

Abstract
False positive recognition is crucial for proper interpretation of FDG-PET studies. The authors present a case of a woman who underwent surgery over a month prior to PET/CT imaging which revealed significant tracer uptake within muscles and soft tissue in several sites contralateral to the location of surgery. The FDG-PET images of this case illustrate the importance of communication between physicians ordering and physicians reading FDG-PET/CT scans as well as atypical FDG-PET findings that could be interpreted as concerning but are, in fact, innocuous. This study also demonstrates the unusual glucose metabolic patterns which may arise following treatment be it surgical, chemotherapeutic or radiation.
Keywords: positron emission tomography, fluorodeoxyglucose, inflammation, post-surgical changes
Figure 1.
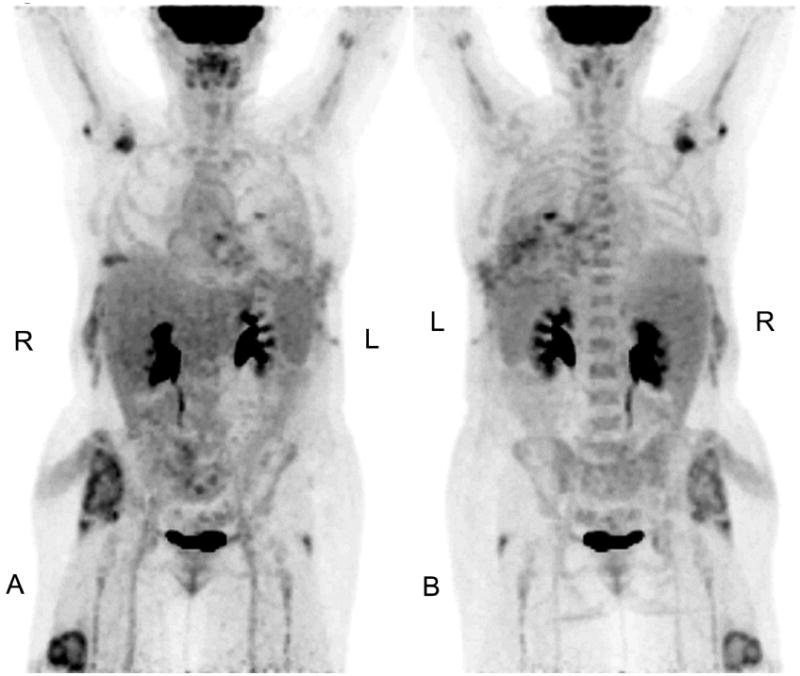
A 48 year-old female with a history of stage IIIB non-small cell lung cancer underwent a whole body FDG-PET/CT for restaging one month following a left extrapleural pneumonectomy and intraoperative photodynamic therapy. Unbeknownst to the nuclear medicine interpreting physicians, the patient was lying in a right lateral decubitus position during this surgical procedure and subsequent emergent re-operation for approximately 14-16 hours. In addition, the patient had been experiencing musculoskeletal pain on her right side during the post-operative recovery period that was not reported to the nuclear medicine interpreting physicians. Her serum creatinine values were not elevated and the patient had no signs of impaired renal function or rhabdomyolosis.
Selected coronal views of maximum intensity projections (A=anterior, B=posterior) of attenuation-corrected maximum intensity projection PET images one hour after intravenous injection of 16.31 mCi of F-18 FDG are shown. The patient's blood glucose level was measured at 107 mg/dl before FDG administration. Several foci of atypical elevated glucose metabolism on the patient's right side are seen. Note radiotracer uptake in the left posterior ribs and soft tissue at the surgical entrance site.
Figure 2.

CT, fused F-18 FDG-PET and CT and FDG-PET (only) transaxial images are shown through the upper thorax (A), abdomen (B), lower pelvis (C) and distal thigh (D). Each slice shows an atypical metabolic pattern as seen in the whole body maximum intensity projection intensity images as above. Maximum SUV of the four atypical FDG- avid regions are 5.0, 3.1, 4.0 and 4.8, respectively.
The affinity of FDG for active inflammatory and infectious disorders is well established 1, 2. Inflammatory processes visualized by FDG-PET include pneumonia 3, atherosclerosis 4, sarcoidosis 5, dermatomyositis6, abcesses 7, 8, inflammatory bowel disease 9, and even statin-induced rhabdomyolysis 10. A pattern of atypical FDG uptake is seen throughout soft tissue and muscle in this patient's right side that can be attributed to stagnant positioning during surgery.
Acknowledgments
This work was funded in part by NIH grant number P01-CA087971.
References
- 1.Zhuang H, Alavi A. 18-fluorodeoxyglucose positron emission tomographic imaging in the detection and monitoring of infection and inflammation. Semin Nucl Med. 2002;32:47–59. doi: 10.1053/snuc.2002.29278. [DOI] [PubMed] [Google Scholar]
- 2.Zhuang H, Yu JQ, Alavi A. Applications of fluorodeoxyglucose-PET imaging in the detection of infection and inflammation and other benign disorders. Radiol Clin North Am. 2005;43:121–34. doi: 10.1016/j.rcl.2004.07.005. [DOI] [PubMed] [Google Scholar]
- 3.Kapucu LO, Meltzer CC, Townsend DW, Keenan RJ, Luketich JD. Fluorine-18-fluorodeoxyglucose uptake in pneumonia. J Nucl Med. 1998;39:1267–9. [PubMed] [Google Scholar]
- 4.Bural GG, Torigian DA, Chamroonrat W, et al. FDG-PET is an effective imaging modality to detect and quantify age-related atherosclerosis in large arteries. Eur J Nucl Med Mol Imaging. 2007 doi: 10.1007/s00259-007-0528-9. [DOI] [PubMed] [Google Scholar]
- 5.Lewis PJ, Salama A. Uptake of fluorine-18-fluorodeoxyglucose in sarcoidosis. J Nucl Med. 1994;35:1647–9. [PubMed] [Google Scholar]
- 6.Liau N, Ooi C, Reid C, Kirkwood ID, Bartholomeusz D. F-18 FDG PET/CT detection of mediastinal malignancy in a patient with dermatomyositis. Clin Nucl Med. 2007;32:304–5. doi: 10.1097/01.rlu.0000257282.76269.85. [DOI] [PubMed] [Google Scholar]
- 7.Kaya Z, Kotzerke J, Keller F. FDG PET diagnosis of septic kidney in a renal transplant patient. Transpl Int. 1999;12:156. doi: 10.1007/s001470050202. [DOI] [PubMed] [Google Scholar]
- 8.Tahara T, Ichiya Y, Kuwabara Y, et al. High [18F]-fluorodeoxyglucose uptake in abdominal abscesses: a PET study. J Comput Assist Tomogr. 1989;13:829–31. doi: 10.1097/00004728-198909000-00014. [DOI] [PubMed] [Google Scholar]
- 9.Louis E, Ancion G, Colard A, Spote V, Belaiche J, Hustinx R. Noninvasive Assessment of Crohn's Disease Intestinal Lesions with 18F-FDG PET/CT. J Nucl Med. 2007;48:1053–9. doi: 10.2967/jnumed.107.040436. [DOI] [PubMed] [Google Scholar]
- 10.Sheehy N, Israel DA. Findings on (18)FDG-PET imaging in statin-induced rhabdomyolysis. Clin Radiol. 2007;62:1012–4. doi: 10.1016/j.crad.2007.04.010. [DOI] [PubMed] [Google Scholar]