

Abstract
INTRODUCTION
Interphalangeal joint of foot is a very unusual location for gouty arthritis and sildenafil use may cause this phenomenon.
PRESENTATION OF CASE
A 58-year-old hypertensive man was admitted to hospital with pain and swelling over interphalengeal joint of his right great toe. His health history included the use of diuretics for a long time and his last gout attack was two years ago at first metatarsophalengeal joint of right foot. Sildenafil, a selective inhibitor of phosphodiesterase type 5 (PDE5), was administered in case of erectile dysfunction for two months. Subsequently, he had several episodes of pain and swelling at first interphalangeal joint of right great toe. Both the onset and recurrence of symptoms were just seen the day after sildenafil use. The patient was free of symptoms after discontinuation of the drug. After an initial evaluation, gout was diagnosed on the basis of synovial fluid analysis.
DISCUSSION
This case demonstrates a rare location of gouty arthritis with an uncommon etiology: sildenafil. Regarding the clinical data, the discussion was made to expand the horizon for diagnosis of patients with similar symptoms, to identify risk factors for gout relevant to elderliness, and to review the management of gout.
CONCLUSION
Sildenafil use may cause gouty arthritis, and surgical decompression may be helpful for definitive diagnosis and symptom relief in atypical presentation of gout.
Keywords: Arthritis, Gouty/chemically induced, Interphalengeal joint, Sildenafil
1. Introduction
Gout is a clinical condition affecting 1% of adult males in developed countries.1 It is the most common cause of inflammatory joint disease in men aged over 40 years.1 Deposition of monosodium urate monohydrate crystals into joint and soft tissue is the underlying pathology and there is a causative relationship between elevated blood uric acid level and urate crystal formation. Although the exact trigger mechanism of an acute attack is poorly understood, predictors for the development of gout in hyperuricemic individuals have been identified.2 These include increased uric acid level, alcohol consumption, hypertension, use of drugs especially antihypertensives, increased body mass index, and family history of gout.2–4 Sildenafil, a selective inhibitor of cyclic guanosine monophosphate (cGMP)-specific phosphodiesterase type 5 (PDE5), may rarely cause gouty arthritis.5 Gout can either manifest as acute arthritis or chronic arthropathy, which is also called tophaceous gout.1,6 Gouty arthritis is most commonly seen at metatarsophalangeal joint. We here report an uncommon case of tophus formation at first interphalengeal joint of foot, probably due to sildenafil use.
2. Case presentation
A 58-year-old male patient was admitted to hospital with two-month history of moderate pain and swelling over interphalangeal joint of his right great toe, which was affecting shoewear. The pain was out of proportion with swelling and worse at nights after using medication for erectile dysfunction. He had visited two primary care physicians before admission and was prescribed pain killers for his acute symptoms. His health history included two previous episodes of gout in both first metatarsophalangeal joints (2 and 4 years prior), hypertension and coronary artery disease for 8 years. His medications were perindopril (4 mg), hydrochlorothiazide (25 mg), salicylic acid (100 mg), allopurinol (800 mg) and colchicine (0.5 mg). He denied smoking, but occasional alcohol use was noted on every weekend. He was not on any particular diet. Due to erectile dysfunction, he has taken 100 mg sildenafil p.o. weekly for 2 months and was still on medication just before the day of admission. Any contributory family history or allergy history were not noted. Physical examination revealed 3 cm × 2 cm tender swelling without cellulitis or ulceration over dorsomedial aspect of first interphalengeal joint of right foot (Picture 1). Joint motion was extremely limited due to pain and swelling. There were no other swellings or tophi noted especially on ears or other joints. He had an average built with body mass index (BMI) of 27.4.
Picture 1.

Swelling over dorsomedial aspect of first interphalengeal joint of right foot.
Plain radiography of right foot showed joint effusion, and soft tissue swelling around first interphalengeal joint (Fig. 1). Laboratory data were within normal limits (Table 1). In the operating room, surgical decompression of first interphalangeal joint of his right foot was performed with a dorsomedial incision over swelling (Pictures 2 and 3). Debris consisted of thick, chalky, white material corresponding to gouty tophus (Picture 2). The surgical approach was adequate to expose the articular surfaces. After debridement and vigorous irrigation with sterile saline solution, intraarticular methyprednisolone 20 mg was injected to the affected site. Incision was gently sutured without tightening. Additional indomethacin 50 mg was prescribed three times daily for 10 days. His pain scale was 7/10 and 3/10 before and after surgery, respectively. Synovial fluid analysis was confirmatory (Table 2). Light microscopy of debris demonstrated gouty tophi consisting of monosodium urate crystals (Fig. 2). Microscopic examination of the specimen revealed polynuclear giant cells and histiocytes around needle-like void spaces and granular nodule formation was seen (Fig. 3). Wound healing was observed on day 18 without complication. The patient was free of symptoms at 2 months, postoperatively.
Fig. 1.

Plain radiography of right foot showing joint effusion, and soft tissue swelling around first interphalengeal joint.
Table 1.
Laboratory data at admission.
| Test | Value | Value range |
|---|---|---|
| WBC | 8200 mm3 | 4–10 |
| Hemoglobin | 12.1 g/dl | 12.5–16.5 |
| Sodium | 141 meq/l | 135–145 |
| Potassium | 3.9 meq/l | 3.5–4.9 |
| Chloride | 105 meq/l | 96–110 |
| BUN | 19 mg/dl | 6.0–23.0 |
| Creatinine | 0.8 mg/dl | 0.6–1.4 |
| Total protein | 5.4 g/dl | 6.0–8.0 |
| Albumin | 3.7 g/dl | 3.6–5.0 |
| Calcium | 8.2 mg/dl | 8.0–10.5 |
| Hemoglobin | 11.6 g/dl | 12.6–16.5 |
| Platelet count | 236,000 mm3 | 150–400 |
| Uric acid | 6.4 mg/dl | 3.4–7.0 |
Picture 2.

Debris consisting of thick, chalky, white material corresponding to gouty tophus.
Picture 3.

Closure of dorsomedial incision after decompression.
Table 2.
Synovial fluid analysis.
| Test | Value | Normal |
|---|---|---|
| Clarity | Translucent | Transparent |
| Color | Whitish Yellow | Clear |
| WBC (per mm3) | 2000 | <200 |
| PMNs (%) | 55 | <25 |
| Gram stain | No organisms | No organisms |
| Culture | Negative | Negative |
| Total protein (g/dl) | 1.9 | 3.1 |
| LDH (IU/l) | 494 | 105–330 |
| Glucose (mg/dl) | 44 | 70–110 |
| Crystal | Monosodium urate crystals | None |
Fig. 2.
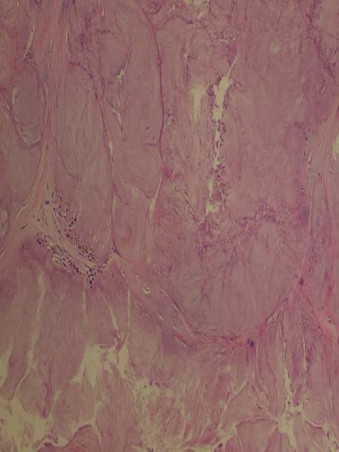
Light microscopy of debris demonstrating gouty tophi consisting of monosodium urate crystals.
Fig. 3.
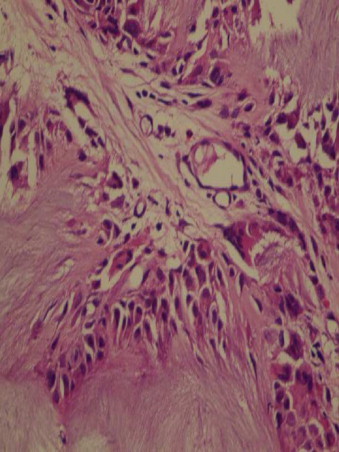
Microscopic examination of the specimen revealing polynuclear giant cells and histiocytes around needle-like void spaces and granular nodule formation.
3. Discussion
Gout is a metabolic disease that can manifest as acute or chronic arthritis with deposition of urate crystals in connective tissue and kidneys. Gouty tophi are commonly found in articular and other cartilages; in synovium, tendon sheaths, and other periarticular structures; in epiphyses, and in subcutaneous layers of the skin in the extremities. Tophi are most often seen in tissues that have a poor blood supply and low temperature, such as the ear helix and first metatarsophalengeal joint.7 The nodules are yellowish-white, and non-tender, and range in size from 1 mm to 7 cm. Aspiration yields a chalky-like material that appears as needle-like crystals under light microscopy. All patients have hyperuricemia at some point of their disease. Hyperuricemia results from either decreased renal excretion (which occurs in 90% of gout patients) or hyperproduction of uric acid.8 Drugs that may cause hyperuricemia and gout include diuretics, cyclosporine, low-dose aspirin, ethambuthol, pyrzinamide, and nicotinic acid.9 Sildenafil, a selective inhibitor of cyclic guanosine monophosphate (cGMP)-specific phosphodiesterase type 5 (PDE5), may also play a role in the etiology.5 In pre-marketing clinical trials over 3700 patients, rare adverse events reported with sildenafil in adults (all <2%) include arrhythmias, cerebral thrombosis, hypertonia, paresthesias, priapism, migraine, tremor, photosensitivity, colitis, vomiting, abnormal liver function tests, anemia, leukopenia, gout, arthritis, dyspnea, and allergic reactions.5 Exact mechanism of sildenafil to trigger a gout attack is not known, but PDE5 is also found in platelets, vascular and visceral smooth muscle, and skeletal muscle in addition to corpus cavernosum. Inhibition of PDE5 in these tissues by sildenafil may increase antiaggregatory activity of nitric oxide and peripheral arterial-venous dilatation.5 Chen et al. reported a case of acute gouty arthritis at first metatarsophalengeal joint after taking sildenafil. The patient had several attacks only after administration of sildenafil, implying a causal relation between sildenafil and gout episodes.10 Since our patient's last attack was two years ago, and both the onset and recurrence of symptoms were just seen the day after sildenafil use, it was considered that there was a causal relation with detoriation of symptoms and the medication. Furthermore, our case had gout attacks at interphalengeal joint of right great toe which is very uncommon location for gouty arthritis. Literature review yielded only one case of gouty arthritis at interphalangeal joint of big toe that is reported as an atypical presentation of gout by Dobson et al.11
As some are commonly prescribed, it is important that physicians dealing with musculoskeletal diseases and erectile dysfunction must be aware of the medications that their patients are taking. So far, increasing attention has been drawn to the role played by diuretics in the pathogenesis of gout, particularly in the elderly, however, the use of phosphodiesterase inhibitors may also contribute to the progression of disease. Gouty arthritis is caused by intense inflammation secondary to monosodium urate crystal deposition in joints. Tophus is often found in the auricular cartilage or metatarsophalengeal joint of great toe. We presented a patient with gouty tophus formation at the first interphalengeal joint of his right foot. Local factors that contribute to tophus formation are changes in perioperative pH level, lower body temperature, explaining nocturnal attacks; and the level of articular dehydration due to diuretics.8 The goals of gout treatment are symptom control for acute attacks, risk factor modification, pharmacotherapy to prevent recurrence and chronic sequelae in the long run, and surgical decompression of tophi for pain management.
Tophaceous gout may lead to significant morbidity and, if untreated, can cause joint erosion and destruction.9 Tophaceous material may present in a liquid, pasty, or chalky/granular state. Treatment may be as simple as aspirating the liquid or squeezing out pasty tophaceous material. Surgery is often indicated for the patient with significant tendon and joint compromise as well as skin breakdown. Surgical decompression followed by optimization of pharmacologic treatment and lifestyle modification provide good recovery.
Conclusion
Sildenafil use may rarely cause gouty arthritis. Interphalengeal joint involvement of great toe is atypical for gout and surgical decompression may be helpful for definitive diagnosis and symptom relief.
Competing interests
The authors declare that they have no competing interests.
Funding
None.
Consent
Written informed consent was obtained from the patient for the publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Authors’ contributions
TA, YI, ME, and HG were involved in conception, design and interpretation. TA and YI wrote the manuscript. TA, YI, and ME collected data, reviewed the literature, and provided the images. All authors read and approved the final version submitted.
Contributor Information
Tugrul Alici, Email: tugrulalici@yahoo.com.
Yunus Imren, Email: yunusimren@yahoo.com.
Mehmet Erdil, Email: drmehmeterdil@gmail.com.
Hakan Gundes, Email: gundesh@yahoo.com.
References
- 1.Krishnan E., Griffith C., Kwoh C. Burden of illness from gout in ambulatory care in the United States. Arthritis and Rheumatism. 2005;52(9 Suppl.):S656. [Google Scholar]
- 2.Wallace K.L., Riedel A.A., Joseph-Ridge N., Wortmann R. Increasing prevalence of gout and hyperuricemia over 10 years among older adults in a managed care population. Journal of Rheumatology. 2004;31:1582–1587. [PubMed] [Google Scholar]
- 3.Vasan R.S., Pencina M.J., Cobain M., Freiberg M.S., D’Agostino R.B. Estimated risks for developing obesity in the Framingham Heart Study. Annals of Internal Medicine. 2005;143:473–480. doi: 10.7326/0003-4819-143-7-200510040-00005. [DOI] [PubMed] [Google Scholar]
- 4.Fitzgerald B.T., Setty A., Mudgal C.S. Gout affecting the hand and wrist: review. Journal of the American Academy of Orthopaedic Surgeons. 2007;15(October (10)):625–635. doi: 10.5435/00124635-200710000-00007. [DOI] [PubMed] [Google Scholar]
- 5.Pfizer Labs; 2002. Viagra® product information. Available at: www.viagramd.com/pi/proPackInsert.asp. [Google Scholar]
- 6.Mikuls T.R., Farrar J.T., Bilker W.B., Fernandes S., Saag K.G. Suboptimal physician adherence to quality indicators for the management of gout and asymptomatic hyperuricaemia: results from the UK General Practice Research Database (GPRD) Rheumatology. 2005;44:1038–1042. doi: 10.1093/rheumatology/keh679. [DOI] [PubMed] [Google Scholar]
- 7.Janssens H.J., Janssen M., Lisdonk E.H., van Riel P.L., van Weel C. Use of oral prednisolone or naproxen for the treatment of gout arthritis: a double-blind, randomised equivalence trial. Lancet. 2008:1854–1860. doi: 10.1016/S0140-6736(08)60799-0. [DOI] [PubMed] [Google Scholar]
- 8.Eggebeen A.T. Gout: an update. American Family Physician. 2007;76(September (6)):801–808. [PubMed] [Google Scholar]
- 9.Kuo Y.J., Chiang C.J., Tsuang Y.H. Gouty arthropathy of the cervical spine in a young adult. Journal of Chinese Medical Association. 2007;70(April (4)):180–182. doi: 10.1016/S1726-4901(09)70354-5. [DOI] [PubMed] [Google Scholar]
- 10.Chen W.L., Chen H.I., Loh C.H. Acute gouty arthritis after taking sildenafil: an old disease with a new etiology. Journal of Rheumatology. 2009;36(January (1)):210–211. doi: 10.3899/jrheum.080572. [DOI] [PubMed] [Google Scholar]
- 11.Dobson M., Alwahab Y., Fazal M.A. Interphalangeal joint involvement of the big toe in gout: a rare presentation. Journal of the American Podiatric Medical Association. 2012;102(May–June (3)):256–258. doi: 10.7547/1020256. [DOI] [PubMed] [Google Scholar]