

Abstract
Introduction:
Increasing population of elderly and the emergence of epidemic of chronic or (non-communicable) diseases, which is likely to adversely affects their health-related quality of life (HRQOL), has implications on health systems in developing countries such as India. A study was conducted to know the common impairments and disabilities and their effect on HRQOL in elderly population.
Materials and Methods:
A community-based cross-sectional study on elderly, selected by cluster sampling from central Delhi, India, was conducted from April 2005 to February 2006. A pre-tested, semi-structured questionnaire, along with Short Form -36 (SF-36) survey was used for data collection. The data was analyzed using Chi square and student's t test on SPSS v12 statistical software. P value of less than 0.05 was considered statistically significant.
Results:
A total of 200 elderly were included in the study. 71.5% subjects had at least one disability/impairment. Around 40% subjects reported their health being poor and another 50% of worsening of their health in the last 1 year. HRQOL score for people with and without chronic morbidity/disability was 51.8 and 73.5, respectively (P<0.05), with overall mean score 56.7 (±17.2). The most commonly affected HRQOL domains were Role Physical, Physical Functioning, and General Health. The HRQOL and domain scores decreased with increasing age, and females had lower mean scores than males (P<0.05).
Conclusion:
The HRQOL of elderly in urban India is severely affected by impairments and disabilities. There is an immediate need for specific preventive and rehabilitative measures targeted on elderly to maintain their health related quality of life. This information may be utilized for designing any policy and/or program targeted for elderly in India and in other similar settings.
Keywords: Non-communicable diseases, disability, elderly, health-related quality of life, India
Introduction
The demographic transition in the 20th century has led to the continuous increase in elderly population across the world. India with approximately 7.8% population aged more than 60 years(1) is classified as a country with aging population.(2) Although old age is not a disease in itself; the elderly are vulnerable to chronic diseases (diseases which are insidious in onset, such as cardiovascular illness, cardiovascular attacks (CVA), cancers, diabetes, and musculoskeletal and mental illnesses). These chronic illnesses lead to impairments and disabilities, which affects the health related quality of life of the elderly and have implications in the form of rising burden on the health systems in developing countries such as India. There are limited number of studies, which has analysed how impairments and disabilities affects the quality of life of elderly. Hence, this study was conducted to know the common impairments and disabilities and their effect on the health-related quality of life (HRQOL) of the elderly living in an urban area of Delhi, India.
Materials and Methods
A community-based cross-sectional study was carried out in New Delhi district of Delhi state in India. A well-demarcated area, known as “Charge II area,” was selected for this study. This area is divided into 49 blocks of around 150 households each, with a total population in the area estimated to be approximately 50,000. The area is a residential complex, with a few office buildings and educational and religious establishments, including a fair number of Jhhuggi clusters. The population in this area was a mix of different socio-economic strata and a variety of religious and regional backgrounds (this was found as a number of surveys were conducted in this area under Lady Hardinge Medical College, New Delhi. The data collection for this study was done from April 2005 to February 2006.
The people aged more than 60 years were considered elderly in this study,(2) and all persons of both sexes and aged more than 60 years were the study subjects. The sample size of 131 was calculated at 20% prevalence of any morbidity, 95% confidence interval, and 7% standard error. Considering that sampling method was cluster sampling, a design effect of 1.5 was estimated to reach an effective sample of 197 study subjects. Finally, 200 subjects were studied.
The study subjects were selected by cluster sampling from the study area. The inter- and intra-cluster homogeneity analysis was done and it was noted that there was inter-cluster homogeneity and intra-cluster heterogeneity; therefore, it was decided to take 20 clusters and 10 elderly in each cluster. These 20 clusters were selected by cluster technique, and 10 consecutive elderly subjects were studied in each cluster. A central point in each cluster was identified and the direction of the first house was selected by rolling a bottle in the centre of a cluster. The process helped in selecting the first house. Subsequently, house-to-house search was done, and if any elderly was found in the house, it was included in the survey. If there were more than one elderly in a single house, a listing of the elderly was done on the back of the paper and the numbers of a currency note were used to select only one elderly in the study. A self-designed, pre-tested, semi-structured questionnaire along with Short Form - 36 version 2 (SF-36v2) questionnaire(3) was used for data collection. The verbal implied consent of the subjects was taken before going ahead with the interview. The Health-Related Quality of Life (HRQOL) of the elderly in this study was assessed by SF-36 survey.(3) This instrument has 11 questions with 36 items, giving this the name of SF-36. The items are scored on a 3-point or 5-point Likert scale. This 36 items have been divided into eight domains named Physical Functioning (PF), Role Physical (RP), Bodily Pain (BP), General Health (GH), Vitality (VT), Social Functioning (SF), Role Emotional (RE), and Mental Health (MH). The data collected was entered into a computer and was analyzed as per the method suggested by the researchers, who have devised this instrument.(3) In brief, all data was entered into a computer and the needful recoding or reverse coding was done for suggested 10 items. This was followed by a domain score calculation by adding all the item scores in a single domain. This score was finally transformed into a scale of 0–100. The final transformed score was used for analysis in this study. The lowest score of 0 represents the worst status in that domain while the highest score of 100 denotes the best score. The data was analyzed using SPSSv12 statistical package, and Chi square test, student's t test, and ANOVA were applied. A P value of <0.05 was considered statistically significant.
Results
A total of 200 elderly, 89 males and 111 females, were interviewed. The mean age of the subjects was 68.0 ± 6.6 years. There was consistent decrease in the number of subjects with advancing age. Females were higher in number in all age groups except in young old-age groups. The age distribution of the study subjects was almost uniform for both sexes (P value >0.05) [Table 1]. 88% of the subjects were Hindu, 6% Muslims, 2.5% Sikhs, and rest others. Six (3.0%) of the subjects were never married; five of them were males. 68.5% men and 38.7% of the women were married at the time of the study. 42.0% of the subjects were living in joint families and 53.5% in nuclear families. It was also noted that this study population of elderly had multiple impairments and disabilities as shown in second section of Table 1.
Table 1.
Age and sex distribution of the study subjects and physical disabilities
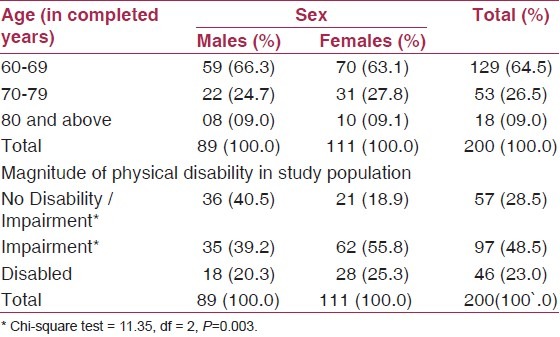
The largest section was of the elderly with some impairment (48.5%). Almost two-fifth males (39.2%) and more than half of females (55.8%) had some form of impairment (P<0.05, significant). Approximately one-fourth (23.0%) of the subjects were disabled. There was significant association of the disability with increasing age. More number of the subjects who were older in age were disabled (P<0.05). Of all males 20.3%, and of all females 25.3%, had some form of disability (P>0.05; not significant). Males with no disability or impairment were almost double in numbers than females, (P<0.05) statistically significant.
Only 12.0%, of the female subjects termed their health as excellent or very good as compared to 35.9% males. There was statistically significant difference in self-appraisal of health, and males reported to have better health than females in this study (P<0.05, significant) [Table 2]. The difference in health transition was found to be statistically significant for the sexes, with more number of females reporting worsening of health than males in comparison of better or same health status.
Table 2.
Self-appraisal of health and transition of health in last 1 year amongst study subjects
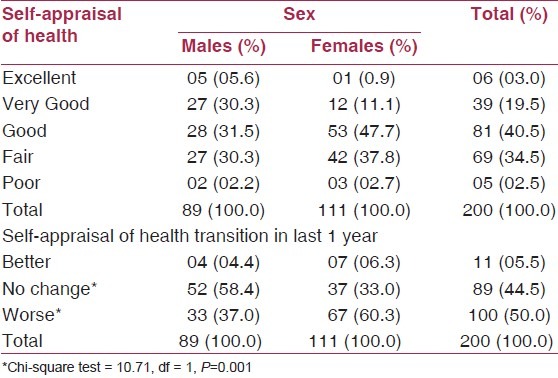
The number of people who complained of worsening of health since last year was higher as age increased (P<0.05), and this was highest for oldest old at 70.6%. (Data not in the Table)
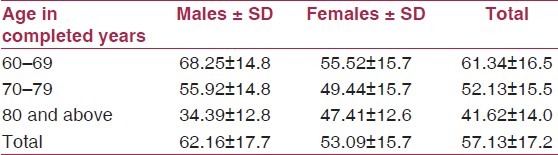
The relationship of age with HRQOL suggests that HRQOL worsened as age increased [Table 3]. The differences in HRQOL scores of young old and old-old were very highly significant (P<0.001). Males had continuous decline in HRQOL scores, with advancing age, which was statistically significant across the age groups (P<0.05, significant). However, the females had lower scores since beginning of old age, and there was no statistically significant difference in the HRQOL scores of old-old and oldest-old.
Table 3.
SF-36 v2 quality of life scores according to age and sex
The comparison of HRQOL scores of elderly without any disability or impairment, of elderly with impairment, and of elderly with disability is given in Table 4. The elderly without any disability or impairment had very high scores in comparison with those who had any impairment or disability. This trend was similar in most of the domains except in bodily pain. Impairment affects all the domains of elderly health significantly, and the presence of disability resulted in further decrease in HRQOL scores.
Table 4.
SF-36 v2 HRQOL scores and disability
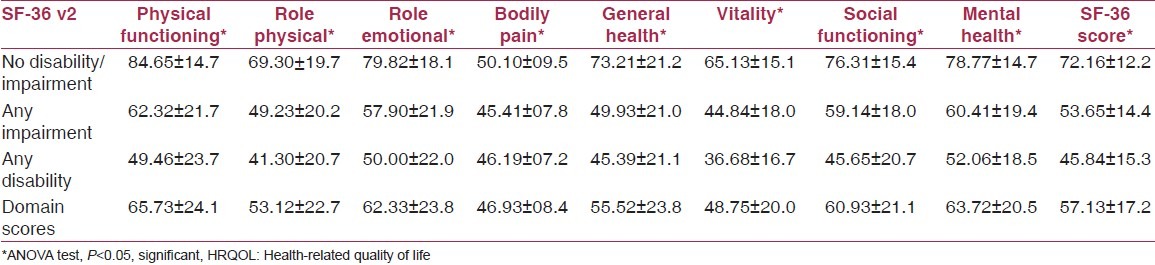
The mean HRQOL score for people with and without chronic morbidity/disability was 51.8 and 73.5, respectively (P<0.05), with population mean being 56.7. Independent of impairment and disability, the most commonly affected HRQOL domains were RP, PF, and GH. Scores decreased as the age increased, with females having less mean scores than males (P<0.05) (data not in Tables). However, with the impairment or disability, the most commonly affected domain in this elderly population was BP (46.93 ± 08.4), followed by VT (48.75 ± 20.0). Two least common affected domains were PF (65.73 ± 24.1) and MH (63.72 ± 20.5). The domains most affected were related to the type of the disability, although any disability affected all domains of HRQOL.
Discussion
The proportion of elderly had decreased in our study as the age increased. This trend is similar to other studied however the proprtions are slightly different from Goel et al.,(4) who found 47.2% of their subjects between 60 and 69 years, 37.8% in 70–79 years, and 15.0% 80 years and above of age, but the proportions are almost similar to a study by Chadha et al.(5) on urban elderly where 60.4% were young old, and 31.6% and 8% were old-old and oldest-old, respectively. Both of these studies were done in urban areas. The gender distribution in the present study is almost similar to that reported by Chadha et al.(5)
The mean number of morbidity in this population was 2.25, which is similar to that reported by a few other researchers,(6–8) however, lower than 6.1 reported by Joshi et al.(9) This difference may be due to variation in the definition taken for the classification of morbidities. There was statistically significant difference in the number of morbidities amongst males and females, and this corroborates the gender difference in morbidities as reported earlier too.(9,10)
The worsening of the health in the last 1 year was reported by majority of those patients who had developed some disease and morbidity in the last year. People without diagnosed morbidities had better HRQOL scores. These findings are in consonance with Jette and Branch,(11) as they commented that there was positive association between disabilities and morbidities. This is the basic notion behind the assessment of HRQOL that it is affected by disability and morbidities, as also propagated by Ware et al.(12)
Elderly without any disability or impairment had very high scores in most of the domains except in BP. The highest and lowest scores in this group were in PF and BP at 84.65 and 50.10, respectively, with total score of 72.16. Impairment and disability adversely affect the health and was reflected by sudden decrease in the scores as elderly with impairment had mean score of 53.65 and highest and lowest of 62.32 and 44.84 in PF and VT, respectively [Table 4]. Impairment and disability affected all the domains of elderly health significantly. There was significant difference in the mean scores of the people affected by impairment and disability and subjects without any disability or impairment (P<0.05). The HRQOL scores are consistent with the health status of the person, and studies report improvement in scores with treatment and rehabilitation. This study has limitations that since we selected only one elderly from each house, there might be some selection bias in the findings. Similarly, socio-demographic, cultural, and psychological factors may play as confounders for HRQOL, which were not analyzed in our study. Furthermore, this study has a small sample size, and a study with bigger sample size could have given more generalizable results.
Conclusion
The elderly population in India is increasing rapidly and this group has higher number of impairments and disabilities. The limited availability of the health facilities and poor access worsen the conditions of elderly, leading to the decrease in their HRQOL. We conclude that HRQOL of elderly in urban India is severely affected by disabilities and impairments, and there is an immediate need for specific preventive and rehabilitative measures targeted towards elderly. The Government needs to effectively plan healthcare services which are elderly friendly, by provision for good healthcare facilities with both preventive and rehabilitative services for the targeted population. The findings of this study may help in designing of various health schemes and policies and programs targeted for improving health status of the elderly in India and in other settings.
Footnotes
Source of Support: Nil,
Conflict of Interest: None declared
References
- 1.Registrar General of Census Operations. Man Singh Road, New Delhi: Government of India; 2001. Census of India 2001. [Google Scholar]
- 2.Problems of the elderly and the Aged, World assembly on the elderly. Report of the Secretary General. New York: United Nations; 1980. United Nations. [Google Scholar]
- 3.Ware JE, Jr, Kosinski M, Dewey JE. Qualitymetric incorporated. Lincoln: United States of America; 2003. How to score Version 2 of SF-36 Health survey; pp. 1–88. [Google Scholar]
- 4.Goel PK, Garg SK, Singh JV, Bhatnagar M, Chopra H, Bajpai SK. Unmet needs of elderly in rural population of Meerut. Indian J Community Med. 2003;28:165–6. [Google Scholar]
- 5.Chadha NK, Chao D, Mir UA, Bhatia H. Structure of social network of the elderly in Delhi. Indian J Gerontology. 2005;19:307–26. [Google Scholar]
- 6.Garg BS, Gupta SC, Mishra VN, Singh RB. A medico social study of aged in urban area. Indian Med Gaz. 1982;114:95–9. [Google Scholar]
- 7.Padda AS, Mohan V, Singh J, Deepti SS, Singh G, Dhillon HS. Health profile of aged persons in urban and rural field practice area of medical college Amritsar. Indian J Community Med. 1998;23:72–6. [Google Scholar]
- 8.Sengupta DK, Chakraborty AK. Health status of males aged 55 years and above in a slum area of Calcutta. Indian J Public Health. 1982;26:112–7. [PubMed] [Google Scholar]
- 9.Joshi K, Kumar R, Avasthi A. Morbidity profile and its relationship with disability and psychological distress among elderly people in Northern India. Int J Epidemiol. 2003;32:978–87. doi: 10.1093/ije/dyg204. [DOI] [PubMed] [Google Scholar]
- 10.Goswami A, Reddaiah VP, Kapoor SK, Singh B, Dey AB, Dwivedi SN, et al. Health problems and health seeking behaviour of rural aged. Indian J Gerontol. 2005;19:163–80. [Google Scholar]
- 11.Jette AM, Branch LG. Impairment and disability in the aged. J Chronic Dis. 1985;38:59–65. doi: 10.1016/0021-9681(85)90008-6. [DOI] [PubMed] [Google Scholar]
- 12.Ware JE, Jr, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992;30:473–83. [PubMed] [Google Scholar]