

Abstract
Intracranial schwannomas most commonly occur in relation to vestibular nerves followed by trigeminal nerves. Authors describe a very unusual case of schwannomas originating in lateral recess of the fourth ventricle. Tumor was completely excised micro-surgically via midline suboccipital craniectomy and C1 laminectomy. Dissection of the surgical specimen revealed that the tumor was completely free from surrounding structures and just hanging in the fourth ventricle. It was not attached to any cranial nerves, brain parenchyma, and blood vessel or to the dura mater. Histopathological examination confirmed the diagnosis of schwannoma. To our knowledge, no such case has been reported so far from this extremely rare location. Relevant literature is reviewed and hypothesis for ectopic location of these tumors has been highlighted.
Keywords: Lateral recess, posterior fossa, schwannomas
Introduction
Schwannomas are benign neoplasms of the peripheral nerve sheath and are believed to have their origin in embryonic neural crest cells. Intracranial schwannomas occur most commonly in relation to vestibulocochlear nerve and constitute about 8% of all intracranial tumors. Next common origin is in relation to trigeminal nerve and rarely in association with other cranial nerves. If it occurs in relation to other cranial nerves usually, it is associated with Von Recklinghauson's disease. Schwannomas have been reported from various unusual intracranial locations like cerebellum, fourth ventricle, sella, frontal lobe, brain stem, etc.[1–5] We report an extremely rare case of schwannomas originating in the lateral recess of fourth ventricle where it did not have any attachment to the surrounding structures. On reviewing literature, we have not come across with any other case from this location.
Case Report
This 30-year-old male patient presented to us with headache and episodes of giddiness on and off for past 4 to 5 months. He did not have any history of difficulty in walking or loss of unconscious. He did not have any evidence of Von Recklighauson's neurofibromatosis. Neurological examination was unremarkable except minimal left-sided cerebellar signs. His routine biochemical and hematological parameters were normal. Computed tomography scan revealed a posterior fossa mass in the region of left half of fourth ventricle and adjacent to middle cerebellar peduncle with perilesional edema, which was enhancing on contrast administration. Magnetic resonance imaging showed a solid mass occupying the left half of the fourth ventricle, which was isointense on T1 WI and hyperintense on T2 WI and brightly enhancing on gadolinium administration [Figures 1 and 2]. The mass was causing edema and pressure effect on middle cerebellar peduncle. Patient was operated via midline suboccipital craniectomy with removal of posterior arch of C1 and complete excision of tumor has been done. Tumor was visualized on lifting left cerebellar tonsil. It was well-encapsulated, grayish white, firm in consistency but easily breakable and vascular. Branches from posterior inferior cerebellar artery supplied the tumor, disconnection of which made tumor avascular. Initially, intratumoral decompression followed by microsurgical total excision of tumor has been done. Tumor was nowhere attached to any of the surrounding structure. Postoperative period was uneventful. He did not develop any hearing disturbance or lower cranial nerves symptoms like hoarseness or dysphagia and recovered well. He had minimal left cerebellar signs as before. He was discharged on 10th post-operative day. Postoperative CT scan showed complete excision of tumor [Figure 3] with residual edema in middle cerebellar peduncle. Histopathological examination confirmed the features of schwannomas [Figure 4].
Figure 1.

MRI brain with gadolinium, axial view, showing well-defined lesion in left lateral part of fourth ventricle with brilliant enhancement
Figure 2.
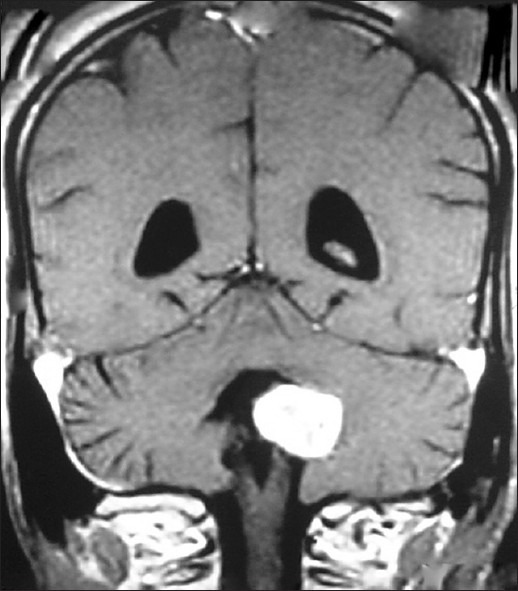
MRI brain with gadolinium, coronal view, showing welldefined tumor in lateral recess with part of the tumor free in 4th ventricle
Figure 3.
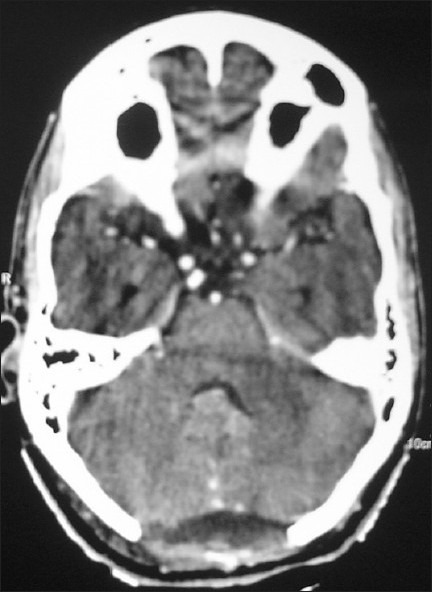
Postoperative contrast-enhanced CT scan, axial view, showing complete excision of tumor
Figure 4.
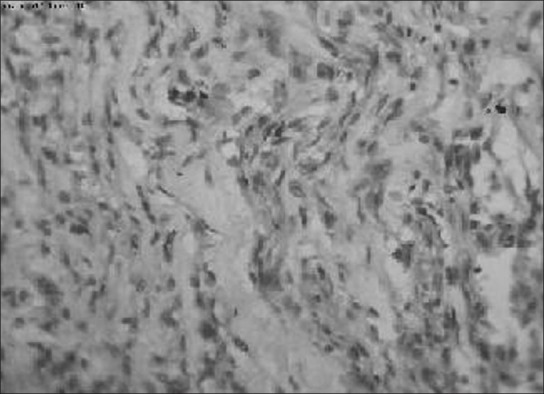
Photomicrograph showing typical palisading arrangement of schwannoma
Discussion
We present short report of schwannoma at a very rare site. The occurrence of a nerve sheath tumor in such a location raises the important question of its histogenesis. Various theories have been proposed for the origin of intraparenchymal schwannomas. Redekop et al. supported the theory of distorted embryogenesis,[4] while Riggs and Clary postulated that these tumors could arise from proliferation of Schwann cells in perivascular plexuses.[6] Russell and Rubenstein suggested that conversion of pial cells to Schwann cells was the possible mode of histogenesis.[7] Prakash et al. suggested misplaced myelinated nerve fibres as site of origin,[8] while Ramamurthi et al,[9] suggested displaced neural crest cells in the developing nervous system to be the origin of these tumors. Differentiation from multipotent mesenchymal cells has also been suggested. Some cases associated with neurofibromatosis have been reported. We believe that the origin of the tumor in the present case is most easily explained by the theory of distorted extra-cerebral ectopic neural crest cell migration with subsequent neoplastic transformation. The other possibilities being the origin from Schwann cells in the perivascular plexus or misplaced myelinated nerve fibers not attached to any of the cranial nerves.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Bhatjiwale M, Gupta S. Midline cerebellar cystic schwannoma: a case report. Neurol India. 1999;47:127–9. [PubMed] [Google Scholar]
- 2.Ladouceur D, Bergeron D, Lamarche JB, Lamontagne L. Cystic schwannoma of the brain stem. Can J Neurol Sci. 1989;16:357–60. doi: 10.1017/s0317167100029243. [DOI] [PubMed] [Google Scholar]
- 3.Mirone G, Natale M, Scuotto A, Rotondo M. Solitary olfactory groove schwannoma. J Clin Neurosci. 2009;16:454–6. doi: 10.1016/j.jocn.2008.04.020. [DOI] [PubMed] [Google Scholar]
- 4.Redekop G, Elisevich K, Gilbert J. Fourth ventricular schwannoma. A case report. J Neurosurg. 1990;73:777–81. doi: 10.3171/jns.1990.73.5.0777. [DOI] [PubMed] [Google Scholar]
- 5.Whee SM, Lee JI, Kim JH. Intrasellar schwannoma mimicking pituitary adenoma: A case report. J Korean Med Sci. 2002;17:147–50. doi: 10.3346/jkms.2002.17.1.147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Riggs H, Clary W. A case of intramedullary sheath cell tumour of the spinal cord. Consideration of vascular nerves as a source of origin. J Neuropathol Exp Neurol. 1957;16:332–6. doi: 10.1097/00005072-195707000-00004. [DOI] [PubMed] [Google Scholar]
- 7.Russell D, Rubinstein L. Pathology of tumours of the nervous system. 4th ed. London: Edward Amold; 1977. pp. 372–9. [Google Scholar]
- 8.Prakash B, Roy S, Tandon P. Schwannoma of the brain stem: Case report. J Neurosurg. 1980;53:121–3. doi: 10.3171/jns.1980.53.1.0121. [DOI] [PubMed] [Google Scholar]
- 9.Ramamurthi B, Anguli V, Iyer C. A case of intramedullary neurinoma. J Neurol Neurosurg Psychiatry. 1958;21:92–4. doi: 10.1136/jnnp.21.2.92. [DOI] [PMC free article] [PubMed] [Google Scholar]