

Abstract
Purpose/Background:
Researchers have observed differences in muscle activity patterns between males and females during functional exercises. The research methods employed have used various step heights and lunge distances to assess functional exercise making gender comparisons difficult. The purpose of this study was to examine core and lower extremity muscle activity between genders during single‐limb exercises using adjusted distances and step heights based on a percentage of the participant's height.
Methods:
Twenty men and 20 women who were recreationally active and healthy participated in the study. Two‐dimensional video and surface electromyography (SEMG) were used to assess performance during three exercise maneuvers (step down, forward lunge, and side‐step lunge). Eight muscles were assessed using SEMG (rectus abdominus, external oblique, erector spinae, rectus femoris, tensor fascia latae, gluteus medius, gluteus maximus, biceps femoris). Maximal voluntary isometric contractions (MVIC) were used for each muscle and expressed as %MVIC to normalize SEMG to account for body mass differences. Exercises were randomized and distances were normalized to the participant's lower limb length. Descriptive statistics, mixed‐model ANOVA, and ICCs with 95% confidence intervals were calculated.
Results:
Males were taller, heavier, and had longer leg length when compared to the females. No differences in %MVIC activity were found between genders by task across the eight muscles. For both males and females, the step down task resulted in higher %MVIC for gluteus maximus compared to lunge, (p=0.002). Step down exercise produced higher %MVIC for gluteus medius than lunge (p=0.002) and side step (p=0.006). ICC3,3 ranged from moderate to high (0.74 to 0.97) for the three tasks.
Conclusions:
Muscle activation among the eight muscles was similar between females and males during the lunge, side‐step, and step down tasks, with distances adjusted to leg length. Both males and females elicited higher muscle activity for gluteus maximus and gluteus medius as compared to the trunk, hip flexors, or hamstring muscles. However these values were well below the recruitment levels necessary for strengthening in both genders.
Level of evidence:
4
Keywords: electromyography, functional exercises, gender, gluteus medius, gluteus maximus
INTRODUCTION
Functional weight bearing tasks are commonly prescribed as therapeutic exercise to strengthen the lower extremity and simulate activities of daily living. The hip and knee are important to address ‐during rehabilitation because weakness in these anatomical regions have been associated with injuries.1‐4 Specifically, an increase in patellofemoral syndrome and non‐contact anterior cruciate ligament injuries have been found in individuals who have weak hip abductors1,4‐7 or delayed activity in portions of the quadriceps muscle.8
In an effort to determine muscle activity or joint motions during weight‐bearing exercises, numerous kinematic or surface electromyography (SEMG) studies have been performed using the lunge,7‐13 single limb squat,13‐16 or step tasks.5,7‐11,14,15,17‐21 The single limb squat exercise has been reported to be effective in activating gluteus medius ranging from 30% reference voluntary contraction (RVC)15 to 60% maximum isometric voluntary contraction (MVIC).16 The SEMG values during the lunge task for the gluteus maximus have ranged from 14%MVIC to 44%MVIC and gluteus medius activity has varied from 15%MVIC to 42%MVIC.9‐11 The wide range of SEMG values for these tasks may be explained due to differences in subject pool, whether the concentric and eccentric phases of exercise were assessed, if SEMG normalization was performed, and how the tasks were performed.
The large variation of SEMG data during LE functional exercise tasks may also be the result of how men and women differ in controlling the lower extremity during exercise or sport activities. Currently, it is unclear as to whether gender differences exist during performance of functional tasks because of the conflicting data. Many studies support the theory that females have an increased reliance on quadriceps or rectus femoris activity during maneuvers that simulate soccer play,22,23 lunges,11,12 and single‐legged squat.11,16,24 In contrast, Beutler et al25 reported greater knee flexion angles during step‐up and squat exercises among men; however quadriceps activity was similar between males and females. Likewise, Cowen and Crossley18 found no gender differences in quadriceps and gluteus medius muscle activity during a stepping task. The inconsistency within the literature may be due to the lack of task standardization among studies. For example, Dwyer et al11 standardized the lunge distance based on leg length but did not normalize the step up and over task. Others have also used the same box heights for males and females despite differences in their actual heights.25‐27
Overall gender differences that occur during athletic maneuvers such as running and cutting,22,23,28‐31 landing,24,27,32,33 jumping,34 and hopping35 have been well documented, yet there are few studies comparing gender performance during common functional tasks.11,16,18 The abundance of evidence associated with gender differences during dynamic running and cutting tasks is, in part, due to researchers attempting to better understand the mechanism linked to athletic‐related injuries such as those that occur in the anterior cruciate ligament. Although single‐limb weight‐bearing exercises do not simulate the same dynamic motions as game‐like tasks, assessment of muscle performance during functional tasks may be important for injury prevention and optimal rehabilitation Therefore, the purpose of this study was to examine core and lower extremity muscle activity between genders during single‐limb exercises using adjusted distances and step heights based on a percentage of the participant's height. It was hypothesized that there would be no significant differences between genders for the %MVIC of the selected trunk, hip, and thigh muscles during the three functional tasks.
METHODS
Subjects
Forty recreationally active subjects, 20 males (mean age = 23.2 ± 1.9 yrs, height= 1.8 ± .09 cm, bodyweight = 87.8 ± 20.0 kg) and 20 females (mean age = 22.4 ± 1.8 yrs, height= 1.6 ± .07 cm, bodyweight= 42.5 ± 7.0 kg) with no known musculoskeletal injuries participated in the study. Recreationally active was defined as someone who participated in recreational activities three to five times a week for at least 30 minutes per day. Subjects were recruited by flyers distributed throughout the university and surrounding community. The exclusion criteria consisted of anyone diagnosed with musculoskeletal, cardiovascular, vestibular, visual, or balance disorders and a history of back injury, back pain or back deformity requiring medical treatment. The university IRB approved the study protocol and written informed consent was obtained from all individuals prior to participation.
Instrumentation
Muscle activity data was collected using an 8‐channel surface telemetry EMG system (Noraxon Myosystem 900 EMG system, Noraxon USA, Inc., Scottsdale, AZ) and a 2‐D video recording was obtained during performance of the test movements in order to assist in subsequent analysis. The digital video camera (Canon Optura50, Canon Inc., Lake Success, NY) was placed at the height of the subject's knee, three meters anterior to the subject for a frontal plane recording for the step down and side‐step tasks and sagittal plane recording for lunge. A transmitter belt unit powered by a 9V battery was worn to collect surface electromyography (SEMG) signals. Raw SEMG data were sampled at 1000Hz for each of the eight muscles on the dominant limb. The unit was set with a differential input impedance of greater than 10 MΩ, a gain of 1000, and a common‐mode rejection ratio of 115 dB.
Procedures
Silver‐silver chloride snap single surface pregelled electrodes (Noraxon USA, Inc., Scottsdale, AZ) were placed in a bipolar configuration on the skin of the dominant leg and torso of same side of dominant limb. The dominant leg was defined the preferred kicking leg.10,14 The electrodes were positioned parallel to the muscle fiber orientation with an interelectrode distance of approximately 2.0 cm. The skin was prepped by shaving, abrading, and cleaning with isopropyl alcohol wipes prior to electrode placement. The ground lead was placed on the subject's anterior superior iliac spine (ASIS) contralateral to the subject's dominant leg. Each subsequent lead was positioned as defined by Cram36 and Rainoldi et al37 on the subject's dominant side. The rectus femoris (RF) electrodes were placed midway between the ASIS and base of the patella. Electrodes for the upper fibers of the rectus abdominus (RA) were placed at the midpoint between the umbilicus and xyphoid process, and three cm lateral with the electrode aligned longitudinally in parallel with the fibers of the muscle. Electrode placement for external oblique (EO) was at the level of the umbilicus at an oblique angle (45 degrees) between the inferior costal margin and ASIS. The electrodes for the tensor fascia latae (TFL) were placed two fingerbreadths distal to the ASIS and two fingerbreadths medial to the greater trochanter. Electrodes for the anterior gluteus medius (GMed) were approximately three cm inferior to the iliac crest.38 Electrodes for the erector spinae (ES) were placed in a vertical direction two centimeters lateral to the spinous processes between L3‐L4. Electrodes for the lower fibers of the gluteus maximus (GMax) were placed inferior and medial to a line drawn between the PSIS and the posterior greater trochanter. The electrodes for biceps femoris (BF) were placed midway between the ischial tuberosity and the crease of the patella fossa.
Following rest period, subjects performed a brief warm up of lower extremity flexibility exercises. After the warm‐up, the experimental protocol was described using verbal instructions and demonstration of each exercise. Subjects were given the opportunity to practice the forward lunge, side‐step lunge, step down exercises for ten repetitions. Participants completed each of the three unilateral functional exercises (step down, forward lunge, and side‐step lunge) in a randomized order. For each activity, the subjects performed two sets of 10 repetitions at a pace of 80 bpm using a metronome. This rate was equal to 20 steps/lunges per minute (four clicks for each repetition). Each step or lunge repetition was three seconds in duration. The initial set was used as a practice trial and second set was used for data analysis. Following each practice session, the subjects were given a 30‐second rest break.
Step down.
Subjects were asked to step down from a height adjusted to 25% (±5%) of their leg length based on previous research.39 The step height was determined by measuring limb length on the dominant limb with the subject in a supine position on a mat table. A tape measure was placed on the most inferior aspect of the anterior superior iliac spine and most distal portion of the medial malleolus. A single measurement of the total leg length was recorded in millimeters, and multiplied by 25% to determine step height for each subject. The subject stood on the step with hands on hips and feet shoulder width apart. The dominant leg served as the stance leg and opposite limb moved in an anterior direction toward the ground, until the heel of the non‐dominant foot contacted the ground, and then returned to initial position (Figure 1).
Figure 1.
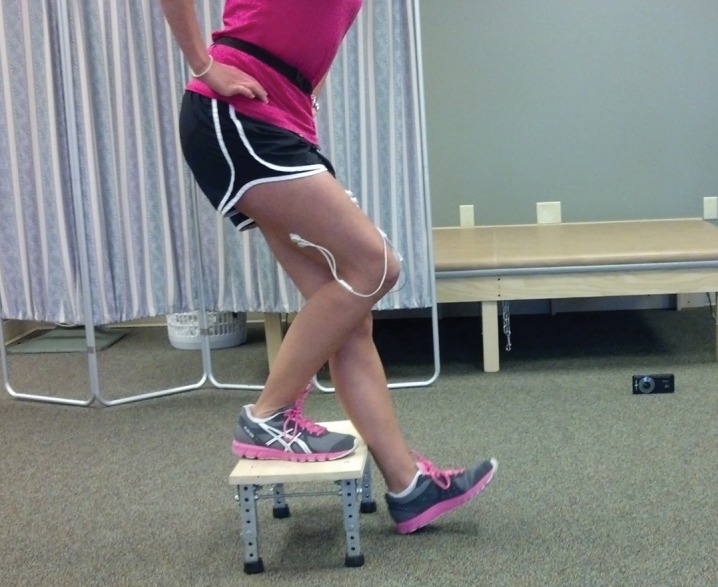
Test position for step down task.
Forward lunge.
Subjects were instructed to stand with their feet shoulder width apart. The distance that the subjects stepped forward during the lunge was adjusted to 65% (±5%) of their leg length. This distance was chosen based on pilot testing in which the final position could be performed comfortably with the dominant limb held vertically while maintaining the knee over the foot. The total leg length recorded in millimeters was multiplied by 65% to determine forward lunge distance for each subject. A tape measure was placed on the floor and the subject was asked to perform the forward lunge with their dominant leg so that the midpoint of the heel reached the adjusted distance. Participants were also instructed to make full foot‐flat while maintaining hip and knee flexion to 90 degrees and avoiding ground contact with the non‐dominant knee. The subjects were asked to return to starting position with full knee extension of the lunge leg (Figure 2).
Figure 2.

Test position for forward lunge task.
Side‐step lunge.
Subjects were instructed to stand with their feet shoulder width apart. The distance that the subjects stepped sideways during the lunge was adjusted to 80% (±5%) of their leg length. This distance was chosen based on pilot testing in which the final position could be performed with the non‐dominant limb held in full knee extension comfortably while the dominant limb maintain the knee over the foot. The total leg length recorded in millimeters was multiplied by 80% to determine side‐step lunge distance for each subject. The non‐dominant leg remained in full knee extension throughout the activity. A tape measure was placed on the floor and the subject was asked to perform a side‐step with their dominant leg so that the midpoint of the heel reached the adjusted distance (Figure 3). The repetition was completed when the subject returned to the initial position.
Figure 3.

Test position for side‐step lunge task.
Electromyography Analysis
Three maximal voluntary isometric contractions (MVIC) were performed in standard manual muscle test positions40 for each subject for the eight muscles analyzed. Following MVIC data collection, participants rested for five minutes prior to the functional exercise testing. Each test for MVIC was held for five seconds, was followed by three second rests between contractions, and was performed three times. There was a 30‐second rest between muscles tested. The rectus femoris was tested with the subject sitting with knees over the table, and manual resistance applied approximately 40 degrees from full knee extension.40 The rectus abdominis muscle was tested with trunk moving in a flexed position as a partial curl‐up, and resistance applied to bilateral shoulders.41 The external oblique abdominal was tested with the subject in a hook lying position with the trunk directed toward the opposite knee.40 The tensor fascia latae was tested in a supine position, the hip placed in an abducted, flexed, and medial rotated position with the knee extended. Manual resistance was applied at the distal lower leg as the limb moved into extension and adduction.40 The gluteus medius was assessed in a sidelying position, with the hip in neutral rotation and slightly extended with manual resistance applied at the distal lower leg as the hip actively moved into abduction. The subject was positioned in prone for gluteus maximus, with the knee flexed to 90 degrees and the hip fully extended. Manual resistance was applied on the lower part of the posterior thigh as the hip moved into extension. The erector spinae was tested with the subject in prone and trunk off the edge of the table at the level of the ASIS. A second investigator stabilized the lower extremity just above the ankle as the subject extended the lumbar spine to neutral and resistance applied to the posterior scapula.41 The biceps femoris was tested in prone position with knee flexed to 45 degrees and lower leg in external rotation.41 The average SEMG amplitudes collected during the functional exercises were later normalized to the highest MIVC value obtained during manual muscle tests, and expressed as percentage of MIVC (%MIVC).
The receiver converted the signal from analog to digital through an external USB A/D converter, and signals were displayed on a computer monitor. The amplifier bandwidth frequency ranged from 10Hz highpass to 500 Hz lowpass. The SEMG signals were directed through a 12‐bit analog‐digital converter (Telemyo, Norazon USA, Inc, Scottsdale, AZ). The raw data was stored in a personal computer and Myoresearch 2.10 software (Noraxon USA, Inc, Scottsdale, AZ) was used to process and analyze the data. The raw SEMG signals were obtained during the 4th through 6th repetitions. Each repetition lasted three seconds which captured the start of the movement and return to original position. The onset of each of the eight muscle contractions during the three tasks were marked by the start of motion as noted on the video recording when the muscle SEMG amplitude was 10 μV of baseline. The raw SEMG signals were processed using a full‐wave rectification and a root‐mean‐square algorithm at a time constant of 300 milliseconds.
STATISTICAL ANALYSIS
The average peak MVICs generated from each of the eight manual muscle tests were used to normalize the SEMG amplitudes for each muscle and expressed as %MIVC. Descriptive statistics, ANOVAs, and ICCs with 95% confidence intervals were calculated using SPSS version 18.0 (SPSS, Inc, Chicago, IL) software. Descriptive statistics were reported as means ± standard deviations for all subjects. One way ANOVAs were used to if determine differences existed for age, height, and body mass index (BMI). Repetitions 4‐6 of each exercise were converted to a mean amplitude for the eight muscles, and the overall mean was used for SEMG was used for analysis. Shapiro‐Wilk's W‐test was applied to examine normality in the distribution of data. The normalized SEMG values were analyzed using 8 separate 2 × 3 ANOVAs (normalized SEMG values for 8 muscles), gender (male and female) and task (lunge, side‐step, step‐down). Post‐hoc comparisons of the means of interest were conducted using the Bonferroni procedure.
The intraclass correlation coefficients (ICC3,3) and 95% confidence intervals (CIs) were calculated across the middle three repetitions (4‐6 repetitions) for each muscle and exercise to confirm consistency of SEMG values. The strength of the correlations were classified as: 0‐.25 “little,” .26‐.49 “low,” .50‐.69 “moderate,” .70‐.89 “high,” and .9‐1.0 “very high.”42 Standard error of the mean (SEM) was calculated by multiplying the standard deviation of the %MVIC for each muscle by the square root of 1 minus the ICC(3,3) to describe the precision of the measurement.42 The significance level was set a priori at p<0.02, (.05/3).
RESULTS
Leg length, height and weight were significantly greater for males as compared to females (Table 1). The men had 0.07 m longer leg length as compared to women. The males were also 0.2 meters taller and weighed 20 kilograms more as compared to females.
Table 1.
Participant Characteristics
| Age (y) | Height (m) | Leg Length (m) | Weight (kg) | BMI(kg/m2) | |
|---|---|---|---|---|---|
| Males | 23±2 | 1.8±.09* | .94±.05* | 85±20* | 26±5 |
| Females | 22±3 | 1.6±.07 | .87±.05 | 65±7 | 24±2 |
Data expressed as means (± standard deviation)
Indicates males were significantly greater in height, leg length, and body weight than females, p=0.0001.
The ANOVA (gender by task) indicated no significant difference existed among the eight muscles and results are presented in Table 2. A significant effect was found among two of the eight muscles, GMax %MVIC, (p=0.004) and GMed %MVIC, (p=0.002) for both males and females. Post hoc testing indicated that the step down task resulted in higher GMax %MVIC activity compared to lunge, (p=.002). The step down exercise was also higher for GMed %MVIC than lunge (p=.002) and side step (p=.006).
Table 2.
Comparison of means (± standard deviation) for electromyographic activity of eight muscles during the three tasks for males and females.
| Lunge | Side‐Step | Step‐Down | ||||
|---|---|---|---|---|---|---|
| Male | Female | Male | Female | Male | Female | |
| Rectus Femoris | 12±2 | 12±2 | 12±3 | 11±2 | 12±2 | 13±2 |
| Rectus Abdominis | 13±3 | 13±4 | 15±3 | 13±4 | 14±4 | 15±5 |
| External Oblique | 12±3 | 12±4 | 12±5 | 13±4 | 13±5 | 12±5 |
| Erector Spinae | 13±3 | 12±4 | 15±2 | 13±4 | 14±3 | 13±4 |
| Tensor Fascia Latae | 12±3 | 13±2 | 12±3 | 13±3 | 13±2 | 14±2 |
| Biceps Femoris | 12±3 | 13±2 | 12±3 | 12±2 | 13±3 | 14±2 |
| Gluteus Medius | 12±2 | 12±2 | 13±3 | 13±2 | 14±3* | 14±3* |
| Gluteus Maximus | 11±3 | 10±2 | 12±4 | 12±2 | 13±2† | 13±2† |
Data expressed as means (± standard deviation) percentage of maximum voluntary isometric contraction (%MVIC).
For gluteus medius muscle, statistically higher %MVIC for step down compared to lunge (p= 002) and side step (p=.006)
For gluteus maximus muscle, statistically higher %MV1C for step down compared to lunge, (p=002)
The reliability analysis (ICC3,3) across the three repetitions for each exercise activity resulted reliability values for the lunge ranging from 0.74 to 0.97, side‐step (.83 to .99), and step down (.82 to .96) (Tables 3 and 4). These values indicate moderate to high ‐reliability across all muscles among the exercise tasks between males and females.42 The SEM values presented in Tables 3 and 4 ranged from .45%MVIC to 1.15%MVIC across the three exercises.
Table 3.
Mean differences expressed as %MVIC during the three tasks for gluteus medius and gluteus maximus muscles.
| Lunge | Side‐Step | Step‐Down | |
|---|---|---|---|
| Gluteus Medius | |||
| Lunge | / | −.34 | −1.79* |
| Side‐Step | .34 | / | −1.45* |
| Step‐Down | 1.79* | 1.45* | / |
| Gluteus Maximus | |||
| Lunge | / | −.95 | −2.00* |
| Side‐Step | .95 | / | −1.05 |
| Step‐Down | 2.00* | 1.05 | / |
Data expressed as mean difference using Bonferroni test‐ mean difference (I‐J) and significance.
indicates significant difference
Table 4.
Intrarater repeatability and SEM for three exercises and eight muscles among females.
| Lunge | Side‐Step | Step‐Down | ||||
|---|---|---|---|---|---|---|
| ICC3,3 | SEM | ICC3,3 | SEM | ICC3,3 | SEM | |
| Rectus Femoris | .74 | .97 | .91 | .63 | .86 | .70 |
| Rectus Abdominus | .94 | .51 | .95 | .94 | .96 | .98 |
| External Oblique | .90 | 1.15 | .95 | .88 | .96 | .91 |
| Erector Spinae | .94 | .90 | .95 | .84 | .97 | .62 |
| Tensor Fascia Latae | .94 | .45 | .88 | .90 | .84 | .87 |
| Biceps Femoris | .86 | .84 | .87 | .81 | .82 | 1.0 |
| Gluteus Medius | .76 | .82 | .83 | .49 | .94 | .64 |
| Gluteus Maximus | .87 | .84 | .86 | .77 | .85 | .61 |
Table 5.
Intrarater repeatability and SEM for three exercises and eight muscles among males.
| Lunge | Side‐Step | Step‐Down | ||||
|---|---|---|---|---|---|---|
| ICC3,3 | SEM | ICC3,3 | SEM | ICC3,3 | SEM | |
| Rectus Femoris | .92 | .62 | .97 | .52 | .90 | .76 |
| Rectus Abdominus | .91 | .99 | .90 | .99 | .93 | 1.05 |
| External Oblique | .97 | .63 | .93 | .83 | .96 | 1.01 |
| Erector Spinae | .94 | .72 | .88 | .85 | .84 | .73 |
| Tensor Fascia Latae | .91 | .81 | .92 | .83 | .87 | .75 |
| Biceps Femoris | .94 | .77 | .92 | .70 | .93 | .90 |
| Gluteus Medius | .92 | .68 | .91 | .78 | .91 | .78 |
| Gluteus Maximus | .97 | .57 | .99 | .42 | .84 | .83 |
DISCUSSION
The purpose of the current study was to examine lower extremity activation patterns between men and women performing three functional tasks. Each of the tasks performed was unilateral weight bearing, and the excursion distances were adjusted to a percentage of the subject's leg length. The results of the current study support the hypothesis that males and females would elicit similar muscle activity among the tasks when the excursion distances were adjusted to a percentage of the subject's leg length.
The current study indicated no gender differences among the three tasks using the adjusted excursion distances based on a percentage of leg length. The authors felt adjusting the step height or lunge distance based upon the subject's leg length was important because of height differences between the males and females. The female subjects were significantly shorter (1.6 ± .07 m) and had shorter leg length (.87 ± .05 m) compared to the height of the males (1.8 ± .09m) and their leg length, (.94 ± .05 m). In contrast, other authors have reported sex differences in muscle activity or limb positioning, however, chose not to modify the task heights.11,26,27 For example, Dwyer et al did not adjust the step height for their step‐up‐and‐over exercise despite the men being 1.4 m taller compared to females.11 Similarly, Zazulak et al maintained the same box height during testing, even though the females were 1.3 m shorter than the males.26 Others have studied muscle activity requiring men and women to drop land from a 6 m box.27 These authors did not report statistical analysis of subject demographics, however the women were 1.9 m shorter compared to males. It may be that in addition to different intrinsic muscle or joint position strategies, women compensate because of the greater relative step height or jump distances related to their shorter stature.
The authors of the current study selected unilateral weight bearing exercises including the forward and side‐step lunge and step‐down activity for examination. Since stair climbing is a very common task, many studies use a standard step height of 20 cm to 21 cm.6,9,11,15,21 However, step heights of 15 cm14,20 19 cm,17 30.5 cm,26 and 25% of leg length41 have been used in research. The distance covered during a lunge has also varied from a comfortable distance7 to full range of motion,9,11 and to 90 degrees of knee flexion.10 These variations of excursion distances and step heights make it difficult to compare functional tasks across studies.
The authors found that the average SEMG activity ranged among the participants from 10 to 14%MVIC for five lower extremity muscles. Trunk muscle activity, specifically for external oblique, rectus abdominis, and erector spinae muscles ranged between 12 to 15%MVIC. Ekstrom et al9 found that the core muscle SEMG activity for rectus abdominis was 7% and external oblique at 17%MVIC. The percent MVIC differences between this study and others may be the result of possible variations among lunge distances, trunk position, electrode placement, or which portion of the muscle was assessed.
The muscle activity variations may also be related to time differences chosen to process SEMG amplitudes. The current study used a 3‐second time period to collect raw SEMG signals which were then smoothed over 300 ms window. Dwyer et al also collected raw SEMG signals for three seconds, however they smoothed over 500 ms window.11 Others have processed SEMG signals with varying window lengths from 15 ms5, 20 ms10 to 55 ms.20 Cram suggested that the typical SEMG window range from 100 ms to 200 ms.36 Others have proposed that the optimal window length for static and dynamic contractions should range from 200 ms to 300 ms, respectively.43 However, these authors assessed the middle deltoid and acknowledged that the 200 to 300 ms values may fluctuate based on the muscle group under study. Further study of SEMG processing may be helpful to determine the preferred window length for weight‐bearing tasks requiring dynamic contractions in lower limb musculature.
Identifying eccentric and concentric components of muscle activity is interesting because it has been found that concentric contraction results in higher EMG amplitude44 and lower mean SEMG frequency45 compared to eccentric contraction. Several SEMG studies have differentiated concentric and eccentric muscle activity during weight bearing tasks by kinematic analysis of joint positions11,13 and ground reaction force data.21 The current study did not employ kinematic or kinetic analysis, thus the authors are unable to accurately identify concentric or eccentric contractions during the unilateral weight bearing tasks. Therefore, eccentric and concentric phases were combined during the SEMG analysis which is similar to other studies.9,10,14,16,20,26
The gluteus medius muscle was found to be statistically most active during the step down task (14%MVIC) compared to either the side‐step (13%MVIC) or lunge (12%MVIC) for both the men and the women. The gluteus maximus muscle elicited higher activity when the participants performed the step down task (13%MVIC) as compared to the lunge (10‐11%MVIC). Despite muscle activity differences, all of the SEMG values fell well below the 40% to 60% intensity levels necessary for strengthening.46 In general, the trunk muscles responded similarly regardless of exercise and the values ranged from 11 to 15%MVIC. Thus, taking into account the low SEMG activity levels for both the core and lower extremity muscles observed during the three functional tasks might help guide clinicians in selecting interventions.
A significant limitation to the current study is the lack of range of motion and strength data. This investigation also did not assess trunk and lower extremity flexibility. Another possible limitation to the current study is that true maximum effort was not produced by the subjects during muscle testing used to establish the MVIC. In order to motivate the subjects, verbal encouragement was provided to everyone. While the current study recruited both men and women for this study, the participants were relatively young, healthy, and recreationally active.
Cross‐talk with the use of SEMG electrodes from adjacent muscles may be a limitation, as in any SEMG study. The current investigation used standardized electrode placement for each of the muscles assessed in our study.36,37 It has been suggested that using the standardized method for SEMG placement improves the recordings at each of the muscles sites.36
CONCLUSION
Gender differences in SEMG measures of muscle activity among the three selected weight bearing ‐single‐limb exercises were not found. This may be due, in part to using adjusted distances and step heights based on the participants' leg length. The information gained from this study has raised questions as to how muscle patterns are affected using normalized distances based on leg length among women. This study also demonstrated that the forward or side‐step lunge and step down tasks demand low levels of core and lower extremity muscle activation. While gluteus maximus and gluteus medius were more active during these tasks compared to the trunk, hip flexor, or hamstring muscles, they still were well below the intensity necessary for strengthening.
REFERENCES
- 1.Ireland ML, Davis IS, Ballantne BT, Wilson JD. Hip strength in females with and without patellofemoral pain. J Orthop Sports Phys Ther. 2003;33:671‐676 [DOI] [PubMed] [Google Scholar]
- 2.Leetun DT, Ireland ML, Wilson JD, Ballantyne TB, Davis IM. Core stability measures as risk factors for lower extremity injury in athletes. Med Sci Sport Exerc. 2004;36:926‐934 [DOI] [PubMed] [Google Scholar]
- 3.Powers CM. The influence of altered lower‐extremity kinematics on patellofemoral joint dysfunction: a theoretical perspective. J Orthop Sports Phys Ther. 2003;33:639‐646 [DOI] [PubMed] [Google Scholar]
- 4.Robinson RL, Nee RJ. Analysis of hip strength in females seeking physical therapy treatment for unilateral patellofemoral pain syndrome. J Orthop Sports Phys Ther. 2007;37:232‐237 [DOI] [PubMed] [Google Scholar]
- 5.Bolgla LA, Malone TR, Umberger BR, Uhl TL. Comparsion of hip and knee strength and neuromuscular activity in subjects with and without patellofemoral pain syndrome. Int J Sports Phys Ther. 2011;6;285‐295 [PMC free article] [PubMed] [Google Scholar]
- 6.Dolak KL, Silkman C, McKeon JM, Hosey RG, Latterman C, Uhl T. Hip strengthening prior to functional exercises reduces pain sooner than quadriceps strengthening in females with patellofemoral pain syndrome: a randomized clinical trial. J Orthop Sports Phys Ther. 2011;41:560‐570 [DOI] [PubMed] [Google Scholar]
- 7.Farrokhi S, Pollard CD, Souza RB. Trunk position influences the kinematics, kinetics, and muscle activity of the lead lower extremity during the forward lunge exercise. J Orthop Sports Phys Ther. 2008;38:403‐409 [DOI] [PubMed] [Google Scholar]
- 8.Chen HY, Chien CC, Wu SK, Liau JJ, Jan MH. Electromechanical delay of the vastus medialis obliquus and vastus lateralis in individuals with patellofemoral pain syndrome. J Orthop Sports Phys Ther. 2012;42:791‐796 [DOI] [PubMed] [Google Scholar]
- 9.Ekstrom RA, Donatelli RA, Carp KC. Electromyographic analysis of core trunk, hip, and thigh muscles during 9 rehabilitation exercises. J Orthop Sports Phys Ther. 2007;37:754‐762 [DOI] [PubMed] [Google Scholar]
- 10.Distefano LJ, Blackburn JT, Marshall SW, Padua DA. Gluteal muscle activation during common therapeutic exercises. J Orthop Sports Phys Ther. 2009;39:532‐540 [DOI] [PubMed] [Google Scholar]
- 11.Dwyer MK, Boudreau SN, Mattacola CG., Uhl TL, Lattermann C. Comparison of lower extremity kinematics and hip muscle activation during rehabilitation tasks between sexes. J Athl Train. 2010;45:181‐190 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Myer GD, Ford KR, Hewett TE. The effects of gender on quadriceps muscle activation strategies during a maneuver that mimics a high ACL injury risk position. J Electromyogr Kinesiol. 2005;15(2):181‐189 [DOI] [PubMed] [Google Scholar]
- 13.Jonhagen S, Halvorsen K, Benoit DL. Muscle activation and length changes during two lunge exercises: implications for rehabilitation. Scand J Med Sci Sports 2009;19:561‐568 [DOI] [PubMed] [Google Scholar]
- 14.Ayotte NW, Stetts DM, Keenan G, Greenway EH. Electromyographical analysis of selected lower extremity muscles during 5 unilateral weight‐bearing exercises. J Orthop Sports Phys Ther. 2007;37:48‐55 [DOI] [PubMed] [Google Scholar]
- 15.Boudreau SN, Dwyer MK, Mattacola CG, Lattermann C, Uhl TL, McKeon JM. Hip‐muscle activation during the lunge, single‐leg squat, and step‐up‐and‐over exercises. J Sport Rehab. 2009;18:91‐103 [DOI] [PubMed] [Google Scholar]
- 16.Zeller BL, McCrory JL, Kibler WB, et al. Differences in kinematics and electromyographic activity between men and women during the single‐legged squat. Am J Sport Med. 2003;31(3):449‐456 [DOI] [PubMed] [Google Scholar]
- 17.Bowyer D, Armstrong M, Dixon J, Smith TO. The vastus medialis oblique: vastus lateralis electromyographic intensity ratio does not differ by gender in young participants without knee pathology. Physiotherapy 2008;94:168‐173 [Google Scholar]
- 18.Cowan SM, Crossley KM. Does gender influence neuromuscular control of the knee and hip? J Electromyogra Kinesiol. 2009;19:276‐282 [DOI] [PubMed] [Google Scholar]
- 19.Earl JE, Monteiro SK, Snyder KR. Differences in lower extremity kinematics between a bilateral drop‐vertical jump and a single‐leg step‐down. J Orthop Sports Phys Ther. 2009;37:245‐252 [DOI] [PubMed] [Google Scholar]
- 20.Hollman JH, Ginos BE, Kozuchowski J, Vaughn AS, Krause DA, Youdas JW. Relationships between knee valgus, hip‐muscle strength, and hip‐muscle recruitment during a single‐limb step‐down. J Sport Rehabil. 2009;16:104‐117 [DOI] [PubMed] [Google Scholar]
- 21.Stemmons Mercer V, Gross MT, Sharma S, Weeks E. Comparison of gluteus medius muscle electromyographic activity during forward and lateral step‐up exercises in older adults. Phys Ther. 2009;89:1205‐1214 [DOI] [PubMed] [Google Scholar]
- 22.Beaulieu ML, Lamontagne M. Lower limb activity and kinematics of an unanticipated cutting manoeuvre: a gender comparison. Knee Surg Sports Traumatol Arthrosc. 2009;17:968‐976 [DOI] [PubMed] [Google Scholar]
- 23.Hanson AM, Padua DA, Blackburn JT, Prentice WE, Hirth C. Muscle activation during side‐step cutting maneuvers in male and female soccer athletes. J Athl Train. 2008;43:133‐143 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Youdas JW, Hollman JH, Hitchcock JR, Hoyme GJ, Johnsen JJ. Comparison of hamstring and quadriceps femoris electromyographic activity between men and women during a single‐limb squat on both a stable and labile surface. J Strength Cond Res. 2007;21:105‐111 [DOI] [PubMed] [Google Scholar]
- 25.Beutler AJ, Cooper LW, Kirkendall DT, Garrett WE. Electromyographic analysis of single‐leg closed chain exercises: Implications for rehabilitation after anterior cruciate ligament reconstruction. J Athl Train. 2002;37:13‐18 [PMC free article] [PubMed] [Google Scholar]
- 26.Zazulak BT, Ponce PL, Straub SJ, et al. Gender comparison of hip muscle activity during single‐leg landing. J Orthop Sports Phys Ther 2005;35(5):292‐299 [DOI] [PubMed] [Google Scholar]
- 27.Russell KA, Palmieri RM, Zinder SM, et al. Sex differences in valgus knee angle during a single‐leg landing. J Athl Train. 2006;41:166‐171 [PMC free article] [PubMed] [Google Scholar]
- 28.Landry SC, McKean KA, Hubley‐Kozey CL, et al. Neuromuscular and lower limb biomechanical differences exist between male and female elite adolescent soccer players during an unanticipated side‐cut maneuver. Am J Sports Med. 2007;35(11):1888‐1890 [DOI] [PubMed] [Google Scholar]
- 29.McLean SG, Lipfert SW, van den Bogert AJ. Effect of gender and defensive opponent on the biomechanics of side‐step cutting. Med Sci Sports Exerc. 2004;36(6):1008‐1016 [DOI] [PubMed] [Google Scholar]
- 30.Imwalle LE, Myer GD, Ford KR, et al. Relationship between hip and knee kinematics in athletic women during cutting maneuvers: a possible link to noncontact anterior cruciate ligament injury and prevention. J Strength Cond Res. 2009;23(8):2223‐2230 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Malinzak RA, Colby SM, Kirkendall DT, Yu B, Garrett WE. A comparison of knee joint motion patterns between men and women in selected athletic tasks. Clin Biomech (Bristal Avon). 2001;16(5):438‐445 [DOI] [PubMed] [Google Scholar]
- 32.Hewett TE, Myer GD, Ford KR, et al. Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: a prospective study. Am J Sports Med 2005;33:4492‐501 [DOI] [PubMed] [Google Scholar]
- 33.Carson DW, Ford KR. Sex differences in knee abduction during landing: a systematic review. Sports Health 2011;3:373‐382 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Hart J, Garrison J, Palmeri‐Smith R, Kerrigan D, Ingersoll C. Lower extremity joint moments of collegiate soccer players differ between genders during a forward jump. J Sport Rehabil. 2008;17: 137‐147 [DOI] [PubMed] [Google Scholar]
- 35.Padua DA, Aarnold BL, Carcia CR, Granata KP. Gender differences in leg stiffness and stiffness recruitment strategy during two‐legged hopping. J Mot Behav. 2005;37(2):111‐126 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Criswell E. Cram's introduction to surface electromyography. 2nd ed. Jones and Bartlett Pub., 2011. p 5‐7 [Google Scholar]
- 37.Rainoldi A, Melchiorri G, Caruso I. A method for positioning electrodes during surface EMG recordings in lower limb muscles. J Neuroscience Methods. 2004;134:37‐43 [DOI] [PubMed] [Google Scholar]
- 38.Perroto A. Anatomical guide for the electromyographer: the limbs and trunk. Springfield, IL: Charles C Thomas; 2005 [Google Scholar]
- 39.Flanagan SP, Kessans KM, Salen GJ. Quantifying bilateral joint contributions during three variations of the step exercises. J Sport Rehabil. 2006;15:255‐265 [Google Scholar]
- 40.Kendall FP, McCreary EK, Provance PG, Rodgers MM, Romani WA. Muscles: Testing and Function with Posture and Pain. 5th ed. Baltimore, MD: Lippincott Williams & Wilkins; 2005 [Google Scholar]
- 41.Hislop HJ, Montgomery J. Muscle testing techniques of muscle examination. Philadelphia, PA. W.B. Saunders Co. 2002 [Google Scholar]
- 42.Munro BH. Statistical Methods for Health Care Research, 3rd Ed. NY: Lippincott William and Wilkins, 1997 [Google Scholar]
- 43.Farfan F, Politti J, Felice C. Evaluation of EMG processing techniques using information theory. Biomedical Engineering Online 2010;9:72‐90 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Moritani T, Muramatsu Muro M, Activity of motor units during concentric and eccentric contractions. Am J Phys Med. 1988;66:338‐350 [PubMed] [Google Scholar]
- 45.McHugh MP, Tyler TF, Greenberg SC, Gleim GW, Differences in activation patterns between eccentric and concentric quadriceps contraction. J Sport Sci. 2002;20:83‐91 [DOI] [PubMed] [Google Scholar]
- 46.Andersen LL, Magnusson SP, Nielsen M, Haleem J, Poulsen K, Aagaard P. Neuromuscular activation in conventional therapeutic exercises and heavy resistance exercises: implications for rehabilitation. Phys Ther. 2006;86:683‐697 [PubMed] [Google Scholar]