

Abstract
Purpose
To examine Mexican-American immigrant caregivers’ beliefs and motivations surrounding the first dental visit for their young children (median age 5 years).
Methods
Qualitative interviews with a convenience sample of 48 low-income, Mexican-American mothers about their young children’s oral health. Transcripts were independently read, coded and thematically analyzed.
Results
Half (51%) of first dental visits were for parent-initiated reasons: for pain or visible dental problems, parent’s proactive desire to get a checkup, or to avoid future dental problems. The other half was initiated by external prompts, especially pediatrician recommendation and school requirement. Once a child went to the dentist for his/her first visit, 94% continued with regular checkups. The mean age for a first dental visit was 3 years. Three parents reported cases in which dentists discouraged visits for symptomatic children before 3 years of age.
Conclusions
These low-income, urban Mexican-American parents are taking their children to their first dental visit around 3 years of age, much later than the recommended 1 year for this at-risk population. Physicians are well-situated to play an important role in prompting first dental visits.
Keywords: Oral Health, Child, Preschool, Parent, Healthcare Disparities, Mexican Americans
BACKGROUND
FIRST DENTAL VISITS
Early dental visits for children help establish a “dental home,” recognize the early stages of early childhood caries before more invasive treatment is needed, and provide opportunity for parent education.1,2 Other research suggests that early dental visits result in fewer restorative needs, and therefore reduced cost for treatment later in life,2,3 and can lead to more positive views about dentists and dental visits.4 The American Dental Association (ADA) and American Academy of Pediatric Dentistry (AAPD) recommend that children have the first dental visit and establish a dental home by 12 months of age.5, 6
Despite these recommendations5,6, most at-risk children in the United States (U.S.) do not have their first dental visit before age 1 year. The age of first visit is generally much later; for example, in Iowa, only 2% of children had a dental visit by age 1, 11% by age 2, and 31% by age 3.7 Another study found that only 47% of low-income African American children in Detroit have ever visited a dentist by age 3.8 These late visits may be in part due to financial barriers to access and dental professional reluctance to treat very young children.7–13 There is very limited literature on parental beliefs, attitudes and motivation for first dental visits. A U.S. study found that caregiver factors such as own preventive care seeking positively influence child dental visit behavior.8 Two quantitative surveys of Saudi Arabian families concluded that parents do not have sufficient knowledge about when first dental visits should occur: 34% of parents thought the first visit should be during the child’s third year, while 42% thought it should be during the sixth year.14,15 The major reasons for a child’s first dental visit in those samples were regular visit (40%) and emergency (28%).14,15
LATINOS AND EARLY CHILDHOOD CARIES
Latino children have among the highest rates of early childhood caries (ECC), even when controlling for other variables such as income.16 Mexican-American school children in particular have higher ECC rates than other groups in both the United States generally, and California specifically.17
Reasons for this health disparity are not fully understood. Some research suggests that Mexican immigrant parents might have poor knowledge and practice of effective preventive measures,18,19 might not understand the relationship between the child’s diet and oral disease, might accord low value to primary teeth or might not recognize early signs of oral health problems in their children.20,21 Additionally, much research has pointed to barriers to access and dental utilization.22,23 There are no reports examining the age and motivation for first dental visits for Mexican-American children, factors that could be playing a role in this health disparity.
Using a basic social constructionist theoretical approach,24 this study sought to examine the meanings and practices of parents around first dental visits for their children. We inquired about the following research questions:
1.) What meanings, thoughts and beliefs surround low-income Mexican-American caregivers’ seeking of a first dental visit for their children? ; and 2.) What factors influenced the timing of a first dental visit?
METHODS
A qualitative approach was used to gain an understanding of urban Mexican-American parents’ knowledge, beliefs and practices surrounding their young children’s oral health, including first dental visit. The study was conducted in a low-income neighborhood with a high proportion of Mexican-American residents in San José, a large, city in northern California. The targeted county is classed as ‘high-risk for ECC’ with 51% of low-income children entering kindergarten with a history of cavities, and nearly one third having untreated decay.22
Eligible study participants were: (1) primary caregivers of children aged 10 or less, with the aim that the youngest child would be aged 5 years or less; (2) self-identified as first- or second- generation immigrants from Mexico. The convenience sample of participants was drawn from multiple sources in the community, including a migrant parents’ group, preschools, low-income dental clinics, community festivals, and referrals from other participants. Screening specifically for children who had caries experience was not undertaken. All data are self-reported; no data come from medical or dental records. No clinical examinations were made or treatments were offered, though referrals to local dental resources were provided upon request.
Bilingual interview staff recruited, screened and obtained informed consent from interested participants. A grocery store certificate of $20 was offered as an incentive to participants. All interviews were face-to-face and relied on open-ended questions and probes from a semi-structured interview guide approved by the institutional review board of the University of California, San Francisco. Interview questions were developed based on previous studies of Latino immigrant and low-income populations’ conceptions of oral disease and experiences with the oral health care system.16,17 Interviews documented caregivers’ conceptions of their children’s oral health and disease and related behaviors. Main questions that generated the data analyzed in this article include:
“When did you take your child to the dentist for the first time?”
“How old was he/she?”
“How did you decide/know that it was time to take him/her?”
Interviews were conducted in Spanish or English, digitally recorded, translated and transcribed; and all observations were recorded as typed field notes. Following standard qualitative analytic procedures,25,26 a short list of codes related to initiation of dental visits was developed and applied independently by two researchers using the NVivo® software package. After initial codes were applied to text, codes were iteratively refined as various themes emerged while re-reading transcripts and field notes.25,26
When parents mentioned multiple reasons prompting an initial dental visit, all were recorded, but in the following numeric results only the first reason was counted. The category of “school” includes both preschool and elementary school. Most parents did not specify the type of medical provider their child saw, so the categorization of “pediatrician” may also include general and family physicians. As each child in the family had a different oral health situation, parents usually went through their family child by child to detail to the interviewer all the oral health experiences her children had, including oral health habits, pain or problems, and encounters with dentists. Responses were categorized per child (as most families had multiple children). This enabled us to discern how parental actions and reasons for the first dental visits changed from first to subsequent children. Acknowledging that there are limitations to this approach, and in the absence of the ability to conduct a prospective study at this time, parents were asked to recall information, such as child’s age at first dental visit. Quotations provided below reflect typical sentiments and comments expressed by the caregivers in the course of the interview.
RESULTS
SAMPLE
The sample comprised 48 women – mothers – primarily from low-income (median annual income= $24,000); low-education (mean= 9 ± 2.8 years); immigrant families of Mexican origin or descent (100%). The average age of mothers was 31 years; about one third (35%) had health insurance; half (52%) came from rural areas; and, the majority (90%) were born in Mexico and had lived in the U.S. an average of 9 years. The majority (60%) of mothers self-reported having themselves a current need for dental treatment. Most participants (90%) preferred to use Spanish language and conducted their interview in Spanish.
As a group, these mothers had an average of 2.5 children per family. Most children (61%) were younger than 5 years of age and had been born in the U.S. (83%). Mothers reported caries experience for nearly two-thirds (64%) of these children. Over one-third (36%) of children under 5 years of age had older siblings with caries experience. The mean age for a child’s first dental visit was 3 ± 1.6 years. In the county studied, Santa Clara County, CA, all children regardless of legal or income status, had access to some form of dental insurance, though a small minority (3%) of undocumented children aged 6 or more were on the waitlist. Nearly all insured children (90%) were on public dental insurance programs.
MOTIVATIONS FOR FIRST DENTAL VISIT
A child’s first dental visit was motivated by two distinct sources: internal or external prompts (see Table 1). Half the mothers reported that their youngest child’s first dental visit was made for internal, parent-initiated reasons. These internal reasons were divided into 3 subcategories, one reactive and two proactive motivations. Half of the mothers initiated the child’s first dental visit because of external prompts. External prompts also comprised 3 subcategories. Once a child had gone into the dentist for whatever reason, almost all (94%, 67 out of 71) continued with regular checkups twice a year, many mothers specifically mentioning reminders from the dentist as the trigger prompting subsequent visits.
Table 1.
Main Reason for First Dental Visit (N=78 children), by Internal and External Prompt
| REASON | N | PROPORTION OF ALL REASONS (percent)* |
|---|---|---|
| INTERNAL PROMPT (Parent initiative) N = 40 |
51% | |
| Reactive: Parent-noticed pain/problem | 16 | 21% |
| Proactive: Parental desire for checkup and Parental avoidance of problem | 24 | 31% |
| EXTERNAL PROMPT N= 38 |
49% | |
| Pediatrician | 16 | 21% |
| School Requirement | 14 | 18% |
| Other | 8 | 10% |
Percentages total more than 100 percent due to rounding error
Internal Prompts
Reactive: Parent-Noticed Problems
The main reason for an internal prompt or parent-initiated first dental visit was reaction to a parent-noticed problem, such as tooth staining or crumbling, the child’s complaining of pain, or trauma. One caregiver explains how a visible problem prompted her to take her child to the dentist for the first time:
<respondent> Because I saw that my daughter’s teeth were going black and I didn’t want that to happen to her. That’s why I took her.
[child’s first dental visit at age 2 years]
Another caregiver explains how, even though the problem was noticed long before hand, it was her child’s pain complaints that motivated a first dental visit:
<interviewer> Okay, so tell me a little bit about the cavity problem...
<respondent> It was with the youngest, when he was about 2 years old. It started when he was about 2 years old, ever since he was little. They [his teeth] hurt him, and he cried and cried, and then when he was about 4, he started to say that it was his teeth that hurt him. And that’s when we started caring for his teeth.
<interviewer> What did you do?
<respondent> We took him to the dentist so that they could take care of the cavities and take out the bad teeth, ones that already had lots of cavities.
[child’s first dental visit at age 4 years]
Proactive: Parental Desires for Checkup
The next most common (40%, n=16) internal prompts were parental self-standards or proactive desires for a preventive visit.. Mostly, this comprised parents deciding it was time for a checkup or cleaning, and asking service providers when their child could see a dentist. For example:
<interviewer> How did you decide to bring her into the dentist the first time?
<respondent> I just thought it was time for her to go for her first cleaning.
[child’s first dental visit at age 3 years]
<interviewer>And how did you decide to take him to the dentist the first time?
<respondent> I asked about it when my [older] daughter had a [dental] appointment and I asked the [dentist] when I should bring him to the dentist for the first time, and he said that if I wanted to I could bring him any time, that he could see him. He already had Medi-Cal and everything…
[child’s first dental visit at age 2 years]
Six of these 16 proactive parental-desires-for-checkup cases were initiated because the parent had an older child and had learned about children’s dental needs through experiences with the older sibling. An example of one of those caregivers:
<interviewer> Ok, let’s move on to your youngest child, the 3-year-old.
<respondent> His first visit to the dentist was when he was 2 years old. He would want to go [to the dentist] when I took the others [older siblings]. I got an appointment for him at that same place, at the [clinic name]. I told them that he was two years old and they said they would see him. They gave him an appointment, I took him to it and I think it was fun for him. He’d see his older brother and sister go in and he’d want to, too. [child’s first dental visit at age 2 years]
Proactive: Avoidance of Problems
A similar proactive parent reason for initiating children’s visits to a dentist was desire to avoid dental problems. The problems parents sought to avoid included: cavities, problems previously experienced by the parents themselves or older siblings (such as pain or abscess), or “silver teeth.” As this caregiver explains:
<interviewer> How did you decide that it was time to take him to the dentist?
<respondent> Well, mainly because I thought that we should take care of his teeth. There are small children that have those silver things [on their teeth]. You see small children who already have that. If I just leave him and don’t take him to the dentist or anything, then maybe he would need that too, all that silver stuff. That’s bad.
[child’s first dental visit at age 3 years]
External Prompts
Pediatrician
The most frequently given external reason prompting a mother to take her child for a first dental visit was pediatrician [physician] recommendation. These caregivers explain:
<interviewer> How did you know it was time to take her [to the dentist]?
<respondent> Because the pediatrician would tell me to when I’d take her there for her checkups. They said it was time to take her to the dentist, to check her teeth to see if they were OK. I started when she was 2 years old. I’d take her every 6 months. They’d clean her teeth and check them. I’ve been taking her every 6 months since she was 2 years old.
[child’s first dental visit at age 2 years]
School
The next most frequent external source prompting a visit was school requirement, as described by this caregiver:
<interviewer> How did you decide that it was time to go to the dentist?
<respondent> Because the school asks you to. You have to bring in a paper that says that they have been to the dentist. That’s why we took him to the dentist.
[child’s first dental visit at age 4 years]
Other
Other examples of external prompts were recommendations from a variety of social or welfare service providers (including federally funded Women Infant and Children [WIC] nutrition sites, continuation school, and community centers) and from family members (such as mothers and sisters.). Collectively, these other external prompt accounted for only 10% of initial dental visits by children.
AGE OF FIRST DENTAL VISIT
As Figure 1 illustrates, the most frequent mother-reported age for the child’s first dental visit was 3 years (range= 0.7–10). Except for school requirement, every other prompt motivating a mother to initiate a child’s first dental visit resulted in the same outcome – on average, a first dental visit around 2.5 years of age,. When compared to all other reasons, the reported age of first dental visit for children with “school requirement” as the parental motivation was different, much later (around 4years vs. 2.5 years).
Figure 1.
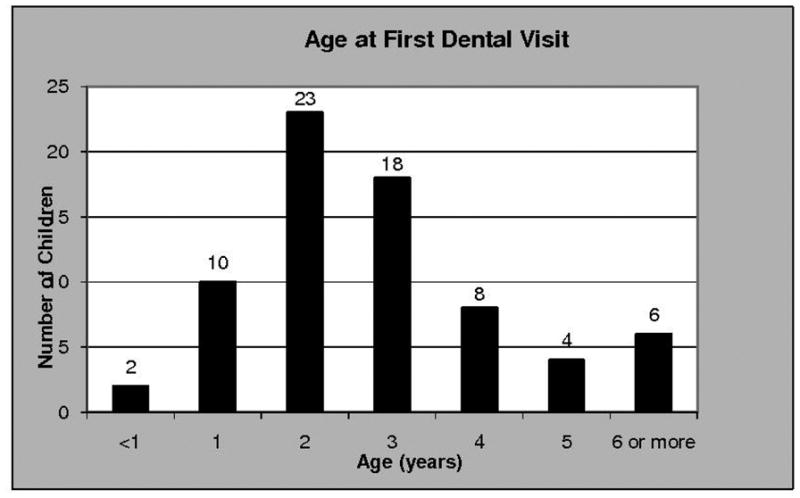
First dental visit by age (n=71 children).
Mother’s education, mother’s age, family income, years in the U.S., child age, country of birth, and birth order appeared to have little or no influence on age at first dental visit. Children born in Mexico and children of older mothers appeared more likely to have first dental visits at a later age than children of U.S.-born or younger mothers.
BARRIERS TO EARLY ACCESS
Some mothers reported difficulty accessing dental care for children. Three parents talked about frustrations when encountering dentists that would not accept their children as dental patients because they were too young. All 3 of these cases were children with significant dental problems. These parents noticed visible problems with their children’s teeth (spots and crumbling) and attempted to take them to dentists when the children were only 2 years old. The caregivers were told their child was too young and to return when their child was 3.
<interviewer> Do you remember the first time you took her to the dentist?
<respondent> The first time I took her to the dent-- well, the dentist said you can’t take them until they’re 3. Because I took her once when her teeth were bad, you could tell they had cavities on them and they [the dentist] said they couldn’t do anything until she turns 3 to put the caps on her because she’s still young. So I took her back when she turned 3 and they put caps on her, on the ones [teeth] that she still had left.
<interviewer> How could you tell she had cavities? What did they look like?
<respondent> Because they’re [the teeth are] yellow and brown and your teeth do not have spots. Not that color spots.
While two parents returned after their child was 3, resulting in extensive restorations, one parent persistently visited many dentists until she found one who would see her 2-year-old:
<respondent> When I took him there [dental clinic]... I had taken him to many places before taking him there, and nobody wanted to see him, because he was a small boy. They didn’t want to see him anywhere. When he had that problem with his teeth, I took him to a dentist, I took him to many dentists, and none of them—they only checked him and said that there was nothing they could do. I called [insurance provider] and [insurance provider] told me about that clinic [that would see him]. Now I’ve changed to that clinic...
DISCUSSION
Results from this study are similar to findings reported in the literature on the general population: few children access dental care under 24 months of age.7,9–12 Half of parents took children to their first dental visit of their own accord, often prompted by visible dental problems, child’s complaint of pain, the caregiver’s concern it is time for a checkup, or to avoid future dental problems. The other half of parents was motivated by pediatricians [physicians], school requirements, or other people. In this study, these low-income, Mexican-origin parents are taking their children to the dentist around 3 years of age, which is around 2 years later than the recommended age of 1 year for high-risk children. Results support the benefits of early first dental visits, with 94% of the sample reporting subsequent regular dental visits or establishment of a “dental home” after the first visit.
Findings from this study provide a valuable contribution to a currently sparse area of the literature. One of this study’s primary strengths is that it is one of the first to describe motivation for first dental visits in a high-risk, low-income, Mexican-American population. While epidemiological surveys can tell us the proportion of children at specific ages who have seen a dentist, this style of research has not examined when the first dental visit was undertaken, nor can it examine what influences that visit. Very little is currently reported on caregivers’ thoughts, beliefs, motivations and behaviors surrounding first dental visits. This research provides some key information about those thoughts, beliefs and motivation and lays a foundation for further research examining these important psycho-social and behavioral components. However, the limitations of this study must be kept in mind when interpreting results. This is not a representative sample. A limitation of particular concern is recall bias because mothers were recalling age at first dental visit, sometimes three or four years after the fact. There is also an issue that multiple children from a single family were included in child data analysis, as there may be family characteristics influencing the data. In this primarily qualitative study, however, inclusion of data from all siblings in a family revealed important information not otherwise discernable: older children’s dental experiences influenced mothers to begin seeking professional oral health care at an earlier age for the younger children in the family. Caution must be used in generalizing findings to a larger population, though in some instances the findings from this study suggest a focus for future studies using larger representative samples. Caution must also be exercised in generalizing results to other Latino populations such as those from a different socioeconomic class, immigrant status, or geographic location. Other limitations of this study include single location, self-report data, and social desirability bias. The distribution and proportion of parental motivations for first dental visit cannot be generalized beyond the study sample, but this study has contributed knowledge about what those motivations are and how they come about, providing a key first step for future studies with larger representative samples.
We found pediatricians to be important sources prompting a child’s first dental visit, resulting in a visit on average around 2.5 years of age. This is similar to other reports noting that despite the current recommendations,5,6 only 5% of physicians are referring children under 1 year old to dentists, and most pediatricians are not referring children for dental visits until an average age of 2.5 years.9,12,27 Because more young children visit a medical provider (85%) than a dental provider (20%), pediatricians can – and do – play a key role in influencing timing of the first dental visit through oral health screenings and dental referrals.28–30 However, only half of practicing physicians that see young children are trained in oral health screening or early childhood caries (ECC) and only 10% know about ECC prevention therapies.12,31 There is ample research to show that physicians with proper training can accurately identify children with and without caries.29,32
Pediatricians have been reported elsewhere to refer children to dental services,9,12,27 and oral health is one of the American Academy of Pediatrics’ (AAP) top 3 priorities and was the focus of the 2008 Peds21 Summit.33 The timing of first dental visit reported in our sample, however, is later than the recommended age. In May 2003, the AAP updated their oral health policy to include risk assessment by 6 months, with high-risk children getting a dentist referral within 6 months of eruption of first tooth or by 1 year of age. The AAP identifies factors that place a child at high–risk for caries including low-income, high sugar diet, poor oral hygiene, having older siblings with caries experience, and parents with poor oral health.34,35 All the children in this study are low-income, a third of them have older siblings with caries, and 60% of caregivers reported themselves to have untreated dental problems. As a high-risk population, they should have been referred to dental treatment much earlier.
There is a possibility that pediatricians referred children at the recommended age and there was a delay between the time of referral and the time when parents actually achieved a first dental visit,31 a topic warranting further research. However, if pediatricians are going to be successful gatekeepers to getting high-risk children to their first dental visit, children need to be screened and referred earlier to allow for this delay.
Pediatricians cannot control the dental environment to which they are referring these children and many pediatricians report difficulty referring children.31 There is a large literature on barriers to access to dental care, including dentists not accepting young children, particularly those on public insurance.31,36–39 There is some debate about whether the dental workforce is trained, equipped, and willing to see and treat such young children, particularly those with severe need, such as many of those with public insurance.7,36–42 Only 36% or fewer dentists agree with the ADA’s recommended age 1 year dental visit.7, 36,42 Smith et al. found that just 3% of dental practices would see publicly insured children under age 1 year for a preventive visit compared to 15% of dental practices who would see publicly insured children over age 5 years for a preventive visit.36 These dentist characteristics do affect access to care and may be a distinctive influence in determining the proportion of children achieving the ADA and AAPD recommended age 1 dental visit. Three parents in our study mentioned dentists discouraging early dental visits. These particular cases involved children with severe ECC that most likely was exacerbated between the parents’ attempts at a first visit, and actually achieving a visit at age 3. This underscores the need for more dentists to treat young children and more dental schools to adequately train dentists to be able to do so.7,36,42 Additionally, there is a need for community organizations to continue to help caregivers overcome barriers to access to care.30,43
Schools also serve as an important prompt to initiate dental care, triggering caregivers who have either not received or not followed suggestions from other sources. Rules at both the preschool and elementary school level44 were important in getting children into the dentist for the first time. In California, legislation passed in 2006 requires a dental visit before the end of the child’s first year in school, whether that be kindergarten or first grade.44 Head Start has requirements that encourage children to visit a dentist and establish a dental home, and parents feel the program helps support them in overcoming access barriers.38,42 However, school age is too late for first dental visits for a high-risk population, such as low-income Mexican-American children (many with older siblings and parents with caries experience or untreated dental problems). Schools should not be relied upon as a primary prompt for first dental visits, but do serve an important function in reinforcing the need for children to receive dental care.
It is important to increase and tailor education for parents, pediatricians, and other service providers to encourage and facilitate the first dental visit by age 1 for this population. At the same time, the dental workforce needs to be better equipped to handle an increase in young patients. For this at-risk population, increasing preventive treatment at a young age may help decrease their later caries experience and cost of care as well as increase their quality of life.
CONCLUSIONS
Parents’ internal motivations for taking their children to a first dental visit are either reactive or proactive. Reactive visit initiation came after discovery of a visible tooth problem or a child’s complaint of pain. Proactive visit initiation resulted from parents’ desire to avoid dental problems or desire for a checkup.
Parents’ external motivation for taking children to the first dental visit stemmed mainly from pediatrician recommendation. School requirement, and other sources (eg, family members) were less prominent external prompts.
Children in the study, as in many previous studies in the literature, sought first dental visits around age 3 years, much later than the recommended 1 year. Children of parents’ that sought a dental visit for their children due to school requirement had particularly late first visits.
Acknowledgments
Support was provided by the National Institute of Dental and Craniofacial Research grant number NIH/NIDCR U54 DE 014251, (Center to Address Disparities in Children’s Oral Health, Jane A. Weintraub, DDS, MPH, Principal Investigator). We thank Dr. Susan A. Fisher-Owens, MD, MPH for her assistance in reviewing the manuscript. We especially thank all of the women and community members who participated in the project.
References
- 1.Ramos-Gomez FJ, Crall J, Gansky SA, Slayton RL, Featherstone JD. Caries risk assessment appropriate for the age 1 visit (infants and toddlers) J Calif Dent Assoc. 2007;35:687–702. [PubMed] [Google Scholar]
- 2.Nainar SM. Longitudinal analysis of dental services provided to urban low-income (Medicaid) preschool children seeking initial dental care. ASDC J Dent Child. 1998;65:339–43. 355–6. [PubMed] [Google Scholar]
- 3.Savage MF, Lee JY, Kotch JB, Vann WF., Jr Early preventive dental visits: effects on subsequent utilization and costs. Pediatrics. 2004;114:e418–23. doi: 10.1542/peds.2003-0469-F. [DOI] [PubMed] [Google Scholar]
- 4.Riley JL, 3rd, Gilbert GH. Childhood dental history and adult dental attitudes and beliefs. Int Dent J. 2005;55:142–50. doi: 10.1111/j.1875-595x.2005.tb00311.x. [DOI] [PubMed] [Google Scholar]
- 5.Baby’s First Teeth. American Dental Association; 2002. [Accessed July 22, 2008]. Available at: http://www.ada.org/prof/resources/pubs/jada/patient/patient_11.pdf. [Google Scholar]
- 6.Guideline on Infant Oral Health Care. American Academy of Pediatric Dentistry; 2004. [Accessed July 15, 2008]. Available at: http://aapd.org/media/Policies_Guidelines/G_InfantOralHealthCare.pdf. [Google Scholar]
- 7.Wolfe JD, Weber-Gasparoni K, Kanellis MJ, Qian F. Survey of Iowa general dentists regarding the age 1 dental visit. Pediatr Dent. 2006;28:325–31. [PubMed] [Google Scholar]
- 8.Sohn W, Ismail A, Amaya A, Lepkowski J. Determinants of dental care visits among low-income African-American children. J Am Dent Assoc. 2007;138:309–18. doi: 10.14219/jada.archive.2007.0163. quiz 395–6, 398. [DOI] [PubMed] [Google Scholar]
- 9.Brickhouse TH, Unkel JH, Kancitis I, Best AM, Davis RD. Infant oral health care: a survey of general dentists, pediatric dentists, and pediatricians in Virginia. Pediatr Dent. 2008;30:147–53. [PubMed] [Google Scholar]
- 10.Kramer PF, Ardenghi TM, Ferreira S, Fischer Lde A, Cardoso L, Feldens CA. Use of dental services by preschool children in Canela, Rio Grande do Sul State, Brazil. Cad Saude Publica Jan. 2008;24:150–6. doi: 10.1590/s0102-311x2008000100015. [DOI] [PubMed] [Google Scholar]
- 11.Schroth RJ, Brothwell DJ, Moffatt ME. Caregiver knowledge and attitudes of preschool oral health and early childhood caries (ECC) Int J Circumpolar Health. 2007;66:153–67. doi: 10.3402/ijch.v66i2.18247. [DOI] [PubMed] [Google Scholar]
- 12.Ismail AI, Nainar SM, Sohn W. Children’s first dental visit: attitudes and practices of US pediatricians and family physicians. Pediatr Dent. 2003;25:425–30. [PubMed] [Google Scholar]
- 13.Slayton RL, Warren JJ, Levy SM, Kanellis MJ, Islam M. Frequency of reported dental visits and professional fluoride applications in a cohort of children followed from birth to age 3 years. Pediatr Dent. 2002;24:64–8. [PubMed] [Google Scholar]
- 14.Al-Shalan TA, Al-Musa BA, Al-Khamis AM. Parents’ attitude towards children’s first dental visit in the College of Dentistry, Riyadh, Saudi Arabia. Saudi Med J. 2002;23:1110–4. [PubMed] [Google Scholar]
- 15.Al-Shalan TA. Factors affecting Saudi parents’ perception of their children’s first dental visit. J Contemp Dent Pract. 2003;4:54–66. [PubMed] [Google Scholar]
- 16.United States. Dept. of Health and Human Services. National Institute of Dental and Craniofacial Research (U.S.) Oral health in America: a report of the Surgeon General. Rockville, Md: U.S. Public Health Service Dept. of Health and Human Services; 2000. [Google Scholar]
- 17.Nurko C, Aponte-Merced L, Bradley EL, Fox L. Dental caries prevalence and dental health care of Mexican-American workers’ children. ASDC J Dent Child. 1998;65:65–72. [PubMed] [Google Scholar]
- 18.Douglass JM, Tinanoff N, Tang JM, Altman DS. Dental caries patterns and oral health behaviors in Arizona infants and toddlers. Community Dent Oral Epidemiol. 2001;29:14–22. [PubMed] [Google Scholar]
- 19.Watson MR, Horowitz AM, Garcia I, Canto MT. Caries conditions among 2–5-year-old immigrant Latino children related to parents’ oral health knowledge, opinions and practices. Community Dent Oral Epidemiol. 1999;27:8–15. doi: 10.1111/j.1600-0528.1999.tb01986.x. [DOI] [PubMed] [Google Scholar]
- 20.Hilton IV, Stephen S, Barker JC, Weintraub JA. Cultural factors and children’s oral health care: a qualitative study of carers of young children. Community Dent Oral Epidemiol. 2007;35:429–38. doi: 10.1111/j.1600-0528.2006.00356.x. [DOI] [PubMed] [Google Scholar]
- 21.Horton S, Barker JC. Rural Latino immigrant caregivers’ conceptions of their children’s oral disease. J Public Health Dent. 2008;68:22–9. doi: 10.1111/j.1752-7325.2007.00078.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Foster . Children’s Dental Health in Santa Clara and San Mateo Counties: Overview of Current Needs and Activities. Lucille Packard Foundation; 2006. [Google Scholar]
- 23.Drum MA, Chen DW, Duffy RE. Filling the gap: equity and access to oral health services for minorities and the underserved. Fam Med. 1998;30:206–9. [PubMed] [Google Scholar]
- 24.Burger Peter, Luckman Thomas. The Social Construction of Reality: A Treatise in the Sociology of Knowledge. Garden City, NY: Doubleday; 1966. [Google Scholar]
- 25.Bernard HR. Research methods in anthropology: qualitative and quantitative approaches. 4. Lanham, MD: AltaMira Press; 2005. [Google Scholar]
- 26.Miles MB, Huberman AM. Qualitative data analysis: an expanded sourcebook. 2. Thousand Oaks: Sage Publications; 1994. [Google Scholar]
- 27.Pierce KM, Rozier RG, Vann WF., Jr Accuracy of pediatric primary care providers’ screening and referral for early childhood caries. Pediatrics. 2002;109:E82. doi: 10.1542/peds.109.5.e82. [DOI] [PubMed] [Google Scholar]
- 28.McCormick MC, Kass B, Elixhauser A, Thompson J, Simpson L. Annual report on access to and utilization of health care for children and youth in the United States--1999. Pediatrics. 2000;105(1 Pt 3):219–30. [PubMed] [Google Scholar]
- 29.Gussy MG, Waters EG, Walsh O, Kilpatrick NM. Early childhood caries: current evidence for aetiology and prevention. J Paediatr Child Health. 2006;42:37–43. doi: 10.1111/j.1440-1754.2006.00777.x. [DOI] [PubMed] [Google Scholar]
- 30.Goldfeld SR, Wright M, Oberklaid F. Parents, infants and health care: utilization of health services in the first 12 months of life. J Paediatr Child Health. 2003;39:249–53. doi: 10.1046/j.1440-1754.2003.00146.x. [DOI] [PubMed] [Google Scholar]
- 31.Lewis CW, Grossman DC, Domoto PK, Deyo RA. The role of the pediatrician in the oral health of children: A national survey. Pediatrics. 2000;106:E84. doi: 10.1542/peds.106.6.e84. [DOI] [PubMed] [Google Scholar]
- 32.Jones CM, Tinanoff N, Edelstein BL, et al. Creating partnerships for improving oral health of low-income children. J Public Health Dent. 2000;60:193–6. doi: 10.1111/j.1752-7325.2000.tb03327.x. [DOI] [PubMed] [Google Scholar]
- 33. [Accessed March 9, 2009];National Summit on Children’s Oral Health. Available at: http://www.aap.org/oralhealth/summit.cfm.
- 34.Hale KJ. Oral health risk assessment timing and establishment of the dental home. Pediatrics. 2003;111(5 Pt 1):1113–1116. doi: 10.1542/peds.111.5.1113. [DOI] [PubMed] [Google Scholar]
- 35.Oral Health Risk Assessment Timing and Establishment of the Dental Home. American Academy of Pediatrics; [Accessed July 9, 2008]. Available at: http://www.aap.org/healthtopics/oralhealth.cfm. [DOI] [PubMed] [Google Scholar]
- 36.Smith RG, Lewis CW. Availability of dental appointments for young children in King County, Washington: implications for access to care. Pediatr Dent. 2005;27:207–11. [PubMed] [Google Scholar]
- 37.Seale NS, Casamassimo PS. Access to dental care for children in the United States: a survey of general practitioners. J Am Dent Assoc. 2003;134:1630–40. doi: 10.14219/jada.archive.2003.0110. [DOI] [PubMed] [Google Scholar]
- 38.Siegal MD, Marx ML, Cole SL. Parent or caregiver, staff, and dentist perspectives on access to dental care issues for Head Start children in Ohio. Am J Public Health. 2005;95:1352–9. doi: 10.2105/AJPH.2004.054858. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Kelly SE, Binkley CJ, Neace WP, Gale BS. Barriers to care-seeking for children’s oral health among low-income caregivers. Am J Public Health. 2005;95:1345–51. doi: 10.2105/AJPH.2004.045286. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Jones K, Tomar SL. Estimated impact of competing policy recommendations for age of first dental visit. Pediatrics. 2005;115:906–14. doi: 10.1542/peds.2004-1687. [DOI] [PubMed] [Google Scholar]
- 41.McWhorter AG, Seale NS, King SA. Infant oral health education in U.S. dental school curricula. Pediatr Dent. 2001;23:407–9. [PubMed] [Google Scholar]
- 42.Siegal MD, Marx ML. Ohio dental care providers’ treatment of young children, 2002. J Am Dent Assoc. 2005;136:1583–91. doi: 10.14219/jada.archive.2005.0093. [DOI] [PubMed] [Google Scholar]
- 43.Kanellis MJ. Caries risk assessment and prevention: strategies for Head Start, Early Head Start, and WIC. J Public Health Dent. 2000;60:210–7. doi: 10.1111/j.1752-7325.2000.tb03330.x. discussion 218–20. [DOI] [PubMed] [Google Scholar]
- 44.Kindergarten Oral Health Requirement (AB 1433) California Dental Association; [Accessed August 19, 2008]. Available at: http://www.cda.org/advocacy_&_the_law/legislation/kindergarten_oral_health_requirement. [Google Scholar]