMed] [Google Scholar]
- 85.Gans RE, Harrington-Gans PA. Treatment efficacy of Benign Paroxysmal Positional Vertigo (BPPV) with Canalith Repositioning Maneuver and Semont Liberatory Maneuver in 376 patients. Semin Hear. 2002;23:129–42. [Google Scholar]
- 86.Radtke A, von Brevern M, Tiel-Wilck K, Mainz-Perchalla A, Neuhauser H, Lempert T. Self-treatment of Benign Paroxysmal Positional Vertigo. Semont maneuver vs. Epley procedure. Neurology. 2004;63:150–2. doi: 10.1212/01.wnl.0000130250.62842.c9. [DOI] [PubMed] [Google Scholar]