

Abstract
INTRODUCTION
Lymphangiomas are benign lesions that are most commonly encountered in the neck of small infants, but are quite uncommon in the adult population. Their removal can be quite difficult, when they reach enormous dimensions or they develop in critical locations. Complete resection is curative, but incomplete resections entail the risk of relapse. Lymphangiomas of the chest wall are quite rare.
PRESENTATION OF CASE
We report a case of a 35-year old man with a giant cavernous lymphangioma of the right lateral chest wall extending into the axilla, which was removed en bloc.
DISCUSSION
These tumors of lymphatic origin tend to grow, as is the case in our patient, but they also tend to recur if not resected completely. Clinical examination and chest CT scan may provide a clue to the diagnosis.
CONCLUSION
Lymphangiomas of the thoracic wall are extremely rare lesions and wide resection is recommended due to the high recurrence rate of these benign lesions.
Keywords: Adult, Chest wall, Lymphangiomatous cysts, Chest wall tumors
1. Introduction
Lymphangiomas are developmental abnormalities of the lymphatic system, known to occur in the neck, but also in the axilla and other sites such as the mediastinum, pelvis and retroperitoneum.1 They most commonly occur in infants.
They are extremely rare in the chest wall.3 They can be of simple capillary, cavernous or cystic type.2 We present a case of a 35-year old man presenting with a huge cavernous lymphangioma of the right lateral chest wall and axilla.
2. Presentation of case
The patient, who was of east Mediterranean origin, presented to the emergency department with a bulging of the right lateral chest wall and right axilla, which had be growing for about two months. He reported no fever. Tuberculin test was negative. There were no other swellings elsewhere. The mass was fluctuant and painful and extended from beneath the pectoralis major m. to beneath the latissimus dorsi m. and from the 6th intercostal space to the apex of the axilla.
Aspiration revealed a dark-colored fluid, which was negative for microorganisms.
The mass was evident on chest X-ray (Fig. 1). CT scan showed a multilocular mass filled with fluid, which was abutting the rib cage, without obviously invading the ribs and extending from beneath the pectoralis major and latissimus dorsi muscles to the apex of the axilla (Fig. 2).
Fig. 1.
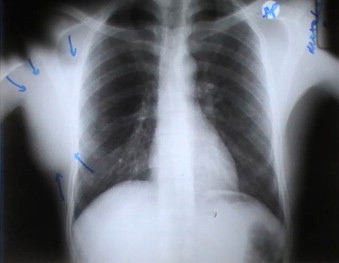
Chest X-ray: a mass is evident in the right chest wall.
Fig. 2.

Chest CT scan: a soft tissue cystic mass is evident in the chest wall.
The patient was scheduled for operation. He was placed in a lateral position, as in the operation for axillary thoracotomy. The incision was centered at the middle of the mass, extending from the lateral border of the pectoralis major m. anterior to the lateral border of the latissimus dorsi posterior. A dark colored cystic mass with thick walls was obvious beneath the subcutaneous tissue (Figs. 3 and 4). The mass extended beneath the pectoralis major almost as far as the sternum and beneath the latissimus dorsi. It invaded muscle slips of the serratus anterior at its lower border and the long thoracic and the nerve to the serratus anterior were displaced on the lateral borders of the mass, without been invaded. Toward the axilla the mass had thin walled and transparent cysts, which were full with a yellowish clear fluid. Blood vessels originating from the axillary vessels, mainly the axillary vein were seen going through the mass. The mass was removed en bloc without scarifying the nerves and by ligating the feeding vessels in the axilla. It was quite easily dissected from the chest wall by a combination of blunt and sharp dissection and the invaded portion of the serratus anterior was also resected with a margin of several centimeters. Closure of the subcutaneous tissue and skin was performed over two suction drains.
Fig. 3.
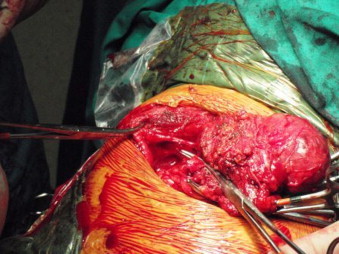
A dark colored mass is evident beneath the subcutaneous tissue.
Fig. 4.

Dissection proceeds.
Postoperative course was uneventful and on routine follow up there was no evidence of wound infection. Final pathology report revealed a cavernous lymphangioma (Fig. 5).
Fig. 5.

Postoperative chest X-ray: the mass has been removed en bloc.
3. Discussion
Cavernous lymphangioma is generally considered a benign mass occurring in the neck of the newborn and small child. 90% appear by the end of the second year of life.4 It is seldom encountered in adult life. Cavernous lymphangioma of the chest wall is rare with only few cases reported.5 These tumors of lymphatic origin tend to grow, as is the case in our patient, but they also tend to recur if not resected completely. That is the reason we performed a radical excision of the mass.
4. Conclusion
Lymphangiomas of the thoracic wall are extremely rare lesions. There is no clue to differentiate lymphangiomas from other chest wall masses, except its soft texture and the rapid rate of growth, but the latter is commonly encountered in some chest wall malignancies as well. CT scan may provide a clue for the correct diagnosis. We recommend that a biopsy should be avoided, when one suspects a chest wall lymphangioma, because it may render a subsequent operation more difficult. It is recommended that a complete resection should be undertaken as soon as the lesion is discovered.
Conflict of interest statement
None.
Funding
None.
Ethical approval
Written consent of the patient has been obtained and we can provide it should the Editor ask for it.
Author contributions
G. Philippakis contributed to the study design, data collection and writing. N. Marinakis contributed to the data collection.
References
- 1.Ravitch M.M., Rush B.F., Jr. Cystic hygroma. In: Welch Ki, Randolph J.G., Ravitch M.M., O’Neill J.A., Jr., Rowe M.I., editors. vol. 1. Year Book Medical Publishers Inc.; Chicago: 1986. p. 536. (Paediatric surgery). [Google Scholar]
- 2.Robbins S.L., Cotran R.S., Kumar V. Blood vessels. In: Robbins S.L., Cotran R.S., Kumar V., editors. Pathologic barir of dir. WB Saunders Co; Philadelphia: 1984. p. 544.http://www.jpgmonline.com/article.asp?issn=0022-3859;year=1995;volume=41;issue=3;spage=89;epage=90;aulast=Kocher-ft2 [Google Scholar]
- 3.Ardenghy M., Miura Y., Kovach R., Hochberg J. Cystic hygroma of the chest wall: a rare condition. Annals of Plastic Surgery. 1996;37(2):211–213. doi: 10.1097/00000637-199608000-00018. [DOI] [PubMed] [Google Scholar]
- 4.Fonnkaisurd E.W. Disorders of the lymphatic system. In: Welch K.J., Randolph J.G., Ravitch M.M., O’Neill J.A. Jr., Rowe M.I., editors. vol. 2. Year Book Medical Publishers Inc.; Chicago: 1986. p. 1506. (Paediatric surgery). [Google Scholar]
- 5.Krainick-Strobel U., Kraimer B., Walz-Mattmuller R. Massive cavernous lymphangioma of the breast and thoracic wall: case report and literature review. Lymphology. 2006;39(September (3)):147–151. [PubMed] [Google Scholar]