

Abstract
AIM: To investigate the short and long-term outcomes of endoscopic balloon dilatation (EBD) for Crohn’s disease (CD) strictures.
METHODS: Between January 1995 and December 2011, 47 EBD procedures were performed in 30 patients (8 females and 22 males) with CD. All patients had strictures through which an endoscope could not pass, and symptoms of these strictures included abdominal pain, abdominal fullness, nausea, and/or vomiting. The 47 strictures included 17 anastomotic and 30 de novo strictures. Endoscopy and dilatation were performed under conscious sedation with intravenous diazepam or flunitrazepam. The dilatations were all performed using through-the-scope balloons with diameters from 8 mm to 20 mm on inflation and lengths of 30-80 mm. Each dilatation session consisted of two to four, 3-min multistep inflations of the balloon, repeated at intervals of 1 wk until adequate dilatation (up to 15-20 mm in diameter) was achieved. The follow-up data were collected from medical records and analyzed retrospectively. Primary success was defined as passage of the scope through the stricture after EBD. Long-term outcomes were analyzed focusing on intervention-free survival and surgery-free survival demonstrated by the Kaplan-Meier method. (Intervention-free meant cases in which neither endoscopic balloon re-dilatation nor surgery was needed after the first dilatation during the observation period). The log rank test was used to evaluate the difference in long-term outcomes between anastomotic and de novo stricture cases.
RESULTS: Primary success was achieved in 44 of the 47 strictures (93.6%). Balloon dilatations failed in 3 cases (6.4%). In 1 case, EBD was a technical failure because the guide-wire could not be passed through the stricture which showed severe adhesion and was a flexural lesion of the intestine. In 2 cases, unexpected perforations occurred immediately after balloon dilatation. Of the 47 treatments, complications occurred in 5 (10.6%). All 5 patients had de novo strictures. One suffered bleeding, two high fever and there were colorectal perforations. One of the patients with a colorectal perforation was treated surgically, the other was managed conservatively. These 2 cases correspond to the two aforementioned EBD failures. Long-term outcomes were evaluated for the 44 successfully-treated strictures after a median follow-up of 26 mo (range, 2-172 mo). During the observation period, re-strictures after EBDs occurred in 26 cases (60.5%). Fourteen of these 26 re-stricture cases underwent EBD again, but in two EBD failed and surgery was ultimately performed in both cases. Twelve of the 26 re-stricture cases were initially treated surgically when the re-strictures occurred. Finally, 30 of the 47 strictures (63.8%) were successfully managed with EBD, allowing surgery to be avoided. Intervention-free survival evaluated by the Kaplan-Meier method was 75% at 12 mo, 58% at 24 mo, and 43% at 36 mo. There was no significant difference between the anastomotic strictures (n = 16) and de novo strictures (n = 28) in the intervention-free survival as evaluated by the log-rank test. Surgery-free survival evaluated by the Kaplan-Meier method was 90% at 12 mo, 75% at 24 mo, and 53% at 36 mo. The 16 anastomotic strictures were associated with significantly better surgery-free survivals than the 28 de novo strictures (log-rank test: P < 0.05).
CONCLUSION: Anastomotic strictures were associated with better long-term outcomes than de novo strictures, indicating that stricture type might be useful for predicting the long-term outcomes of EBD.
Keywords: Crohn’s disease, Endoscopic balloon dilatation, Stricture, Anastomotic, De novo, Outcome
INTRODUCTION
Crohn’s disease (CD) is characterized by chronic or recurrent acute inflammation of the intestinal tract resulting in acute inflammatory changes of the intestinal wall, strictures and/or fistulas. Up to one-third of patients develop a stricture within 10 years after the diagnosis[1-3]. These strictures are mainly treated surgically. It is well known that up to 80% of CD patients will eventually require at least one surgical resection within 10 years of being diagnosed[4,5]. Although surgical resection can relieve the symptoms caused by these strictures, the strictures often recur after resection, sometimes necessitating another surgery and producing short bowel syndrome[6,7]. Therefore, surgical resection must be avoided whenever possible.
In recent years, endoscopic balloon dilatation (EBD) has offered a therapeutic alternative to surgery[8-12]. A recent systematic review estimated immediate success rates to be approximately 86%, and that long-term clinical efficacy was achieved in 58% of patients[9]. EBD has been regarded as a safe and effective procedure in the management of CD strictures. Many previous reports have shown short-term success rates of EBD to generally be high (80%-100%), while the long-term outcomes vary among studies. The factors which affect long-term outcomes of EBD have not been sufficiently clarified. A recent report by Mueller et al[12] showed that long-segment de novo strictures in the terminal ileum had poor long-term responses to EBD, raising the possibility that long-term outcomes of EBD could be affected by the characteristics of strictures. To assess this possibility, we hypothesized that long-term outcomes of EBD might differ between two types of strictures, anastomotic and de novo.
The aim of the present study was to evaluate the short- and long-term outcomes of EBD in our hospital and to compare the long-term outcomes of EBD for these two types of strictures affecting CD patients, anastomotic and de novo strictures.
MATERIALS AND METHODS
Patients
Between January 1995 and December 2011, 47 EBD procedures were performed in 30 patients (8 females and 22 males) with CD. The ages at dilatation ranged from 18 to 72 years (mean age, 32.5 ± 10.5). The average duration of CD was 12.8 (range, 1-35) years. Characteristics of these patients are summarized in Table 1.
Table 1.
Patients characteristics
| Number of patients | n = 30 |
| Number of dilatations | 47 |
| Gender: male/female | 22/8 |
| Age at EBD (mean ± SD), yr | 32.5 ± 10.5 |
| Disease duration (mean ± SD), yr | 12.8 ± 8.0 |
| Median follow-up | 26 mo (range, 2-172 mo) |
| Medical therapy at first dilatation (%) | |
| None | 0 |
| 5-aminosalicylic acid: | 86.7 |
| Steroids: | 13.3 |
| Azathioprine/6-mercaptoprine: | 20.0 |
| Infliximab | 13.3 |
| Elemental diet: | 33.3 |
| Total parental nutrition: | 16.7 |
EBD: Endoscopic balloon dilatation.
All patients had strictures through which an endoscope could not pass, and symptoms of these strictures included abdominal pain, abdominal fullness, nausea, and/or vomiting.
The 47 strictures included 17 anastomotic and 30 de novo strictures. The locations of the anastomotic strictures were 1 at the gastro-jejunal, 5 at the ileo-ileal, 9 at the ileocolonic, and 2 at the ileorectal anastomosis. The locations of de novo strictures were 8 at the pyloric ring of the stomach, 1 in the duodenum, 8 in the ileum or at the ileocaecal valve, 7 in the colon, and 6 in the rectum.
Inclusion and exclusion criteria for EBD
EBD were performed on demand only when the patients presented with obstructive symptoms. Prior to endoscopy, all the patients received radiological assessment to confirm the clinically suspected stricture, to exclude intestinal fistulas and angulated strictures and to measure the length of the strictures. Detailed inclusion criteria for EBD were: (1) clinical symptoms of obstruction (abdominal pain, abdominal fullness, nausea, vomiting); (2) evidence of gut stenosis, detected by radiological examination, through which a standard colonoscope or gastrointestinal scope or enteroscope could not be passed; and (3) no or low inflammatory disease activity.
Exclusion criteria were strictures longer than 3 cm and those complicated by intestinal fistula, active ulceration, or abscess.
Dilatation protocol
Informed consent was obtained from all patients before the dilatation procedure. Endoscopy and dilatation were performed under conscious sedation with intravenous diazepam or flunitrazepam. Dilatation was performed using a standard gastrointestinal scope for 10 upper gastrointestinal strictures, a standard colonoscope for 36 lower gastrointestinal strictures, and an entroscope (double-balloon enteroscopy) for 1 ileo-ileal anstomotic stricture. The dilatations were all performed using through-the-scope balloons (Rigiiflex TTS™, or Controlled Radial Expansion Wireguided Balloon Dilatation Catheter™, Boston Scientific, Boston, MA, United States), with diameters from 8 mm to 20 mm on inflation and lengths of 30-80 mm. The balloon was introduced into the stricture using a guide-wire under radiological control. Each dilatation session consisted of two to four, 3-min multistep inflations of the balloon, repeated at intervals of 1 wk until adequate dilatation (up to 15-20 mm in diameter) was achieved. Passage of the scope through the stricture was attempted in all patients and was used to define primary therapeutic success.
After the successful dilatation, patients were followed in our hospital as out-patients. Repeat dilatations were performed on demand when the patients had obstructive symptoms due to re-strictures confirmed by both radiological assessment and endoscopy.
Statistical analysis
The follow-up data were collected from medical records and analyzed retrospectively.
Primary success was defined as passage of the scope through the stricture after EBD. Long-term outcomes were analyzed focusing on intervention-free survival and surgery-free survival demonstrated by the Kaplan-Meier method. (Intervention-free meant cases in which neither endoscopic balloon re-dilatation nor surgery was needed after the first dilatation during the observation period). The log rank test was used to evaluate the difference in long-term outcomes between anastomotic and de novo stricture cases. A two-sided P value of < 0.05 was considered significant.
RESULTS
Rates of primary success
Primary success was achieved in 44 of the 47 strictures (93.6%). Balloon dilatations failed in 3 cases (6.4%). In 1 case, EBD was a technical failure because the guide-wire could not be passed through the stricture which showed severe adhesion and was a flexural lesion of the intestine. In 2 cases, unexpected perforations occurred immediately after balloon dilatation.
Complications
Of the 47 treatments, complications occurred in 5 (10.6%). All 5 patients had de novo strictures. One suffered bleeding, two high fever and there were colorectal perforations. One of the patients with a colorectal perforation was treated surgically, the other was managed conservatively. These 2 cases correspond to the two aforementioned EBD failures.
Long-term outcomes
An overview of the treatment outcomes for the 47 strictures is shown in Figure 1. Long-term outcomes were evaluated for the 44 successfully-treated strictures after a median follow-up of 26 mo (range, 2-172 mo). During the observation period, re-strictures after EBDs occurred in 26 cases (60.5%). Fourteen of these 26 re-stricture cases underwent EBD again, but in two EBD failed and surgery was ultimately performed in both cases. Twelve of the 26 re-stricture cases were initially treated surgically when the re-strictures occurred. Finally, 30 of the 47 strictures (63.8%) were successfully managed with EBD, allowing surgery to be avoided.
Figure 1.
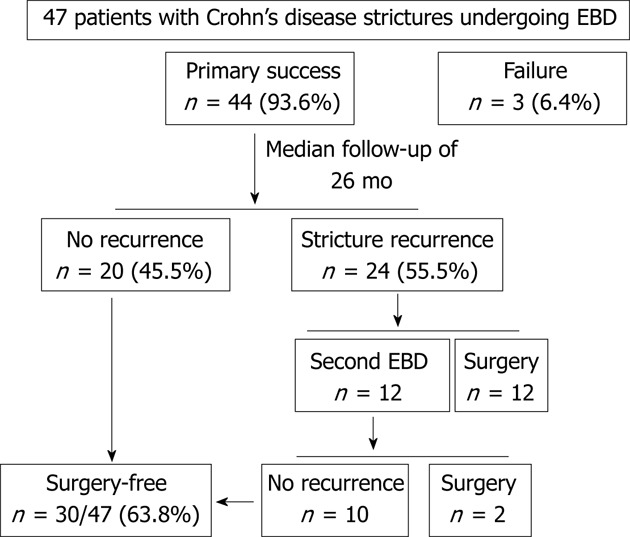
Overview of treatment outcomes for 47 strictures. Long-term outcomes were evaluated for the 44 successfully-treated strictures after a median follow-up of 26 mo (range, 2-172 mo). During the observation period, re-strictures after endoscopic balloon dilatations (EBDs) occurred in 26 cases (60.5%). Fourteen of these 26 re-stricture cases underwent EBD again, but in two EBD failed and surgery was ultimately performed in both cases. Twelve of the 26 re-stricture cases were initially treated surgically when the re-strictures occurred. Finally, 30 of the 47 strictures (63.8%) were successfully managed with EBD, allowing surgery to be avoided.
Intervention-free survival evaluated by the Kaplan-Meier method was 75% at 12 mo, 58% at 24 mo, and 43% at 36 mo (Figure 2). There was no significant difference between the anastomotic strictures (n = 16) and de novo strictures (n = 28) in the intervention-free survival as evaluated by the log-rank test (data not shown).
Figure 2.
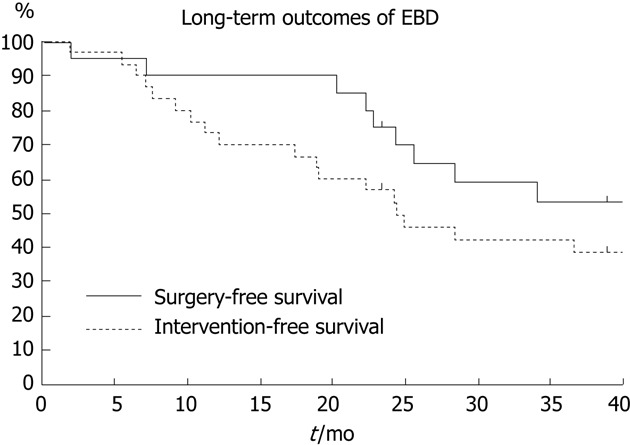
Long-term outcomes of endoscopic balloon dilatation by the Kaplan-Meier method. Intervention-free survival evaluated by the Kaplan-Meier method was 75% at 12 mo, 58% at 24 mo, and 43% at 36 mo. Surgery-free survival evaluated by the Kaplan-Meier method was 90% at 12 mo, 75% at 24 mo, and 53% at 36 mo. EBD: Endoscopic balloon dilatation.
Surgery-free survival evaluated by the Kaplan-Meier method was 90% at 12 mo, 75% at 24 mo, and 53% at 36 mo (Figure 2). The 16 anastomotic strictures were associated with significantly better surgery-free survivals than the 28 de novo strictures (log-rank test: P < 0.05) (Figure 3).
Figure 3.
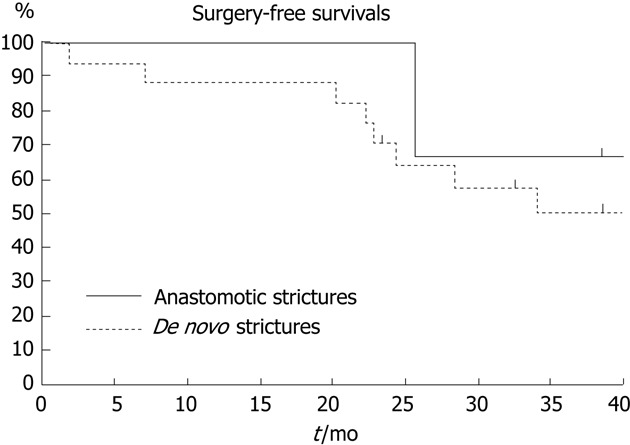
Surgery-free survivals-anastomotic vs de novo strictures. The 16 anastomotic strictures were associated with significantly better surgery-free survivals than the 28 de novo strictures (log-rank test: P < 0.05).
DISCUSSION
EBD has become an alternative to surgery in the treatment of CD strictures in recent years. Many reports have shown good short-term success rates of EBD, while the long-term outcomes have varied among studies. Whether or not the stricture type, such as anastomotic or de novo, impacts long-term outcomes of EBD remains an open question. In this study, we evaluated short- and long-term outcomes of EBD for strictures associated with CD, in our hospital, and analyzed differences in long-term outcomes between anastomotic and de novo strictures.
As for short-term outcomes, primary success was achieved in 44 of the 47 strictures treated. EBD failed in only 3 cases. In 1 case, EBD was technically impossible and in 2 others unexpected perforations occurred immediately after EBD. Therefore, the primary success rate was 93.6% (44/47) in our study. The primary success rate was 86% in a systematic review[9] and 97% in a recent single-center cohort study[13]. Our primary success rate was thus similar to those reported previously. An important issue is the type of stricture, i.e., anastomotic versus de novo. In the aforementioned systematic review[9], 68% of the strictures treated by EBD were located at anastomotic sites, as were 84% of those in the recent single-center cohort study[13]. On the other hand, there were several more de novo (n = 28, 63.6%) than anastomotic strictures (n = 16, 36.4%) in our study. Despite the rather large percentage of de novo strictures, the primary success rate was very high. Mueller et al[12] also reported a primary success rate of 95% despite the majority of their patients presenting with de novo strictures (69%). These findings suggest that short-term outcomes might be not affected by the type of stricture.
In this study, we successfully performed EBD using double-balloon enteroscopy for one patient who had an ileo-ileal anastomtic stricture. In recent years, a few reports described the usefulness and efficacy of EBD for small intestinal strictures in CD patients using double-balloon enteroscopy[11,14]. This procedure may be potentially of significant benefit and should be considered as a useful and effective alternative to surgery. Further investigation should be necessary to confirm the benefit of this procedure.
In this study, 5 patients each experienced one complication (10.6%). All 5 patients had de novo strictures. The de novo strictures thus appeared to be associated with an increased risk of complications as compared with anastomotic strictures. One patient experienced bleeding (2.1%), 2 had high fever (4.3%), and 2 had colorectal perforations (4.3%). The perforation rate in this study was thus very similar to those in the literature[9,11,12,15-21] which have been in the 0%-10% range. We believe that it is important to perform multistep inflation with a gradually increasing diameter under minimal conscious sedation. This technique may have contributed to the low perforation rate in our study. A more aggressive endoscopic technique, general anesthesia, and using excessively large dilatation balloons are considered to be risk factors for perforation[8,22,23].
As for long-term outcomes, re-strictures after the first EBD occurred in 26 cases (60.5%) out of 44 successfully-treated strictures. Re-strictures did not seem to depend on the diameter of the first dilatation because dilatations were evenly achieved up to 15-20 mm in diameter in most of the successfully-treated strictures. Fourteen of these 26 cases were successfully treated with a second EBD during follow-up for re-strictures and surgery was avoided. Ultimately, 14 cases (31.8%) required surgery to treat re-strictures. These results compare favorably with those of the aforementioned systematic review which described 144 of 347 patients (42%) as ultimately needing surgery to treat re-strictures after EBD. In this study, we also estimated intervention-free and surgery-free survivals. Intervention-free survival was 75% at 12 mo, 58% at 24 mo, and 43% at 36 mo. Surgery-free survival was 90% at 12 mo, 75% at 24 mo, and 53% at 36 mo. These results are also similar to those of previous reports[12,13,22].
Little is known about prognostic factors that affect long-term outcomes after EBD. Smoking has been regarded as a prognostic factor increasing the risk of recurrence[20,24]. Hoffmann et al[24] indicated the presence of ulcers in strictures to be associated with poorer long-term outcomes, whereas Thienpont et al[13] reported that there was no association between endoscopic activity, mainly determined by the sizes and number of ulcerations. Thienpont et al[13] also reported that increased levels of C-reactive protein did not influence long-term outcomes. As for the characteristics of strictures, Mueller et al[12] recently described the length and the location of strictures as affecting long-term outcomes. In their report, the patients who required surgery after EBD had longer strictures than those who did not, and all of the surgical patients had de novo strictures in the terminal ileum. In the present comparison of anastomotic and de novo strictures, we found the anastomotic type to be associated with significantly better surgery-free survival rates. Both our results and those of Mueller et al[12] suggested stricture type (anastomotic or de novo) to be useful for predicting long-term outcomes of EBD.
The effects of concurrent or subsequent therapy aimed at increasing the efficacy of EBD remain unclear. Local steroid injection into the strictures after EBD is controversial. Some studies have found this technique to improve outcomes of EBD[17,19,21-23,25,26], and a recent randomized double blind controlled trial showed this technique to effectively reduce both re-dilatation and surgery in pediatric CD patients with strictures[27]. However, opposite results were also obtained in a placebo controlled trial, although the number of patients was limited[28]. Further study is needed to clarify the utility of this technique. Little is known about the efficacy of subsequent administration of medications such as azathioprine or infliximab, and this topic also requires further study.
In summary, we examined short- and long-term effects of EDB for CD strictures. Although the complication rate was relatively low, de novo strictures may carry an increased risk of perforation. Our results also showed anastomotic strictures to be associated with better long-term outcomes than de novo strictures, indicating that stricture type (anastomotic vs de novo) might be useful for predicting the long-term outcomes of EBD.
COMMENTS
Background
In recent years, the efficacy of endoscopic balloon dilatation (EBD) for Crohn’s disease (CD) strictures has been confirmed. Although EBD has been regarded as a safe and effective procedure in the management of CD strictures, the factors which affect long-term outcomes of EBD have not been sufficiently clarified.
Research frontiers
The authors hypothesized that outcomes of EBD might differ between two types of strictures, anastomotic and de novo. In this study, the authors evaluated the short- and long-term outcomes of EBD in the hospital and compared the outcomes of EBD for these two types of strictures affecting CD patients, anastomotic and de novo strictures.
Innovations and breakthroughs
The results showed that patients with anastomotic strictures had better long-term outcomes than those with de novo strictures. This is the first report to clarify that types of the strictures affect the long-term outcomes of EBD in CD patients.
Applications
When considering treatment for CD strictures, this study may indicate that the type of the stricture (anastomotic vs de novo) might be useful for predicting long-term outcomes of EBD.
Peer review
The study reported that EBD might be useful to treat the stricture of CD. The paper also observed the short and long-term outcomes of EBD for two different strictures in CD. The argument of the paper is new.
Footnotes
P- Reviewers Yu CG, Riccioni ME S- Editor Song XX L- Editor A E- Editor Li JY
References
- 1.Cosnes J, Cattan S, Blain A, Beaugerie L, Carbonnel F, Parc R, Gendre JP. Long-term evolution of disease behavior of Crohn’s disease. Inflamm Bowel Dis. 2002;8:244–250. doi: 10.1097/00054725-200207000-00002. [DOI] [PubMed] [Google Scholar]
- 2.Louis E, Collard A, Oger AF, Degroote E, Aboul Nasr El Yafi FA, Belaiche J. Behaviour of Crohn’s disease according to the Vienna classification: changing pattern over the course of the disease. Gut. 2001;49:777–782. doi: 10.1136/gut.49.6.777. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Van Assche G, Geboes K, Rutgeerts P. Medical therapy for Crohn’s disease strictures. Inflamm Bowel Dis. 2004;10:55–60. doi: 10.1097/00054725-200401000-00009. [DOI] [PubMed] [Google Scholar]
- 4.Bernell O, Lapidus A, Hellers G. Risk factors for surgery and postoperative recurrence in Crohn’s disease. Ann Surg. 2000;231:38–45. doi: 10.1097/00000658-200001000-00006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Farmer RG, Whelan G, Fazio VW. Long-term follow-up of patients with Crohn’s disease. Relationship between the clinical pattern and prognosis. Gastroenterology. 1985;88:1818–1825. doi: 10.1016/0016-5085(85)90006-x. [DOI] [PubMed] [Google Scholar]
- 6.Stebbing JF, Jewell DP, Kettlewell MG, Mortensen NJ. Recurrence and reoperation after strictureplasty for obstructive Crohn’s disease: long-term results [corrected] Br J Surg. 1995;82:1471–1474. doi: 10.1002/bjs.1800821108. [DOI] [PubMed] [Google Scholar]
- 7.Rutgeerts P, Geboes K, Vantrappen G, Kerremans R, Coenegrachts JL, Coremans G. Natural history of recurrent Crohn’s disease at the ileocolonic anastomosis after curative surgery. Gut. 1984;25:665–672. doi: 10.1136/gut.25.6.665. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Nomura E, Takagi S, Kikuchi T, Negoro K, Takahashi S, Kinouchi Y, Hiwatashi N, Shimosegawa T. Efficacy and safety of endoscopic balloon dilation for Crohn’s strictures. Dis Colon Rectum. 2006;49:S59–S67. doi: 10.1007/s10350-006-0685-0. [DOI] [PubMed] [Google Scholar]
- 9.Hassan C, Zullo A, De Francesco V, Ierardi E, Giustini M, Pitidis A, Taggi F, Winn S, Morini S. Systematic review: Endoscopic dilatation in Crohn’s disease. Aliment Pharmacol Ther. 2007;26:1457–1464. doi: 10.1111/j.1365-2036.2007.03532.x. [DOI] [PubMed] [Google Scholar]
- 10.Stienecker K, Gleichmann D, Neumayer U, Glaser HJ, Tonus C. Long-term results of endoscopic balloon dilatation of lower gastrointestinal tract strictures in Crohn’s disease: a prospective study. World J Gastroenterol. 2009;15:2623–2627. doi: 10.3748/wjg.15.2623. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Hirai F, Beppu T, Sou S, Seki T, Yao K, Matsui T. Endoscopic balloon dilatation using double-balloon endoscopy is a useful and safe treatment for small intestinal strictures in Crohn’s disease. Dig Endosc. 2010;22:200–204. doi: 10.1111/j.1443-1661.2010.00984.x. [DOI] [PubMed] [Google Scholar]
- 12.Mueller T, Rieder B, Bechtner G, Pfeiffer A. The response of Crohn’s strictures to endoscopic balloon dilation. Aliment Pharmacol Ther. 2010;31:634–639. doi: 10.1111/j.1365-2036.2009.04225.x. [DOI] [PubMed] [Google Scholar]
- 13.Thienpont C, D’Hoore A, Vermeire S, Demedts I, Bisschops R, Coremans G, Rutgeerts P, Van Assche G. Long-term outcome of endoscopic dilatation in patients with Crohn’s disease is not affected by disease activity or medical therapy. Gut. 2010;59:320–324. doi: 10.1136/gut.2009.180182. [DOI] [PubMed] [Google Scholar]
- 14.Despott EJ, Gupta A, Burling D, Tripoli E, Konieczko K, Hart A, Fraser C. Effective dilation of small-bowel strictures by double-balloon enteroscopy in patients with symptomatic Crohn’s disease (with video) Gastrointest Endosc. 2009;70:1030–1036. doi: 10.1016/j.gie.2009.05.005. [DOI] [PubMed] [Google Scholar]
- 15.Blomberg B, Rolny P, Järnerot G. Endoscopic treatment of anastomotic strictures in Crohn’s disease. Endoscopy. 1991;23:195–198. doi: 10.1055/s-2007-1010654. [DOI] [PubMed] [Google Scholar]
- 16.Junge U, Züchner H. [Endoscopic balloon dilatation of symptomatic strictures in Crohn’s disease] Dtsch Med Wochenschr. 1994;119:1377–1382. doi: 10.1055/s-2008-1058848. [DOI] [PubMed] [Google Scholar]
- 17.Ramboer C, Verhamme M, Dhondt E, Huys S, Van Eygen K, Vermeire L. Endoscopic treatment of stenosis in recurrent Crohn’s disease with balloon dilation combined with local corticosteroid injection. Gastrointest Endosc. 1995;42:252–255. doi: 10.1016/s0016-5107(95)70101-x. [DOI] [PubMed] [Google Scholar]
- 18.Dear KL, Hunter JO. Colonoscopic hydrostatic balloon dilatation of Crohn’s strictures. J Clin Gastroenterol. 2001;33:315–318. doi: 10.1097/00004836-200110000-00012. [DOI] [PubMed] [Google Scholar]
- 19.Thomas-Gibson S, Brooker JC, Hayward CM, Shah SG, Williams CB, Saunders BP. Colonoscopic balloon dilation of Crohn’s strictures: a review of long-term outcomes. Eur J Gastroenterol Hepatol. 2003;15:485–488. doi: 10.1097/01.meg.0000059110.41030.bc. [DOI] [PubMed] [Google Scholar]
- 20.Sabaté JM, Villarejo J, Bouhnik Y, Allez M, Gornet JM, Vahedi K, Modigliani R, Lémann M. Hydrostatic balloon dilatation of Crohn’s strictures. Aliment Pharmacol Ther. 2003;18:409–413. doi: 10.1046/j.1365-2036.2003.01715.x. [DOI] [PubMed] [Google Scholar]
- 21.Ferlitsch A, Reinisch W, Püspök A, Dejaco C, Schillinger M, Schöfl R, Pötzi R, Gangl A, Vogelsang H. Safety and efficacy of endoscopic balloon dilation for treatment of Crohn’s disease strictures. Endoscopy. 2006;38:483–487. doi: 10.1055/s-2006-924999. [DOI] [PubMed] [Google Scholar]
- 22.Couckuyt H, Gevers AM, Coremans G, Hiele M, Rutgeerts P. Efficacy and safety of hydrostatic balloon dilatation of ileocolonic Crohn’s strictures: a prospective longterm analysis. Gut. 1995;36:577–580. doi: 10.1136/gut.36.4.577. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Singh VV, Draganov P, Valentine J. Efficacy and safety of endoscopic balloon dilation of symptomatic upper and lower gastrointestinal Crohn’s disease strictures. J Clin Gastroenterol. 2005;39:284–290. doi: 10.1097/01.mcg.0000155128.31208.44. [DOI] [PubMed] [Google Scholar]
- 24.Hoffmann JC, Heller F, Faiss S, von Lampe B, Kroesen AJ, Wahnschaffe U, Schulzke JD, Zeitz M, Bojarski C. Through the endoscope balloon dilation of ileocolonic strictures: prognostic factors, complications, and effectiveness. Int J Colorectal Dis. 2008;23:689–696. doi: 10.1007/s00384-008-0461-9. [DOI] [PubMed] [Google Scholar]
- 25.Matsui T, Hatakeyama S, Ikeda K, Yao T, Takenaka K, Sakurai T. Long-term outcome of endoscopic balloon dilation in obstructive gastroduodenal Crohn’s disease. Endoscopy. 1997;29:640–645. doi: 10.1055/s-2007-1004271. [DOI] [PubMed] [Google Scholar]
- 26.Brooker JC, Beckett CG, Saunders BP, Benson MJ. Long-acting steroid injection after endoscopic dilation of anastomotic Crohn’s strictures may improve the outcome: a retrospective case series. Endoscopy. 2003;35:333–337. doi: 10.1055/s-2003-38145. [DOI] [PubMed] [Google Scholar]
- 27.Di Nardo G, Oliva S, Passariello M, Pallotta N, Civitelli F, Frediani S, Gualdi G, Gandullia P, Mallardo S, Cucchiara S. Intralesional steroid injection after endoscopic balloon dilation in pediatric Crohn’s disease with stricture: a prospective, randomized, double-blind, controlled trial. Gastrointest Endosc. 2010;72:1201–1208. doi: 10.1016/j.gie.2010.08.003. [DOI] [PubMed] [Google Scholar]
- 28.East JE, Brooker JC, Rutter MD, Saunders BP. A pilot study of intrastricture steroid versus placebo injection after balloon dilatation of Crohn’s strictures. Clin Gastroenterol Hepatol. 2007;5:1065–1069. doi: 10.1016/j.cgh.2007.04.013. [DOI] [PubMed] [Google Scholar]