

Abstract
Dentigerous cysts are the most common type of developmental odontogenic cysts arising from the crowns of impacted, embedded, or unerupted teeth. They constitute about 20% of all epithelium-lined cysts of the jaws. The teeth involved most often are mandibular third molar and maxillary canines. About 70% of dentigerous cysts occur in the mandible and 30% in the maxilla. Dentigerous cysts associated with ectopic teeth within the maxillary sinus are fairly rare, and only 20 cases had been reported in Medline since 1980. In the present paper, we report an additional case of dentigerous cysts associated with ectopic third molar in the right maxillary sinus. Also, pathogenesis of ectopic tooth, role of advanced imaging, differential diagnosis, and management are discussed.
Keywords: Dentigerous cyst, ectopic tooth, maxillary sinus, third molar
Introduction
The term “dentigerous cyst” was coined by Paget in 1853. These cysts are the most common type of developmental odontogenic cysts arising from the crowns of impacted, embedded, or unerupted teeth.[1] They constitute the second most common cystic lesion of the jaws, after radicular cysts.[2] The literal meaning of dentigerous is ‘tooth bearing.’[3] They are most frequently associated with the crowns of permanent teeth, though few rare cases are reported in association with the crowns of deciduous tooth,[4] complex odontoma,[5] and supernumerary teeth.[6,7] Dentigerous cysts associated with supernumerary teeth constitute 5-6% of all dentigerous cysts and about 90% are associated with a maxillary mesiodens.[6]
The most reasonable theory to explain its pathogenesis appears to be that the cyst is the result of the accumulation of fluid between an unerupted tooth and the surrounding reduced enamel epithelium. They are two times common in males than in females. About 70% of dentigerous cysts occur in the mandible and 30% in the maxilla. The mandibular third molar and maxillary canines are involved most often, followed by the mandibular premolars and the maxillary third molar.[8]
Dentigerous cyst associated with an ectopic tooth within the maxillary sinus is fairly rare, and only 20 cases had been reported in Medline since 1980 including the 3 cases reported by Buyukkurt et al.[9] who reviewed the literature reports of this condition from 1980 to 2009. In the present paper, we report an additional case of dentigerous cysts associated with an ectopic third molar in the right maxillary sinus.
Case Report
A 22-year-old unmarried male reported to the dept. of Oral Medicine and Radiology, with the chief complaint of pus discharge from upper right posterior region of jaw and right nostril since last 3 years. Detailed history revealed that it started as pus discharge from oral cavity 3 years back, for which he took medicines from a general physician for over a year. But, no permanent relief was obtained, and condition further deteriorated when pus discharge from right nostril started 6 months back. Later on, he consulted a dentist for the problem who prescribed medicines for a week. As there was no relief, he referred him to our dental college.
Extra-oral examination revealed presence of diffuse, soft, tender swelling over right maxillary sinus [Figure 1]. Intra-oral examination revealed absence of the upper right third molar. Pus discharge was evident from distal aspect of upper right second molar, on application of pressure with finger in buccal vestibule in that region. A provisional diagnosis of infected right maxillary sinus was considered.
Figure 1.
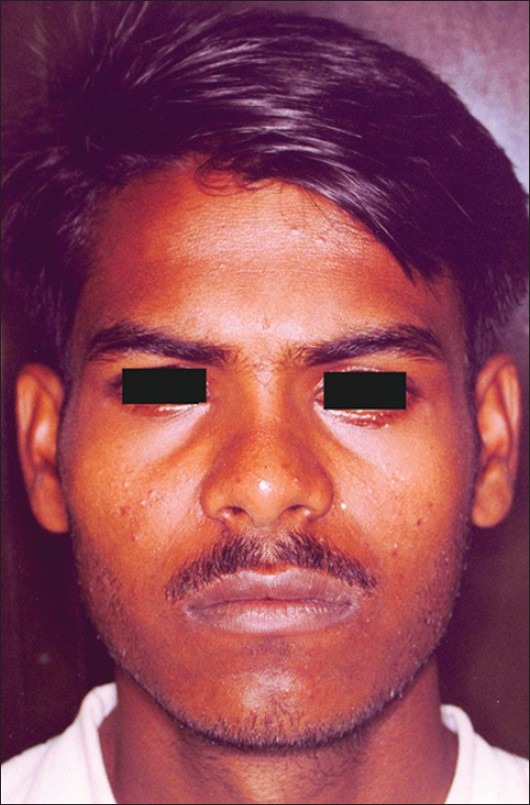
Extra-oral photograph showing diffuse swelling over right maxillary sinus
Radiographic evaluation included IOPA of the upper right second molar, OPG, Waters view, lateral cephalogram, and CT scan. OPG revealed upper right third molar in the maxillary sinus near its posterosuperior aspect [Figure 2]. On CT scan examination, a cystic expansile lesion was seen in the right maxillary sinus with the crown of an unerupted tooth within it. Bony defect was seen in its inferior wall allowing the cyst to communicate with the roof of the oral cavity. [Figure 3].
Figure 2.

OPG showing impacted third molar in the right maxillary sinus near its posterosuperior aspect
Figure 3.
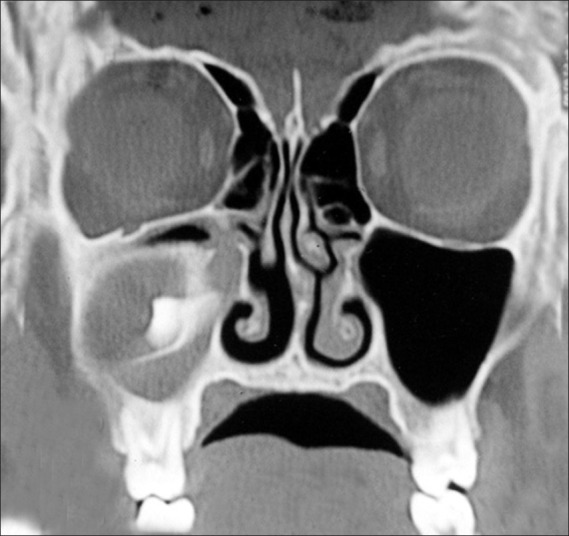
Coronal CT image showing expansile cystic lesion surrounding crown of impacted molar in the right maxillary sinus
Incisional biopsy report was indicative of dentigerous cyst. Patient was referred to Maxillo-facial Surgery department where enucleation of cystic lesion under GA was carried out via the Caldwell-Luc approach, and tissue was sent for histopathological examination, which confirmed the finding of incisional biopsy report [Figure 4]. Post-operative healing was uneventful, and patient was followed-up over a period of next 2 years and was asymptomatic [Figures 5 and 6].
Figure 4.
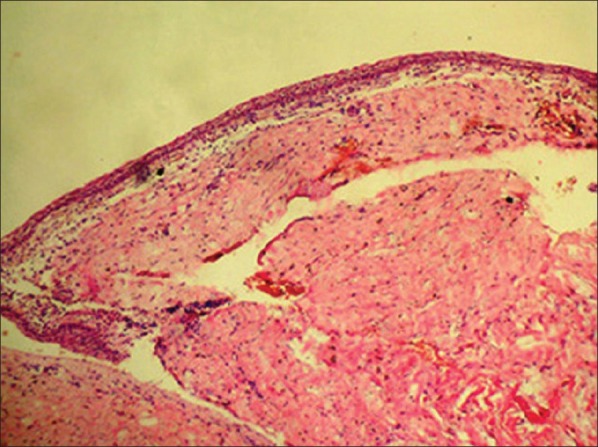
Photomicrograph showing the cystic lesion lined by non-keratinized squamous epithelium
Figure 5.

Post-operative photograph
Figure 6.

Post-operative OPG
Discussion
Ectopic teeth are those located in the jawbones or regions other than the alveolar arch. Ectopic eruption of a tooth is rare; however, there have been few reports of tooth in the nose,[10] mandibular condyle,[11] coronoid process,[12] and maxillary sinus,[9] which is also the largest of the paranasal sinuses.
Ectopic eruption may occur as a result of 1 of 3 distinct processes described below,[13] or it may be idiopathic.
Disturbance in tooth developmental
Odontogenesis is a complex process, and abnormal tissue interactions between the oral epithelium and the underlying mesenchymal tissue during development may potentially result in ectopic tooth development and eruption.[14]
Pathological process
It is believed that the displacement of tooth buds by the expansion of progressively growing dentigerous cysts results in the displacement of the tooth to other areas. In the present case, etiologic factor was also dentigerous cyst.
Iatrogenic activity:
During the extraction of the third molar, an iatrogenic displacement into the maxillary antrum can occur. Bonder et al.[13] have mentioned a case of an iatrogenic displacement of the upper right third molar into the maxillary antrum in a 40-year-old female during the extraction of that tooth.
Though cases of dentigerous cysts are reported in children,[15,16] they are usually present in the second or third decade of life and are rare in childhood. The incidence is higher in males than in females (M: F-1.84: 1).[8] Dentigerous cysts are usually single lesions. Multiple and bilateral cysts have been reported in patients with syndromes such as basal cell nevus syndrome, mucopolysaccharidosis,[17] and cleidocranial dysplasia[18] as well as in a non-syndromic patient.[16]
The dentigerous cyst progresses slowly and may exist for several years without being noticed. When the maxillary sinus is invaded, symptoms usually occur late in the process. It can cause headache,[19] obstruction of the sinus,[20] epiphora due to nasolacrimal duct obstruction,[21] recurrent sinusitis,[22] purulent rhinorrhea,[14] elevation of the orbital floor,[23] and fractures.[24] Impingement of this lesion on the orbital floor can cause diplopia and possibly even blindness.[25]
On radiographic examination, dentigerous cysts appear as unilocular radiolucencies of varying sizes, with well-defined sclerotic borders, associated with the crown of an unerupted tooth. If a follicular space on radiography is more than 5 mm, an odontogenic cyst can be suspected.
Water view, OPG, and lateral cephalogram are simple and inexpensive projections for radiographic evaluation of an ectopic tooth in the maxillary sinus. Though expensive, CT and MRI certainly have an edge over conventional radiographs. CT scan provides superior bony detail, help in determination of the size and extent of the lesion, and is useful to distinguish a maxillary lesion of antral origin from an extra-antral lesion.[24] Bonder et al.[13] studied 12 patients with teeth in the maxillary sinus by plain film radiography (PFR) and by CT with a dental software programme. He found that CT was superior to PFR to determine proximity of the tooth to the sinus wall or its ankylosis, proper surgical planning (crestal incision or Caldwell-Luc approach), as well as prediction of prognosis or complications.
Ustuner et al.[16] provided MRI findings of the cystic lesion, which appears homogeneously hypointense on T1-weighted images and hyperintense on T2-weighted images. The impacted tooth appears hypointense on all sequences. Chronic secretions, air, and acute hemorrhage in the sinus may also appear hypointense, but their central location in the sinus distinguishes them from tooth, which lies eccentrically in the cyst wall.
The differential diagnosis of a dentigerous cyst includes unicystic ameloblastoma, adenomatoid odontogenic tumor (AOT), early stages of Gorlin cyst/calcifying epithelial odontogenic tumor (CEOT), ameloblastic fibroma, ameloblastic fibro-odontoma, and odontogenic keratocyst. Unicystic ameloblastoma is seen in persons under the age of 30 years, occurs equally in both genders, and has a tendency to occur in posterior mandible associated with the crown of an unerupted third molar. AOT is common in second decade, affects females twice as often as males, has a striking tendency to occur in the anterior maxilla and in about 74% of cases associated with the crown of an unerupted canine. However, AOT of the maxillary antrum is extremely rare. Gorlin cyst is commonly found in the incisor and canine area (65% of cases). Approximately one third of cases are associated with an unerupted tooth, most often a canine. CEOT is an uncommon lesion, which is most often encountered between third to fifth decades, occurs equally in both genders, and has a tendency to occur in posterior mandible associated with an impacted third molar. Ameloblastic fibroma is an uncommon tumor, occurs in first two decades, more common in males, commonly found in posterior mandible, and is associated with an unerupted tooth in about 75% of cases. Ameloblastic fibro-odontoma often occurs in the maxilla associated with an impacted tooth. However, the ameloblastic fibro-odontoma is rarely found within the maxillary sinus and usually occurs in persons under the age of 20. Odontogenic keratocyst may be found in patients from infancy to old age, commonly found in posterior body and ascending ramus of mandible, and in 25% to 40% of cases, unerupted tooth is involved.
Histologically, dentigerous cysts are lined by a layer of non-keratinized stratified squamous epithelium, with a surrounding wall of thin connective tissue containing odontogenic epithelial rests. Cases of ameloblastoma or epidermoid carcinomas developing from the lining epithelium of a dentigerous cyst are adequately documented, whereas mucoepidermoid carcinomas are less well-documented.[26] Also, squamous cell carcinoma[27] may develop from the lining epithelium of a dentigerous cyst.
The standard treatment for a dentigerous cyst is enucleation and extraction of the associated tooth via a Caldwell-Luc procedure. In large cysts, an initial marsupialization to diminish the size of the osseous defect, followed by enucleation and tooth extraction, has been advocated. The major disadvantage of marsupialization is recurrence or persistence of the lesion. Endoscopic approach for its management is also described in the literature, which is associated with lesser operative as well as post-operative morbidity.[1]
In conclusion, occurrence of an ectopic tooth in the maxillary sinus and association of a dentigerous cyst with it is a rare phenomenon. Its presence may be asymptomatic initially with clinical manifestations, later on as adjacent structures are affected. Convention radiographs are sufficient for the diagnosis, but advanced imaging is useful for treatment planning.
Footnotes
Source of Support: Nil,
Conflict of Interest: None declared
References
- 1.Di Pasquale P, Shermetaro C. Endoscopic removal of a dentigerous cyst producing unilateral maxillary sinus opacification on computed tomography. Ear Nose Throat J. 2006;85:747–8. [PubMed] [Google Scholar]
- 2.Tournas A, Tewfik M, Chauvin P, Manoukian J. Multiple unilateral maxillary dentigerous cysts in a nonsyndromic patient: A case report and review of the literature. Int J Pediatr Otorhi Extra. 2006;1:100–6. [Google Scholar]
- 3.Browne RM, Smith AJ. Pathogenesis of odontogenic cysts. In: Browne RM, editor. Investigative Pathologyof the Odontogenic Cyst. Boca Ratonl: CRC Press; 1991. pp. 88–109. [Google Scholar]
- 4.Kusukawa J, Irie K, Morimatsu M, Koyanagi S, Kameyama T. Dentigerous cyst associated with a deciduous tooth: A case report. Oral Surg Oral Med Oral Pathol. 1992;73:415–8. doi: 10.1016/0030-4220(92)90317-j. [DOI] [PubMed] [Google Scholar]
- 5.Sales M, Cavalcanti M. Complex odontoma associated with dentigerous cyst in maxillary sinus: Case report and computed tomography features. Dentomaxillofac Radiol. 2009;38:48–52. doi: 10.1259/dmfr/95388644. [DOI] [PubMed] [Google Scholar]
- 6.Lustmann J, Bodner L. Dentigerous cysts associated with a supernumerary teeth. Int J Oral Maxillofac Surg. 1988;17:100–2. doi: 10.1016/s0901-5027(88)80159-0. [DOI] [PubMed] [Google Scholar]
- 7.Papadopoulos MS. An unusual case of a dentigerous cyst due to a mesiodens. Br J Oral Surg. 1981;19:307–8. doi: 10.1016/0007-117x(81)90053-6. [DOI] [PubMed] [Google Scholar]
- 8.Jones AV, Craig GT, Franklin CD. Range and demographics of odontogenic cysts diagnosed in a UK population over a 30-year period. J Oral Pathol Med. 2006;35:500–7. doi: 10.1111/j.1600-0714.2006.00455.x. [DOI] [PubMed] [Google Scholar]
- 9.Buyukkurt MC, Omezli MM, Miloglu O. Dentigerous cyst associated with an ectopic tooth in the maxillary sinus: A report of 3 cases and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;109:67–71. doi: 10.1016/j.tripleo.2009.07.043. [DOI] [PubMed] [Google Scholar]
- 10.Lin IH, Hwang CF, Su CY, Kao YF, Peng JP. Intranasal tooth: Report of three cases. Chang Gung Med J. 2004;27:385–9. [PubMed] [Google Scholar]
- 11.Yusuf H, Quayle AA. Intracondylar tooth. Int J Oral Maxillofac Surg. 1989;18:323. doi: 10.1016/s0901-5027(89)80027-x. [DOI] [PubMed] [Google Scholar]
- 12.Toranzo Fernandez M, Terrones Meraz MA. Infected cyst in the coronoid process. Oral Surg Oral Med Oral Pathol. 1992;73:768. doi: 10.1016/0030-4220(92)90028-o. [DOI] [PubMed] [Google Scholar]
- 13.Bonder L, Tovi F, Bar-Ziv J. Teeth in the maxillary sinus - imaging and management. J Laryngol Otol. 1997;111:820–4. doi: 10.1017/s0022215100138721. [DOI] [PubMed] [Google Scholar]
- 14.Srinivasa Prasad T, Sujatha G, Niazi T, Rajesh P. Dentigerous cyst associated with an ectopic third molar in the maxillary sinus: A rare entity. Indian J Dent Res. 2007;18:141–3. doi: 10.4103/0970-9290.33793. [DOI] [PubMed] [Google Scholar]
- 15.O’Neil D, Mosby E, Lowe J. Bilateral mandibular dentigerous cysts in a five-year-old child: report of a case. ASDC J Dent Child. 1989;56:382–4. [PubMed] [Google Scholar]
- 16.Ustuner E, Fitoz S, Atasoy C, Erden I, Akyar S. Bilateral maxillary dentigerous cysts: A case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003;95:632–5. doi: 10.1067/moe.2003.123. [DOI] [PubMed] [Google Scholar]
- 17.Roberts M, Barton N, Constantopoulos G, Butler D, Donahue A. Occurrence of multiple dentigerous cysts in a patient with the Morateax-Lamy syndrome (mucopolysaccharidosis, type VI) Oral Surg Oral Med Oral Pathol. 1984;58:169–75. doi: 10.1016/0030-4220(84)90133-6. [DOI] [PubMed] [Google Scholar]
- 18.Trimble LD, West RA, McNeill RW. Cleidocranial dysplasia.Comprehensive treatment of dentofacial abnormalities. J Am Dent Assoc. 1982;5:661–6. doi: 10.14219/jada.archive.1982.0450. [DOI] [PubMed] [Google Scholar]
- 19.Freedland ES, Henneman PL. An unusual cause of headache: A dentigerous cyst in the maxillary sinus. Ann Emerg Med. 1987;16:1174–6. doi: 10.1016/s0196-0644(87)80481-x. [DOI] [PubMed] [Google Scholar]
- 20.Litvin M, Caprice D, Infranco L. Dentigerous cyst of the maxilla with impacted tooth displaced into orbital rim and floor. Ear Nose Throat J. 2008;87:160–2. [PubMed] [Google Scholar]
- 21.Ray B, Bandyopadhyay SN, Das D, Adhikary B. A rare cause of nasolacrimal duct obstruction: Dentigerous cyst in the maxillary sinus. Indian J Ophthalmol. 2009;57:465–7. doi: 10.4103/0301-4738.57161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Prabhu SP, Padwa BL, Robson CD, Rahbar R. Dentigerous cyst associated with a displaced tooth in the maxillary sinus: An unusual cause of recurrent sinusitis in an adolescent. Pediatr Radiol. 2009;39:1102–4. doi: 10.1007/s00247-009-1337-z. [DOI] [PubMed] [Google Scholar]
- 23.Golden AL, Foote J, Lally E, Beideman R, Tatoian J. Dentigerous cyst of the maxillary sinus causing elevation of the orbital floor- report of a case. Oral Surg Oral Med Oral Pathol. 1981;52:133–6. doi: 10.1016/0030-4220(81)90308-x. [DOI] [PubMed] [Google Scholar]
- 24.Han MH, Chang KH, Lee CH, Na DG, Yeon KM, Han MC. Cystic expansile masses of the maxilla: Differential diagnosis with CT and MR. AJNR Am J Neuroradiol. 1995;16:333–8. [PMC free article] [PubMed] [Google Scholar]
- 25.Savundranayagam A. Migratory third molar erupting into the lower border of orbit causing blindness in the left eye. Aust Dent J. 1972;17:418–20. doi: 10.1111/j.1834-7819.1972.tb04970.x. [DOI] [PubMed] [Google Scholar]
- 26.Rajendran R. Cysts and Tumors of Odontogenic Origin. In: Rajendran R, Sivapathasundharam B, editors. Shafer's Textbook of Oral Pathology. 5th ed. New Delhi: Elsevier Publishers; 2006. pp. 360–1. [Google Scholar]
- 27.Yasuoka T, Yonemoto K, Kato Y, Tatematsu N. Squamous cell carcinoma arising in a dentigerous cyst. J Oral Maxillofac Surg. 2000;58:900–5. doi: 10.1053/joms.2000.8219. [DOI] [PubMed] [Google Scholar]