

Abstract
Background:
The increasing proportion of elderly persons is contributing to an increase in the prevalence of diabetes. The residents of urban slums are more vulnerable due to poverty and lack of access to health care.
Objective:
To estimate the prevalence of diabetes in elderly persons in an urban slum and to assess their awareness, treatment and control of this condition.
Materials and Methods:
All persons aged 60 years and above, residing in an urban slum of Delhi, were included in this cross-sectional community- based study. Data were collected on sociodemographic variables. The participants’ awareness and treatment of diabetes was recorded. Their fasting blood sugar was estimated using an automated glucometer. Diabetes was diagnosed if fasting blood glucose was ≥126 mg/dL, or if the participant was taking treatment for diabetes. Impaired fasting blood glucose was diagnosed if fasting blood glucose was 110–125 mg/dL.
Results:
Among the 474 participants studied, the prevalence of diabetes was estimated to be 18.8% (95% CI 15.3–21.5). It decreased with increasing age, and was higher among women. The prevalence of impaired fasting blood glucose was 19.8% (95% CI 16.3–23.7). It was higher among women. One-third of the diabetic participants were aware of their condition; two-thirds of these were on treatment and three-fourths of those on treatment had controlled fasting blood sugar level. The awareness, treatment and control were better among women.
Conclusions:
Diabetes is common among elderly persons in urban slums. Its magnitude and low awareness warrant effective public health interventions for their treatment and control.
Keywords: Awareness, diabetes, elderly, older persons, slum
Introduction
Diabetes is a common non-communicable disease in India, as well as the rest of the world. The estimates of prevalence of diabetes suggested that nearly 3% of adults were diabetic in the year 2000, and this figure is projected to be nearly doubled by the year 2030.(1) Diabetes also contributes to 5% of the total mortality.(2,3)
The most important demographic transition in India, as well as in the world, is due to increase in the number of aged persons, leading to an increase in the prevalence of hypertension and diabetes. Recently, India has witnessed this demographic transition, with a reduction in crude birth rate and increase in life expectancy.(4,5)
In spite of its high prevalence, and being a major cause of mortality, diabetes remains highly undiagnosed. Undiagnosed diabetes is associated with increased risk of all-cause mortality.(6) Delayed diagnosis and inadequate or improper treatment result in poor disease outcomes.
Low-socioeconomic status is associated with development of diabetes.(7) Elderly persons living in urban slums are more vulnerable to various non-communicable diseases and their complications due to lack of basic amenities, poor health-seeking behavior and stress due to lack of social support.(8) This study was conducted to estimate the prevalence of diabetes among elderly persons residing in an urban slum and to assess the awareness, treatment and control of this condition among them.
Materials and Methods
This was a cross-sectional, community-based study among elderly persons aged 60 years and above in Sanjay Colony, an urban slum located in the southern part of the National Capital Territory of Delhi, India. The sample size was estimated based on a multicenter study carried out in 10 cities of India, which reported the prevalence of diabetes among the elderly persons as 13.4%.(9) With a relative precision of 25% and a-error of 5%, the sample size was estimated to be 411. Taking a non-response rate of 10%, the sample size was increased to 460. A house-to-house enumeration of all elderly persons in the slum yielded 545 persons. All eligible elderly persons were recruited to the study. The participants were eligible if they had been residing the study area for at least the last 6 months, and were able to comprehend the questions. Data were collected by house-to-house visits during December 2009 to February 2010. Three house visits were made in case the eligible participant was not available on the first visit. Participants who refused to participate or those who could not be contacted despite three house visits were taken as non-responders.
All participants were interviewed in the local language, at their homes. Information on sociodemographic variables, viz. age and sex, and treatment history of diabetes was recorded. All interviews and tests were conducted by a single physician.
Fasting blood sugar was estimated using an EukareR automated glucometer (Eumed Biotechnology Co., Ltd., Jubei City, Hsinchu County, Taiwan). Diabetes was diagnosed if the fasting blood glucose was ≥126 mg/dL (≥7.0 mmol/L) after an overnight fast for at least 8 hours, or if the participant was taking treatment for diabetes.(10) Impaired fasting blood glucose was diagnosed if fasting blood glucose was 110–125 mg/dL (6.1–6.9 mmol/L).(10)
The awareness status regarding their own diabetes mellitus was defined as having diabetes diagnosed by a health professional with presence of a prescription, or anti-diabetic medicines possessed by the participant. The treatment status was defined as taking any pharmacological treatment for diabetes. Participants who were already diabetic and taking treatment were considered to have control if the fasting blood glucose was <126 mg/dL.
Data were entered in Epi-Info software version 3.5.1. Statistical analysis was done in STATA version 9. Proportions were calculated, with 95% confidence intervals, and Chi-square test was applied. The study was approved by the Institute Ethics Committee of the All India Institute of Medical Sciences, New Delhi. Written informed consent was taken from the participants. Provision for referral and service was made for the participants who were diagnosed with any ailment.
Results
A total of 545 eligible elderly persons were enumerated in the study area, of which 496 (91.0%) were interviewed for the study. The remaining 49 participants could not be contacted despite three visits to their homes.
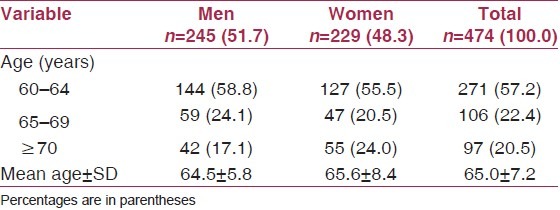
Of the 496 participants who were interviewed, 22 (4.4%) refused for fasting blood sugar estimation. None of these 22 persons had any prescription for anti-diabetic medicines. Hence, fasting blood sugar testing was done in 474 (95.6%) of the 496 participants. Fifty-two percent of the participants were male. About four-fifths of the participants were aged less than 70 years [Table 1]. The mean age was 65.0 years.
Table 1.
Demographic characteristics of the participants
The prevalence of diabetes in elderly persons was estimated to be 18.8% (95% CI 15.3–21.5). It was 15.9% (95% CI 12.7–19.4) and 21.8% (95% CI 18.1–25.7) among men and women, respectively. The prevalence decreased with increasing age [Table 2].
Table 2.
Prevalence of diabetes and impaired fasting blood glucose in the participants
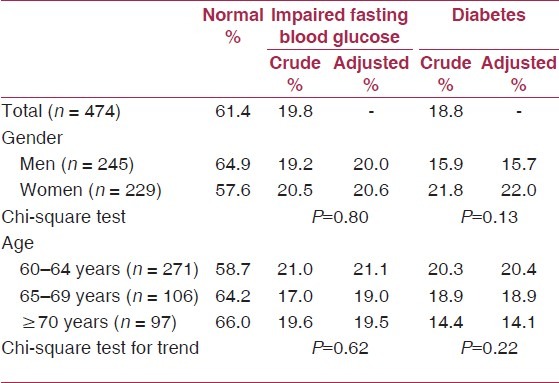
The prevalence of impaired blood glucose was estimated to be 19.8% (95% CI 16.3–23.7). It was 19.2% (95% CI 14.4–24.7) and 20.5% (95% CI 15.5–26.3) among men and women, respectively [Table 2].
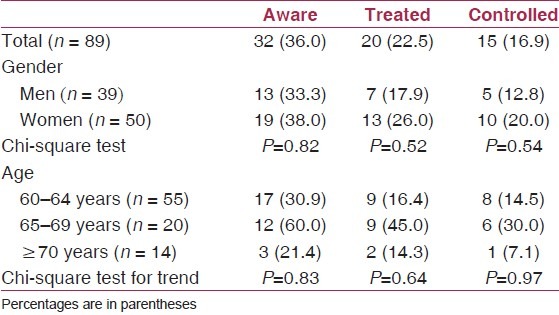
About one-third (36.0%) of the 89 diabetics were aware of their condition. The awareness, treatment and control were better among women; however, this was not statistically significant. Of those participants who were aware, more than half were on treatment. Of those on treatment, three- fourth had controlled fasting blood sugar [Table 3].
Table 3.
Participants with diabetes who were aware, treated and controlled
Discussion
The ageing of population in India is likely to lead to an increase in the prevalence of diabetes. The prevalence of diabetes was estimated to be 18.8% in the present study. Studies from India have reported a prevalence from 13% to 25%, which is comparable.(9,11,12) Studies from other Asian nations such as Thailand and Hong Kong have reported lower prevalence rates of 14% and 15%, respectively.(13,14) Decrease in the prevalence of diabetes with increasing age in the present study could be due to a survival bias.
On an average, every fifth elderly person was identified as having impaired fasting blood glucose. This is a pre- diabetic condition. Its identification can facilitate early institution of dietary and lifestyle modifications and periodic monitoring of blood glucose levels. This may prevent or delay progression to diabetes in this group.
Awareness of their diabetes was found to be low among the participants of the present study. Only 36% were aware of their condition. This is low compared with that reported from Hong Kong (66%), and comparable to the one-third reported from Nepal.(14,15) However, 62.5% of those who were aware that they had diabetes were taking treatment. The awareness, treatment and control were better among women.
Among elderly persons, the prevalence of diabetes was found to be comparable to previous reported estimates. However, the awareness level in them regarding its presence was low. Screening, diagnosis and proper treatment of diabetes is required for elderly persons. Because they may be unable to visit the fixed health facility due to dependency on family members, etc., domiciliary visits by health staff may be considered for creating awareness and screening of this condition. The screening test for diabetes is relatively easy to perform. Training of health workers in screening and appropriate referral is a feasible option. Health education to increase awareness in the community on the preventive aspects of chronic conditions, especially lifestyle modification, is very important. Taking into account the increasing population of the urban slums in India, instituting mechanisms for serving the elderly persons living in them deserves adequate attention.
Strengthening primary health care services in urban slums, with special emphasis on the vulnerable population like elderly persons, is needed. Non-communicable diseases are a major cause of morbidity and mortality in this age group, and deserve special attention of policy makers and programme managers.
Footnotes
Source of Support: Nil,
Conflict of Interest: None declared
References
- 1.Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of diabetes: Estimates for the year 2000 and projections for 2030. Diabetes Care. 2004;27:1047–53. doi: 10.2337/diacare.27.5.1047. [DOI] [PubMed] [Google Scholar]
- 2.Geneva: World Health Organization; 2005. Preventing chronic diseases: A vital investment: WHO global report; p. 2. [Google Scholar]
- 3.Roglic G, Unwin N, Bennett PH, Mathers C, Tuomilehto J, Nag S, et al. The burden of mortality attributable to diabetes: Realistic estimates for the year 2000. Diabetes Care. 2005;28:2130–5. doi: 10.2337/diacare.28.9.2130. [DOI] [PubMed] [Google Scholar]
- 4.Registrar General and Census Commissioner of India, Census of India. 2001. [Last accessed on 2009 Oct 10]. Available from: http://www.censusindia.gov.in .
- 5.Health Information of India 2003; Central Bureau of Health Intelligence, Directorate General of Health Services, Ministry of Health and Family Welfare, Government of India. [Last accessed on 2009 Oct 11]. Available from: http://cbhidghs.nic.in/hii2003/chap2.asp .
- 6.Wild SH, Smith FB, Lee AJ, Fowkes FG. Criteria for previously undiagnosed diabetes and risk of mortality: 15-year follow-up of the Edinburgh Artery Study cohort. Diabet Med. 2005;22:490–6. doi: 10.1111/j.1464-5491.2004.01433.x. [DOI] [PubMed] [Google Scholar]
- 7.Ross NA, Gilmour H, Dasgupta K. 14-year diabetes incidence: The role of socio-economic status. Health Rep. 2010;21:19–28. [PubMed] [Google Scholar]
- 8.Anand K, Shah B, Yadav K, Singh R, Mathur P, Paul E, et al. Are the urban poor vulnerable to non-communicable diseases? A survey of risk factors for non-communicable diseases in urban slums of Faridabad. Natl Med J India. 2007;20:115–20. [PubMed] [Google Scholar]
- 9.Srivastava RK. Multicentric study to establish epidemiological data on health problems in elderly. A Government of India and WHO Collaborative Programme Ministry of Health and Family Welfare, Government of India. 2007 [Google Scholar]
- 10.Definition and diagnosis of diabetes mellitus and intermediate hyperglycemia. Report of a WHO/IDF consultation. 2006. [Last accessed on 2009 Oct 10]. Available from: http://whqlibdoc.who.int/publications/2006/9241594934_eng.pdf .
- 11.Puri S, Kalia M, Swami HM, Singh A, Abhimanyu, Mangat C, et al. Profile of diabetes mellitus in elderly of Chandigarh, India. The Internet Journal of Endocrinology. 2007;4 [Google Scholar]
- 12.Gupta HL, Yadav M, Sundarka MK, Talwar V, Saini M, Garg P. A study of prevalence of health problems in asymptomatic elderly individuals in Delhi. J Assoc Physicians India. 2002;50:792–5. [PubMed] [Google Scholar]
- 13.Porapakkham Y, Pattaraarchachai J, Aekplakorn W. Prevalence, awareness, treatment and control of hypertension and diabetes mellitus among the elderly: The 2004 National Health Examination Survey III, Thailand. Singapore Med J. 2008;49:868–73. [PubMed] [Google Scholar]
- 14.Kung AW, Janus ED, Lau CP. The prevalence of diabetes mellitus and its effect in elderly subjects in Hong Kong. Hong Kong Med J. 1996;2:26–33. [Google Scholar]
- 15.Chhetri MR, Chapman RS. Prevalence and determinants of diabetes among the elderly population in the Kathmandu Valley of Nepal. Nepal Med Coll J. 2009;11:34–8. [PubMed] [Google Scholar]