

Abstract
Inversely planned intensity-modulated radiotherapy (IMRT) and stereotactic small field radiotherapy should be verified before treatment execution. A second verification is carried out for planned treatments in IMRT and 3D conformal radiotherapy (3D-CRT) using a monitor verification commercial dose calculation management software (DCMS). For the same reference point the ion-chamber measured doses are compared for IMRT plans. DCMS (Diamond) computes dose based on modified Clarkson integration, accounting for multi-leaf collimators (MLC) transmission and measured collimator scatter factors. DCMS was validated with treatment planning system (TPS) (Eclipse 6.5 Version, Varian, USA) separately. Treatment plans computed from TPS are exported to DCMS using DICOM interface. Doses are re-calculated at selected points for fields delivered to IMRT phantom (IBA Scanditronix Wellhofer) in high-energy linac (Clinac 2300 CD, Varian). Doses measured at central axis, for the same points using CC13 (0.13 cc) ion chamber with Dose 1 Electrometer (Scanditronix Wellhofer) are compared with calculated data on DCMS and TPS. The data of 53 IMRT patients with fields ranging from 5 to 9 are reported. The computed dose for selected monitor units (MU) by Diamond showed good agreement with planned doses by TPS. DCMS dose prediction matched well in 3D-CRT forward plans (0.8 ± 1.3%, n = 37) and in IMRT inverse plans (–0.1 ± 2.2%, n = 37). Ion chamber measurements agreed well with Eclipse planned doses (–2.1 ± 2.0%, n = 53) and re-calculated DCMS doses (–1.5 ± 2.6%, n = 37) in phantom. DCMS dose validation is in reasonable agreement with TPS. DCMS calculations corroborate well with ionometric measured doses in most of the treatment plans.
Keywords: Diamond software, dose accuracy in RT, IMRT verification, ionometry
Introduction
3D conformal, intensity-modulated (IMRT) and stereotactic treatments are executed using multi-leaf collimators (MLC) in linear accelerators. Intensity modulation in the beamlets is achieved by irradiation of multiple beam directed field segmental irradiation (step and shoot IMRT) and dose delivered by dynamic motion of collimator leaves (dynamic IMRT). Inverse planning software ensures planned dose delivery based on the constraints on the uniformity of dose in Planning Target Volume (PTV) and protection of normal tissue/risk organs to lower limits of dose. There are some mishaps reported in the recent past, in dose delivery with complex treatment plans, and recommendations were made to practice stringent quality assurance (QA) methods.[1–4] Therefore, it is needed to have process management in the department for pre-treatment validation for complex treatment plans.[5] Commercial phantoms and film verification methods are practised for dose verification and energy fluence patterns. 3D-dose display methods using gel dosimetry have also been reported, because of tissue equivalence and high spatial resolution.[6]
To avoid incorrect dose delivery to the patient, the actual monitor units (MU) delivered by the machine by each radiation field should be checked. Intensity modulation in the beamlets is achieved by irradiation of multiple beam directed fields, segmental irradiation, and dose delivered by dynamic motion of collimator leaves. Accuracy of delivery of dose during IMRT needs confirmation.[7,8] Inverse planning software ensures planned dose delivery based on the constraints on the uniformity of dose in PTV and protection of normal tissue/risk organs to lower limits of dose.
Beam configuration and collimation properties of the treatment machines in treatment planning systems (TPS) ensure correctness of dose delivery planned by them.[9] Still there is a need to verify the computer plans and check the number of MU delivered to the patient, which are carried out by in-house developed software, excel spreadsheets, or commercial softwares.[10–12] It is also recommended to use an independent MU or dose calculation methods as a routine QA. MU calculation softwares work based on physical effects which are accurately described and handled by an independent set of algorithms. They are able to verify multiple beams, by importing treatment plan from TPS through record and verify system.
For IMRT treatments, for all the patients, we follow pre-treatment verifications using ionometric method in solid phantom. Film exposures and verifications have been carried out for all patients in the first two years, but because of difficulties in development of films, reproducibility and calibration problems, we discontinued film verification method. In the above context, we want to develop a compulsory check to routinely perform MU verification by a separate software, in addition to dose measurements in phantom.
Materials and Methods
Treatment planning and MU verification
The accuracy of dose computation by Eclipse TPS is independently checked by a Dose Calculation Management Software (DCMS) (Diamond, K and S Associates Inc, Nashville, USA). “Diamond” performs calculation based on modified Clarkson method, which integrates the primary and the scatter components of the radiation dose to a point from all individual and segmental subfields. Photon beam data, scatter factors, off-axis factors, MLC leaf transmission and tray factors for each energy are configured in the system during commissioning of DCMS.
The treatment plans generated by TPS are exported to DCMS using DICOM interface. For validation of DCMS, the IMRT phantom is configured in and doses delivered to phantom are verified for open fields, physical wedge fields, and blocked fields, for the calculated doses at reference points in the central and off-axis of the individual beams. The 6 MV photons from high energy linac (2300 CD), low-energy linac (600 CD), and 15 MV photon beams are examined. The effect of source to skin distances (SSD) (110 cm, 125 cm) and the effect of blocked fields (both by physical blocks and MLC) are also examined.
3D-conformal radiotherapy (3D-CRT) and IMRT treatments are carried out with 6 MV and 15 MV photons in Clinac 2300 CD (Varian, Palo Alto, USA). For IMRT, sliding window technique with MLC (millennium 120 MLC) is used. Eclipse TPS (Varian) (6.5 Version) with inverse planning (Helios) optimization software is used for generating IMRT treatment plans. For IMRT, the doses at reference points from individual segments are calculated for the entire treatment delivery, taking information of leaf movements for delivered intensity profile consisting of linear segment files generated at Eclipse. Calculated and measured doses for a given number of MUs are compared for 3D-CRT (n = 37) and IMRT (n = 53) patients, with the number of fields in each plan ranging up to nine.
Doses are measured for sliding window dose delivery at central axis with CC13 (0.13 cc) ion chamber with Dose 1 Electrometer in IMRT phantom (IBA, Scanditronix, Nurenberg). Doses at corresponding points are checked for the same MUs using Diamond Software.
Results
DCMS calculations showed good agreement (within 2%) with Eclipse TPS for open fields, wedged fields, changed SSD, and blocked fields for both 6 MV and 15 MV photons [Tables 1–5]. For large wedge angle physical wedges (45°, 60° wedge angles), the deviations in calculated doses appear to be more. Also, it is seen that the central axis reference points (CAx) showed better comparison in delivered doses, compared to off-axis reference points (OAx). Effects of SSD are addressed well by DCMS in the calculations. Doses from irregular fields, both by physical blocks and MLC, are calculated properly by DCMS.
Table 1.
Comparison of calculated dose by DCMS (open fields)
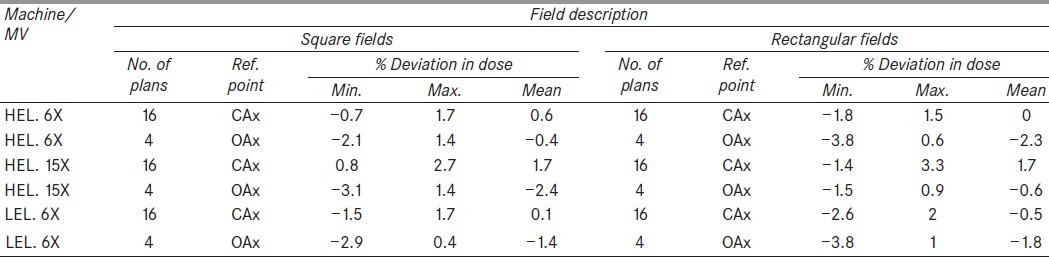
Table 5.
Comparison of calculated doses for irregular shaped fields (blocks and MLC shaping)
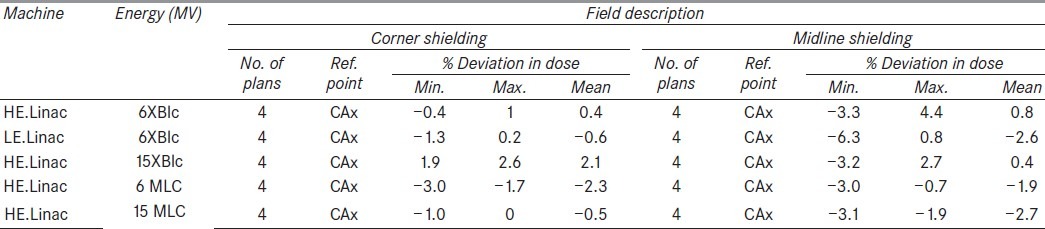
Table 2.
Comparison of calculated dose for 6 MV by DCMS (physical wedge fields)
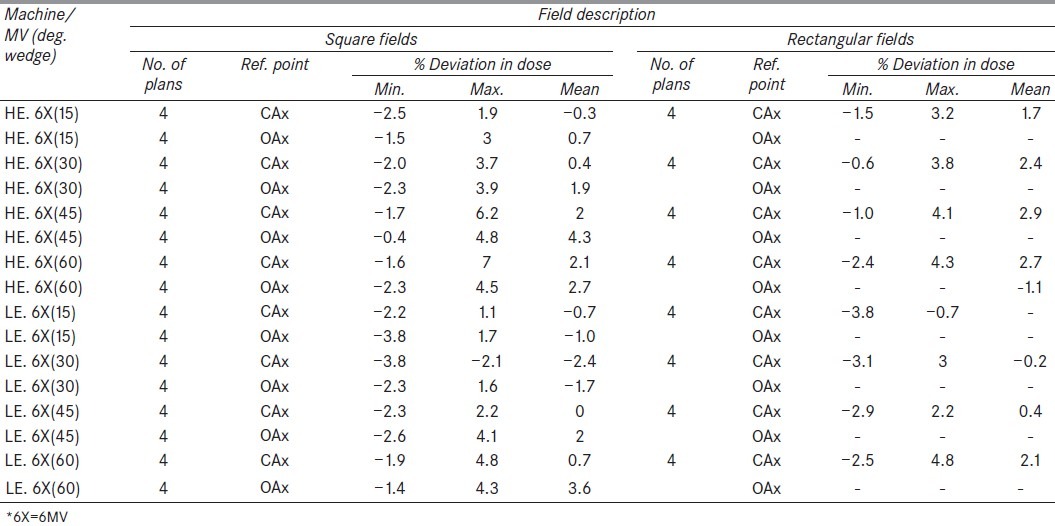
Table 3.
Comparison of calculated dose for 15 MV by DCMS (physical wedge fields)
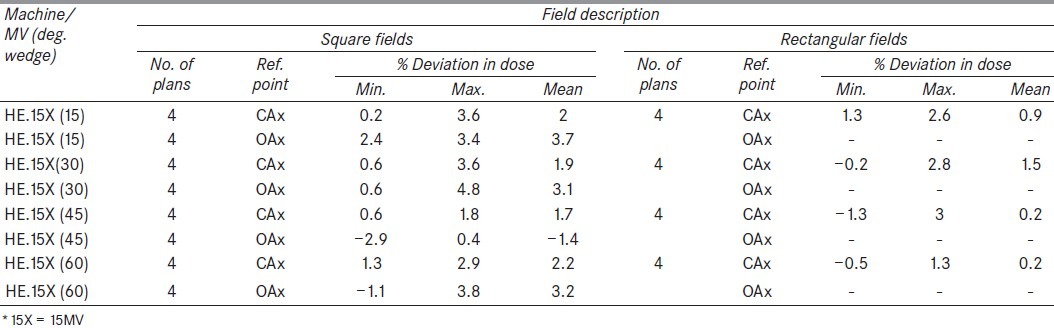
Table 4.
Comparison of calculated doses for changed source skin distances

In the patient treatment plans, the computed dose for selected MUs by Diamond showed good agreement [Table 6] with planned dose by Eclipse in 3D-CRT forward plans (0.8 ± 1.3%, n = 37), and in IMRT inverse plans (–0.1 ± 2.2%, n = 37). Ionometric measurements carried out at central axis reference points agreed well with Eclipse planned doses (–2.1 ± 2.0%, n = 53) and with DCMS calculated doses (–1.5 ± 2.6%, n = 37). The measured doses in the department using CC13 chamber showed good agreement with planned dose, within 2%. A few narrow segmental fields showed more deviation in measurements, but the same fields showed less deviation in DCMS.
Table 6.
Comparison of calculated doses (Eclipse and DCMS) and measured doses

Discussion
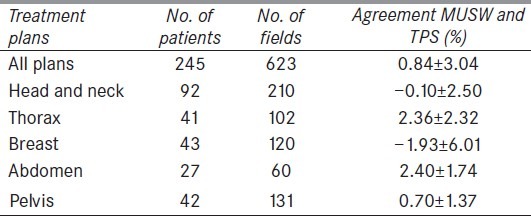
The objective of our present work is to validate the Diamond MU management software and to implement it for routine use in the department for verification of plans generated by the TPS. Efficacy of independent MU verification software (based on semi-analytical models) was highlighted in a recent publication.[11] A Matlab-based software (MUV) showed good efficacy in its application at five well-established radiotherapy centers in Europe. For IMRT plans, they reported mean deviations of –1.0 ± 7.3% (for dynamic) and –1.3 ± 3.2% (for step and shoot). Our results for IMRT indicated an agreement of dose with mean deviation of –0.1 ± 2.2%. Another study on Diamond software[12] reported agreement with (TPS) Eclipse on an average deviation of 0.4 ± 0.8% (1 SD) and an average deviation of –0.1 ± 0.7% (1 SD) in ion-chamber measurements. In another study,[12] a commercial RadCalc software package was validated with Plato TPS for 3D-CRT. The results of their study[13] are highlighted in Table 7. Our 3D-CRT results (0.8 ± 1.3%, n = 37 for Diamond and Eclipse) compare with their mean values of deviation 0.84 ± 3.04% for n = 245 (for RadCalc and Plato). The Diamond MU software calculated doses based on equivalent path length method which is comparable to the softwares used in their study. Our reported plans do not include breast tangential with more variations in body contours. In the present study, for a few patients’ DCMS, we could not calculate doses if there were split fields or isocentre gets blocked from primary beam.
Table 7.
Comparison of calculated doses on other MU check software[13]
Our ionometric measured doses with compact chamber CC13 in IMRT phantom compared well with Eclipse calculated doses (–2.1 ± 2.0%, n = 53) and DCMS calculated doses (–1.5 ± 2.6%, n = 37). This implies the need for a parallel system to independently verify in case of discrepancy in measurement or changes in calibration of detectors, which is a crucial element in pre-treatment approval of complex plans. An earlier report by Dobaldo et al.[14] estimated uncertainty in IMRT absolute dosimetry with ionization chambers (IC) around 1–1.5%, under non-reference conditions. They recommend an action level of 5% when IMRT pre-treatment validation is carried out with IC measurements. To bring down the uncertainty in measurements with small segmental fields, a suggested method[15] makes use of analytical output factors, validated by small volume diamond detector. The American Association of Physicists in Medicine Task Group report[16] outlined a word of caution that because MU verification software often performs dose estimations using a simpler geometrical model and calculation algorithm than the primary calculation, exact or almost exact agreement between the two can no longer be expected.
DCMS dose validation is in reasonable agreement with TPS. DCMS calculations corroborate well with ionometric measured doses in most of the treatment plans. The data presented in this work indicate that we can use DCMS in addition to the relative and absolute dosimetry for IMRT plan validations.
Acknowledgments
The authors thank Head, Department of Radiation Oncology, and Director General, Royal Hospital, for their kind permission for submission of the manuscript.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Bogdanich W, Robelo KA. A report. New York Times; 2010. A pin point beam strays invisibily, harming instead of healing; p. 28. [Google Scholar]
- 2.International Atomic Energy Agency ‘Lessons learnt from Accidental Exposures in Radiotherapy”. (Vienna-IAEA): IAEA SRS-17; 2000. [Google Scholar]
- 3.“Prevention of accidental exposures to patients undergoing radiation therapy.”. New York: Pergamon: ICRP Publication; 2000. International Commission on Radiological Protection; p. 86. [DOI] [PubMed] [Google Scholar]
- 4.ICRP. Preventing Accidental Exposures from New External Beam Radiation Therapy Technologies. 112. Ann. ICRP 39 (4) New York: Pergamon: ICRP Publication; 2009. [DOI] [PubMed] [Google Scholar]
- 5.Ravichandran R, Bhasi S, Binukumar JP, Davis CA. Need of patient specific quality assurance and pre-treatment verification program for special plans in radiotherapy. J Med Phys. 2011;36:181–3. doi: 10.4103/0971-6203.83501. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Shreiner LJ. Where does gel dosimetry fit in the clinic? J Phys Conf Serv. 2009;164:012001. [Google Scholar]
- 7.Sivakumar SS, Krishnamurthy K, Davis CA, Ravichandran R, Kannadhasan S, Binukumar JP, et al. Implementation of dynamic intensity-modulated radiotherapy: Dosimetric aspects and initial experience. J Med Phys. 2008;33:64–7. doi: 10.4103/0971-6203.41195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Ravichandran R, Binukumar JP, Sivakumar SS, Krishnamurthy K, Davis CA. A method for estimation of accuracy of dose delivery with dynamic slit windows in medical linear acclererators. J Med Phys. 2008;33:127–9. doi: 10.4103/0971-6203.42768. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Commissioning and quality assurance of computerized planning systems for radiation treatment planning systems for radiation treatment of cancer. Vienna: IAEA; 2004. International Atomic Energy Agency Technical Report Series No. 430. [Google Scholar]
- 10.Ayyangar KM, Nehru R, Li S, Djajaputra D, Pillai S, Fung A, et al. Independent IMRT Dose calculation methods. Int Conf Med Phys Radiat Saf. 2005;30:81–6. [Google Scholar]
- 11.Georg D, Nyholm T, Olofsson J, Kjaer-Kristoffersen F, Schnekenburger B, Winkler P, et al. Clinical evaluation of monitor unit software and the application of action levels. Radiother Oncol. 2007;85:306–15. doi: 10.1016/j.radonc.2007.04.035. [DOI] [PubMed] [Google Scholar]
- 12.Mata Colodro F, Serna Berná A, Puchades Puchades V. Dosimetric validation of a redundant independent calculation software for VMAT fields. Phys Med. 2012 doi: 10.1016/j.ejmp.2012.05.003. PMD 22658464. [DOI] [PubMed] [Google Scholar]
- 13.Sellakumar P, Arun C, Sanjay SS, Ramesh SB. Comparison of monitor units calculated by radiotherapy planning system and an independent monitor unit verification software. Phys Med. 2011;27:21–9. doi: 10.1016/j.ejmp.2010.01.006. [DOI] [PubMed] [Google Scholar]
- 14.Sanchez-Dobaldo F, Hartman GH, Pena J, Capote R, Paiusco M, Rein B, et al. Uncertainty estimation in Intensity Modulated Radiotherapy absolute dosimetry verification. Int J Radiat Oncol Biol Phys. 2007;68:301–10. doi: 10.1016/j.ijrobp.2006.11.056. [DOI] [PubMed] [Google Scholar]
- 15.Sudhir K, Sharma SD, Mayya YS. An analytical representation of MLC shaped narrow photon beam output factors. Souvenir and book of abstracts. AMPICON. 2009;28:67–8. [Google Scholar]
- 16.Stern RL, Heaton R, Fraser MW, Goddu SM, Kirby TH, Lam KL, et al. Verifications of monitor unit calculations for non-IMRT clinical radiotherapy. Report of AAPM task group 114. Med Phys. 2011;38:504–30. doi: 10.1118/1.3521473. [DOI] [PubMed] [Google Scholar]