

Abstract
Objective
To assess whether high school football played between 1946 and 1956, when headgear was less protective than today, was associated with development of neurodegenerative diseases later in life.
Methods
All male students who played football from 1946 to 1956 in the high schools of Rochester, Minnesota, plus a non–football-playing referent group of male students in the band, glee club, or choir were identified. Using the records-linkage system of the Rochester Epidemiology Project, we reviewed (from October 31, 2010, to March 30, 2011) all available medical records to assess later development of dementia, Parkinson disease (PD), or amyotrophic lateral sclerosis (ALS). We also compared the frequency of dementia, PD, or ALS with incidence data from the general population of Olmsted County, Minnesota.
Results
We found no increased risk of dementia, PD, or ALS among the 438 football players compared with the 140 non–football-playing male classmates. Parkinson disease and ALS were slightly less frequent in the football group, whereas dementia was slightly more frequent, but not significantly so. When we compared these results with the expected incidence rates in the general population, only PD was significantly increased; however, this was true for both groups, with a larger risk ratio in the non–football group.
Conclusion
Our findings suggest that high school students who played American football from 1946 to 1956 did not have an increased risk of later developing dementia, PD, or ALS compared with non–football-playing high school males, despite poorer equipment and less regard for concussions compared with today and no rules prohibiting head-first tackling (spearing).
Abbreviations and Acronyms: ALS, amyotrophic lateral sclerosis; CTE, chronic traumatic encephalopathy; PD, Parkinson disease; REP, Rochester Epidemiology Project
Multiple concussive head injuries incurred in sporting activities previously have been associated with progressive neurodegenerative disease later in life. Initially, it was reported in boxers (dementia pugilistica),1 but an evolving literature now suggests that this risk extends to other sports in which concussions are common. The term chronic traumatic encephalopathy (CTE) has been used to define this condition, with dementia being the primary delayed outcome.2 Besides fighting sports, American football, soccer, and hockey predispose players to head trauma and have been implicated in the later development of CTE.3,4 Moreover, head trauma and sport-related trauma have been reported as risk factors for development of Parkinson disease (PD),5 dementia,6 and amyotrophic lateral sclerosis (ALS).7,8
Although repeated concussive head trauma is a purported risk factor for later neurodegenerative disease, few studies have evaluated long-term risks in a cohort of athletes participating in a sport that is often associated with concussions.9 American football as played several decades ago often put participants at risk for concussion, which at the time was commonly disregarded (“bell rung”); moreover, the protective headgear of that era was marginally protective against concussions (Figure 1). We chose to analyze the long-term medical outcomes of a cohort of high school football players from Rochester (Olmsted County), Minnesota, using the medical records linkage system of the Rochester Epidemiology Project (REP).10,11 We hypothesized that athletes playing football during the decade 1946-1956 would be more likely to develop a neurodegenerative condition later in life than non–football players. Because CTE has been linked to dementia, PD, and ALS, we specifically assessed the frequency of these 3 conditions from the historical medical records. We compared outcomes in the high school football cohort with outcomes in male classmates from the same years who participated in band, glee club, or choir but did not participate in any sport activity. We also compared our results with the expected frequency of dementia, PD, and ALS as determined by using previously published sex- and age-adjusted incidence rates of the general population of Olmsted County.
FIGURE 1.
One of the football players from Rochester Lourdes High School in 1946 wearing a “dog-ear” leather helmet.
Photo courtesy of Lourdes High School, Rochester, MN. Used with permission.
Methods
Study Population and Medical Records Abstraction
During the years of interest, 1946-1956, Rochester had only 2 high schools: Lourdes High School and Rochester High School. Yearbooks were available for these high schools, documenting rosters of football players, as well as members of the band, glee club, and choir (non–football players). We created lists of the male members of these respective groups; football players who also participated in band, glee club, or choir were included only in the list of football players. The yearbooks contained at least the following information: full name, year of graduation, and the activities performed during the previous years in high school. Soccer, tennis, boxing, and hockey were not available sports during these study years.
We linked the individuals in these 2 groups to their medical records, taking advantage of the REP browser. The REP is a unique medical records linkage system that encompasses the care delivered to residents of Olmsted County (including the city of Rochester). All individuals visiting any county care provider are present in the system. This is an active records linkage system that spans from the early 1900s to the present. Further details on the REP have been reported elsewhere.10,11 The REP includes a tool that allows one to search for individuals on the basis of their first and last names and the year of birth. We searched for each person on our compiled lists, using his full name and the approximate year of birth (assuming that students graduated at age 18±2 years).
The study population was limited to only those individuals who had a medical record in the records linkage system and for whom we could confirm a match with our compiled lists. Individuals were included in the REP if they had at least one medical visit in their lifetime at any of the medical facilities in Olmsted County. Therefore, those who left Olmsted County before generating any medical records were not included.
A 2-step process was used to abstract the medical record. First, we screened the electronic medical indexes of the records linkage system using the REP tools. We focused our search on dementia of any type, parkinsonism of any type, and ALS. Second, a neurologist (R.S.), unaware of the status of the individuals (football players vs non–football players), reviewed the complete available medical charts of all those who ever received one of the diagnoses in order to confirm the electronic-based diagnosis. To determine the reliability of the clinical diagnosis of the abstractor, we compared his diagnoses with a set of electronic codes that already had been used in a previous study on the incidence of parkinsonism in the same population.12 There were no differences between the diagnoses made by the neurologist and the cases identified by the electronic codes.
In addition, we reviewed autopsy reports and stored brain tissues when available. The study protocol and all procedures were approved by the institutional review boards of Mayo Clinic and Olmsted Medical Center. The study was performed from October 31, 2010, to March 30, 2011.
Data Analyses
We calculated the median, 25th percentile, and 75th percentile for the years of follow-up and the age at follow-up. To compare groups for length of follow-up and age at follow-up, we reported P values from the Wilcoxon rank sum test. We performed 2 separate analyses to determine if playing football increased the risk of dementia, PD, or ALS. First, we compared the football cohort directly to the cohort of students who participated in band, choir, or glee club. Individuals were followed up until the time of last available medical record information or until the time of onset of one of the outcomes of interest (dementia, PD, or ALS). We then performed Cox proportional hazards analysis and calculated a hazards ratio (HR) and 95% confidence interval (CI).
We calculated separately for the football cohort and the non–football cohort the expected number of persons with the outcomes of interest (dementia, PD, and ALS) based on incidence rates previously published for the population of Olmsted County.12-14 Specifically, the expected number of outcomes was calculated by applying incidence rates to the age- and sex-specific person-years of follow-up in our study in the same years covered by the historical rates. We then calculated standardized incidence ratios (SIRs) to summarize this comparison. All analyses were performed by a statistician (not a coauthor) at the conventional 2-tailed α level of .05 using SAS version 9 (SAS Institute Inc, Cary, NC).
Results
We identified 512 male football players and 203 male members of the band, glee club, or choir from high school classes between 1946 and 1956. Among these, we were able to successfully match 438 football players (86%) and 140 band, glee club, or choir members (69%) to a record in the REP system (Figure 2).
FIGURE 2.
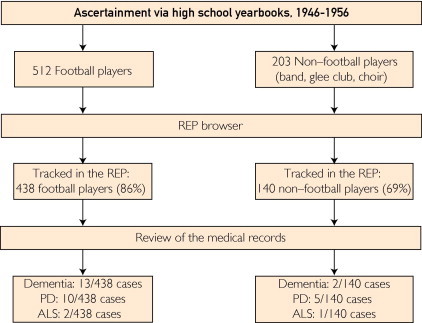
Flowchart of the study. ALS = amyotrophic lateral sclerosis; PD = Parkinson disease; REP = Rochester Epidemiology Project.
The median period of follow-up in the system was 50.2 years (interquartile range [IR], 13.7-57.5) for the football players and 42.7 years (IR, 8.8-55.4) for the non–football players. The age at the last follow-up was 68.4 years (IR, 31.5-75.6) for the football players and 59.1 years (IR, 26.7-73.4) for the band, glee club, and choir members.
We identified 13 cases of dementia of any type among the football players and 2 cases among the non–football players; the difference between groups was not significant (HR, 1.58; 95% CI, 0.36-7.01; P=.55). Our observed cases were fewer than expected in both groups, compared with Olmsted County incidence data (expected number of dementia cases in the football cohort, 18.2; expected number of dementia cases in the non–football cohort, 4.3). However, the differences between observed and expected were not significant (SIR, 0.72; 95% CI, 0.38-1.23 in the football players and SIR, 0.47; 95% CI, 0.05-1.68 in the non–football cohort). The median age at the onset of dementia was 72.4 years (IR, 69.3-77.0) in the football players and 76.0 years (IR, 75.0-77.0) in the non football cohort.
Parkinson disease was identified in 10 football players and 5 band, glee club, or choir members, which was statistically similar (HR, 0.48; 95% CI, 0.17-1.42; P=.19). Olmsted County incidence data predicted a PD frequency of 4.2 cases in football players and 1.0 case in band, glee club, or choir members; although comparison of observed frequency with this population-based data showed a statistically significant difference, this was true for both groups (SIR, 2.36; 95% CI, 1.13-4.34 in the football players and SIR, 4.94; 95% CI, 1.61-11.51 in the non–football cohort). The median age at onset of PD was 70.5 years (IR, 58.9-77.4) in the football players and 67.7 years (IR, 55.5-78.1) in the band, glee club, or choir members.
Amyotrophic lateral sclerosis was the only motor neuron disease subtype that we identified, and it was diagnosed in 2 football players and 1 band, glee club, or choir member (HR, 0.52; 95% CI, 0.05-5.68; P=.59). We also found no significant difference between observed and population-based expected number of cases for either group (SIR, 3.15; 95% CI, 0.38-11.33 in the football players and SIR, 6.44; 95% CI, 0.16-35.7 in the non–football cohort) (Tables 1 and 2).
TABLE 1.
Historical Cohort Study of Football Players vs Non–Football Players and Risk of Neurodegenerative Diseasesa
| Football players (N=438) | Band/glee club/choir members (N=140) | HR | 95% CI | P valueb | |
|---|---|---|---|---|---|
| Follow-up | |||||
| Years of follow-upc | 50.2 (13.7, 57.5) | 42.7 (8.8, 55.4) | … | … | .03 |
| Age at follow-upc | 68.4 (31.5, 75.6) | 59.1 (26.7, 73.4) | … | … | .01 |
| Outcome | |||||
| Dementia | 13 | 2 | 1.58 | 0.36-7.01 | .55 |
| Parkinson disease | 10 | 5 | 0.48 | 0.17-1.42 | .19 |
| Amyotrophic lateral sclerosis | 2 | 1 | 0.52 | 0.05-5.68 | .59 |
HR = hazards ratio; CI = confidence interval.
P values are for the Wilcoxon rank sum test.
Values are median (25th percentile, 75th percentile).
TABLE 2.
Historical Cohort Study of Football Players and Non–Football Players vs General Population and Risk of Neurodegenerative Diseases
| Football players (N=438) | Band/glee club/choir members (N=140) | P valuea | |
|---|---|---|---|
| Dementia | |||
| Observed | 13 | 2 | |
| Expectedb | 18.1 | 4.3 | |
| SIR vs expectedc | 0.72 (0.38-1.23) | 0.47 (0.05-1.68) | |
| Years after indexd | 55.3 (51.5, 59.4) | 57.8 (57.2, 58.5) | .44 |
| Age at outcomed | 72.4 (69.3, 77.0) | 76.0 (75.0, 77.0) | .35 |
| Parkinson disease | |||
| Observed | 10 | 5 | |
| Expectedb | 4.2 | 1.0 | |
| SIR vs expectedc | 2.36 (1.13-4.34) | 4.94 (1.61-11.51) | |
| Years after indexd | 52.4 (42.4, 59.6) | 49.8 (37.4, 60.2) | .95 |
| Age at outcomed | 70.5 (58.9, 77.4) | 67.7 (55.5, 78.1) | .95 |
| Amyotrophic lateral sclerosis | |||
| Observed | 2 | 1 | |
| Expectedb | 0.64 | 0.16 | |
| SIR vs expectedc | 3.15 (0.38-11.33) | 6.44 (0.16-35.7) | |
| Years after indexd | 47.6 (46.3, 48.8) | 42.8 (42.8, 42.8) | .67 |
P values are for the Wilcoxon rank sum test.
Expected numbers of cases are calculated from age-specific person-years and previously published incidence rates in the Olmsted County population.
Standardized incidence ratios (SIRs) are calculated on the basis of observed number of cases and expected number of cases. Values are SIR (95% confidence interval).
Values are median (25th percentile, 75th percentile).
Only a single brain was available for neuropathologic examination. This was a case of motor neuron disease that occurred in the football group. Routinely processed formalin-fixed tissues from multiple neocortical and subcortical areas were stained by a variety of techniques, including antibodies to β-amyloid, tau, alpha-synuclein, and TDP-43. Review of this material revealed that tau pathology was minimal and limited to medial temporal areas, which is consistent with nonspecific age-associated changes. We did not observe any pathologic findings supportive of CTE.
Discussion
Our findings suggest that playing American football in high school between 1946 and 1956 did not increase the long-term risk of developing dementia, PD, or ALS later in life. Indeed, the frequency of PD and ALS was lower in the football group than in the band, glee club, and choir group; however, the 2 groups did not differ statistically. Although the dementia frequency was higher in the football group (3% vs 1.4%), the difference was not significant (P=.55).
Our concern was that the repetitive head trauma associated with high school football may have predisposed players to development of neurodegenerative disease similar to CTE.4 Chronic traumatic encephalopathy is an insidiously developing neurodegenerative disorder beginning many years after multiple concussive brain injuries, best described in professional athletes, and characterized by progressive dementia and parkinsonism.3 Chronic traumatic encephalopathy neuropathology is distinct from Alzheimer disease and other neurodegenerative diseases.3,4,15 Moreover, several epidemiological studies have found that prior brain trauma is a risk factor for dementia,6,16 PD,5,17 and ALS.15,18 In particular, ALS has been found to be increased in professional Italian soccer players7 and professional American football players.8
Ideally, we would have been able to document specific instances of concussions in our football cohort. However, in that era, all but the most severe concussions were largely ignored, and players often returned to the game after injury (being said to have had their “bell rung”). Thus, medical records provide few references to such injuries.
Although the body weight and bulk of athletes from the investigated era (1946-1956) were, on average, less than those of modern athletes, the helmets and football rules put the earlier athletes at greater concussive risk. Figure 1 shows a common helmet of that era, which would hardly protect the player from a concussive blow. Not until 1973 did the National Operating Committee on Standards for Athletic Equipment (NOCSAE) implement the first football helmet standards, initially for professional football19,20 and then college (1978), with high school standards not being adopted until 1980. Moreover, it was not until 1976 that rules prohibited spearing (leading with the head when blocking or tackling). Illustrating the risks to the brain, a study of American football fatalities reported that from 1945 through 1999 the major cause of death was brain injury (69%) and that most fatalities occurred from 1965 to 1969. With the adoption of NOCSAE standards, fatalities decreased by 74% and head injuries decreased from 4.25 per 100,000 to 0.69 per 100,000.21 In summary, the evolution of better helmet technology, together with further rule changes and head injury management guidelines, has further reduced football head injuries.22
For this analysis to be valid, adequate follow-up is necessary. Neurodegenerative diseases typically develop among elderly persons, although CTE may occur much earlier.4 In our study, follow-up was approximately 50 years of observation after high school graduation (median for dementia, 55 years; PD, 52.4 years; ALS, 47.6 years). The median age at last follow-up in the football group was 68.4 years, which may not extend sufficiently to ascertain all neurodegenerative diseases; however, premature neurodegenerative disease should have surfaced by that time. In addition, our analyses were adjusted either directly for age (via a matched non–football cohort) or indirectly for age (age-specific incidence rates) and did not rely on complete lifetime ascertainment.
This study has certain other limitations. Although we were able to track the vast majority of students in our system, it is possible that we have limited medical information regarding the later medical outcomes in some of them. Moreover, almost 35% of the non–football players never entered the system, either because they had no medical visits or because they no longer lived in the county; this could have led to selection bias. In addition, we can only speculate about the severity of concussions in the football cohort, as we have no direct documentation, and we were unable to include information regarding football players' time on the field, positions, or number of years played. Thus, we considered all players of equal likelihood to have suffered concussive trauma. The study sample size is relatively small, despite 10 years of ascertainment; thus, the study may be underpowered and a type II error cannot be excluded. Data were not available for other factors that might have influenced outcomes—smoking, use of caffeine, exposure to pesticides, family history, and so forth. Also, it may be noted that follow-up duration and age were greater in the football group, which should have biased toward identifying more, rather than less, neurodegenerative disease among the football players. Finally, we were able to identify only 3 cases of ALS (2 in the football group and 1 in the non–football group). Therefore, our findings should be interpreted cautiously, in light of the rarity of the outcome.
Compared with general residents of Olmsted County from the same birth year and sex, both groups, football and non–football, were less likely to develop dementia but more likely to be diagnosed with PD or ALS. Although the difference was significant only for PD, this was true for both high school groups and seems paradoxical. However, that these comparisons to population-expected cases ran parallel in our 2 high school groups suggests that other population variables affected these results. Possibly, differences in methodology between our study and the prior Olmsted County incidence studies12-14 may have contributed to these findings. For example, this might have included differences in case ascertainment. Also, individuals moving out of Olmsted County after 1 or 2 medical visits would have reduced the denominators in the prior incidence studies. Additionally, we did not collect information on death rates in our 2 groups. Finally, note that this study assessed high school males in the immediate World War II era. The prior population-based incidence study likely captured a broader group of young males, many of whom had quit or deferred high school to serve in the military. Thus, our 2 male high school groups had different demographic characteristics than males of similar age in the prior incidence studies.
Conclusion
Our findings suggest that high school football players from a well-defined community who played from 1946 to 1956 did not have an increased risk of dementia, PD, or ALS compared with non–football players. These data should be interpreted in light of the many differences between today's high school football players and those of the distant past. Although today's players have better equipment, trainers and physicians who are more knowledgeable about concussions, and rules against spearing, they also tend to be larger and quicker than athletes in the prior era, increasing the force of impact. Moreover, although dramatically different from the marginally protective headgear of this earlier era, current helmets certainly do not eliminate concussions and may provide players with a false sense of protection. Although these results should be somewhat reassuring to high school players from 50 years ago, they should give no reassurance to today's players.
Acknowledgments
The authors thank all the personnel of the Rochester Historical Society and Lourdes High School for their help and support.
Statistical analyses were conducted by B. R. Grossardt, MS, Division of Biomedical Statistics and Informatics, Department of Health Sciences Research, College of Medicine, Mayo Clinic, Rochester, MN.
Footnotes
Grant Support: The study was supported by National Institutes of Health Grant R01-AG034676, the Rochester Epidemiology Project (Principal Investigator: Walter A. Rocca, MD, MPH).
Supplemental Online Material
Author Interview Video
References
- 1.Martland H. Punch drunk. JAMA. 1928;91:1103–1107. [Google Scholar]
- 2.Miller H. Mental after-effects of head injury. Proc R Soc Med. 1966;59(3):257–261. doi: 10.1177/003591576605900327. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Gavett B.E., Stern R.A., McKee A.C. Chronic traumatic encephalopathy: a potential late effect of sport-related concussive and subconcussive head trauma. Clin Sports Med. 2011;30(1):179–188. doi: 10.1016/j.csm.2010.09.007. xi. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.McKee A.C., Cantu R.C., Nowinski C.J. Chronic traumatic encephalopathy in athletes: progressive tauopathy after repetitive head injury. J Neuropathol Exp Neurol. 2009;68(7):709–735. doi: 10.1097/NEN.0b013e3181a9d503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Bower J.H., Maraganore D.M., Peterson B.J., McDonnell S.K., Ahlskog J.E., Rocca W.A. Head trauma preceding PD: a case-control study. Neurology. 2003;60(10):1610–1615. doi: 10.1212/01.wnl.0000068008.78394.2c. [DOI] [PubMed] [Google Scholar]
- 6.Mortimer J.A., van Duijn C.M., Chandra V., EURODEM Risk Factors Research Group Head trauma as a risk factor for Alzheimer's disease: a collaborative re-analysis of case-control studies. Int J Epidemiol. 1991;20(suppl 2):S28–S35. doi: 10.1093/ije/20.supplement_2.s28. [DOI] [PubMed] [Google Scholar]
- 7.Chio A., Benzi G., Dossena M., Mutani R., Mora G. Severely increased risk of amyotrophic lateral sclerosis among Italian professional football players. Brain. 2005;128(pt 3):472–476. doi: 10.1093/brain/awh373. [DOI] [PubMed] [Google Scholar]
- 8.Abel E.L. Football increases the risk for Lou Gehrig's disease, amyotrophic lateral sclerosis. Percept Mot Skills. 2007;104(3, pt 2):1251–1254. doi: 10.2466/pms.104.4.1251-1254. [DOI] [PubMed] [Google Scholar]
- 9.Field M., Collins M.W., Lovell M.R., Maroon J. Does age play a role in recovery from sports-related concussion?: A comparison of high school and collegiate athletes. J Pediatr. 2003;142(5):546–553. doi: 10.1067/mpd.2003.190. [DOI] [PubMed] [Google Scholar]
- 10.Melton L.J., III History of the Rochester Epidemiology Project. Mayo Clin Proc. 1996;71(3):266–274. doi: 10.4065/71.3.266. [DOI] [PubMed] [Google Scholar]
- 11.St Sauver J.L., Grossardt B.R., Yawn B.P., Melton L.J., III, Rocca W.A. Use of a medical records linkage system to enumerate a dynamic population over time: the Rochester Epidemiology Project. Am J Epidemiol. 2011;173(9):1059–1068. doi: 10.1093/aje/kwq482. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Bower J.H., Maraganore D.M., McDonnell S.K., Rocca W.A. Incidence and distribution of parkinsonism in Olmsted County, Minnesota, 1976-1990. Neurology. 1999;52(6)):1214–1220. doi: 10.1212/wnl.52.6.1214. [DOI] [PubMed] [Google Scholar]
- 13.Edland S.D., Rocca W.A., Petersen R.C., Cha R.H., Kokmen E. Dementia and Alzheimer disease incidence rates do not vary by sex in Rochester, Minn. Arch Neurol. 2002;59(10):1589–1593. doi: 10.1001/archneur.59.10.1589. [DOI] [PubMed] [Google Scholar]
- 14.Juergens S.M., Kurland L.T., Okazaki H., Mulder D.W. ALS in Rochester, Minnesota, 1925-1977. Neurology. 1980;30(5):463–470. doi: 10.1212/wnl.30.5.463. [DOI] [PubMed] [Google Scholar]
- 15.McKee A.C., Gavett B.E., Stern R.A. TDP-43 proteinopathy and motor neuron disease in chronic traumatic encephalopathy. J Neuropathol Exp Neurol. 2010;69(9):918–929. doi: 10.1097/NEN.0b013e3181ee7d85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Guskiewicz K.M., Marshall S.W., Bailes J. Association between recurrent concussion and late-life cognitive impairment in retired professional football players. Neurosurgery. 2005;57(4):719–726. doi: 10.1093/neurosurgery/57.4.719. discussion 719-726. [DOI] [PubMed] [Google Scholar]
- 17.Goldman S.M., Tanner C.M., Oakes D., Bhudhikanok G.S., Gupta A., Langston J.W. Head injury and Parkinson's disease risk in twins. Ann Neurol. 2006;60(1):65–72. doi: 10.1002/ana.20882. [DOI] [PubMed] [Google Scholar]
- 18.Chen H., Richard M., Sandler D.P., Umbach D.M., Kamel F. Head Injury and amyotrophic lateral sclerosis. Am J Epidemiol. 2007;166(7):810–816. doi: 10.1093/aje/kwm153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Clarke K.S., Powell J.W. Football helmets and neurotrauma—an epidemiological overview of three seasons. Med Sci Sports. 1979;11(2):138–145. [PubMed] [Google Scholar]
- 20.National Football League Properties Inc. Bennett T. Macmillan; New York, NY: 1977. The NFL's Official Encyclopedic History of Professional Football. [Google Scholar]
- 21.Levy M.L., Ozgur B.M., Berry C., Aryan H.E., Apuzzo M.L. Analysis and evolution of head injury in football. Neurosurgery. 2004;55(3):649–655. doi: 10.1227/01.neu.0000134598.06114.89. [DOI] [PubMed] [Google Scholar]
- 22.Levy M.L., Ozgur B.M., Berry C., Aryan H.E., Apuzzo M.L. Birth and evolution of the football helmet. Neurosurgery. 2004;55(3):656–661. doi: 10.1227/01.neu.0000134599.01917.aa. discussion 661-662. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Author Interview Video