

Abstract
Purpose
This study aimed to evaluate the prevalence and the effects of unmet needs on quality of life (QOL) among recurrent breast cancer survivors.
Methods
Completed questionnaires were collected from 52 women with recurrent breast cancer. Clinical and socio-demographic characteristics were reviewed, and the Supportive Care Needs Survey, Functional Assessment of Cancer Therapy-Breast Cancer Instrument, and Beck Depression Inventory (BDI) were administered. The frequency of unmet needs and the mean differences by patient characteristics and BDI scores were analyzed. The predictive value of unmet needs on QOL, controlling for socio-demographic variables and then for clinical variables, was analyzed in hierarchical regression models.
Results
The most common unmet needs belonged to the health system and information domain. The depressive group had greater unmet needs in the psychological domain (p<0.001), physical and daily living domain (p=0.001), and health and information domain (p=0.002). Patients with lower education attainment and those with lower performance status had greater unmet needs in the psychological needs (p=0.002) and in the physical and daily living needs domain (p=0.002), respectively. Unmet needs in the psychological domain (p=0.008), physical and daily living domain (p=0.022), and sexuality domain (p=0.040) strongly predicted QOL of women with recurrent breast cancer.
Conclusion
Unmet needs were strong predictors for QOL among recurrent breast cancer patients. This suggests that QOL of women with recurrent breast cancer is possibly more affected by unmet needs than by patient's socio-demographic or clinical characteristics. Intervention strategies could be developed based on the identified needs of women with recurrent breast cancer in order to improve their QOL. Further longitudinal and prospective studies will be necessary to confirm the independent impact of unmet needs on QOL.
Keywords: Breast carcinoma, Quality of life, Recurrence, Unmet needs
INTRODUCTION
The risk of cancer recurrence is an ongoing and significant issue for breast cancer survivors [1,2]. Although early detection and advances in treatment have improved disease-free survival rates of women diagnosed with breast cancer, a substantial proportion still experience recurrence or are diagnosed with a new primary breast cancer [2].
It has been reported that women experience recurrence as a time of increased psychological distress and threat [3]. Previous studies showed psychosocial adaptation experienced by recurrent breast cancer patients were poorer than that experienced by patients with an initial diagnosis of breast cancer [4-9]. Cancer patients with advanced or recurrent disease are reported to be more depressed and experience worse quality of life (QOL) than patients with early disease [4,5].
Psychosocial adaptation to cancer has been evaluated using a variety of constructs including QOL, satisfaction with care, and needs assessment [10]. Needs assessment identifies specific issues that patients need help with and directly assesses the perceived urgency of the need for help, which enables focused care on the issues patients themselves have identified as ones that require most help [11]. Identifying and addressing the unmet needs of patients are important because they are found to be significantly associated with both psychological distress and poor QOL [4-6], which may in turn negatively affect the health care system by increasing health care utilization and costs [12-15].
Although the QOL of breast cancer patients is well documented, few studies have assessed unmet needs and their role in QOL among women with recurrent breast cancer. A few factors have been identified as predictors of overall quality of life among women with recurrent breast cancer, including age, time since recurrence, recurrence pattern (local-regional or distant recurrence), sites of metastasis, current physical symptoms, and treatment status [16-18]. Unmet needs were reported to be associated with QOL in breast cancer patients [13,15,19,20]. However, to our knowledge, no study has investigated the predictive value of unmet needs on QOL among recurrent breast cancer patients.
The specific aims of the current study were to examine the unmet needs and depression among patients with recurrent breast cancer and to explore the predictive value of unmet needs on QOL along with socio-demographic and clinical variables.
METHODS
Patients
The subjects in this study were a consecutive sample of 55 outpatients diagnosed with recurrent breast cancer at Severance Hospital Breast Cancer Clinic, Seoul, Korea. The eligibility criteria for inclusion in the study were as follows: 1) a diagnosis of recurrence of breast cancer, 2) aged between 20 and 80 years old, and 3) no evidence of psychosis, dementia, or suicidal behavior. After informed consent had been obtained, the patients were asked to complete the questionnaires. Among the 55 eligible patients, 53 consented to participate in the study and 52 returned the completed surveys. A total of 52 cases were used in the analysis. Data were collected from January 2007 until October 2008. This study was approved by the Institutional Review Board of Severance Hospital (4-2009-0269).
Measurements
Socio-demographic and medical background
Socio-demographic background including patient's age, marital status, job, education, and economic status were included in the survey. Medical/treatment variables were collected by reviewing the patients' medical records. Performance status was evaluated by the Eastern Cooperative Oncology Group Performance Status (ECOG-PS) scale. ECOG-PS assesses the level of functioning based on activity, ambulatory status, and the need for care ranging from grade 0 (normal activity) to grade 4 (completely bedridden). ECOG-PS is widely used and well validated [21].
The Supportive Care Needs Survey (SCNS)
The unmet needs of recurrent breast cancer patients were assessed by the SCNS, which was designed to provide direct assessment of cancer patients' perceived needs for help and to identify the magnitude of the need for help [10]. The survey contains 59 items covering five domains of needs and other additional items as follows: psychological (22 items), health system and information (15 items), physical and daily living (7 items), patient care and support (8 items), sexuality (3 items), and additional 4 items. The participants were asked to indicate the level of their need for help over the last month in relation to having cancer ranging from 1, no need (not applicable); 2, no need (satisfied); 3, low need; 4, moderate need; to 5, high need. Subscale scores were calculated by summing the responses to each of the items of need and dividing the total by the number of items in the domain. A higher score indicated a higher perceived need. The survey's psychometric properties have been well documented [10]. We used the SCNS-LF59 survey in Korean language, which had been translated and back-translated by Hwang and Park [22]. The reliability coefficient was 0.964 in the psychological needs domain, 0.905 in the physical and daily activity domain, 0.927 in the sexuality domain, 0.947 in the health system and information domain, and 0.916 in the patient care and support domain.
The Beck Depression Inventory (BDI)
The BDI is one of the most commonly used self-report depression symptom questionnaires in the medical field. BDI is a 21-item inventory used to describe symptoms and attitudes. Each item describes a particular aspect of depression and has four self-evaluative statements. The study participants were asked to circle the items that best describe how they have been feeling in the last week. The Korean version of the BDI was standardized [23] and its validity and reliability have been established [24]. The reliability coefficient for BDI was 0.873 in this study.
Functional Assessment of Cancer Therapy-Breast (FACT-B)
The FACT-B version 4 was used to assess health-related QOL. The FACT-B is a 36-item questionnaire composed of the FACT-General (27 items) and the breast cancer subscale (9 items). FACT-B consists of the following subscales: physical well-being, emotional well-being, social/family wellbeing, and breast cancer subscale. A total FACT-B score is calculated by summing the subscales. The participants were asked to rate how true each statement was for the period of last 7 days, using a scale from 0 to 4. The psychometric properties of the FACT-B are well documented [25], and the survey was validated in Korea [26]. The α coefficient for the FACT-B total score was 0.713 in this study.
Statistical analysis
Descriptive statistics were used to analyze the socio-demographic and clinical characteristics of the sample. The frequency of each response option of the 59 items was generated and the 20 items with the highest frequency of moderate to high needs were ranked. Differences of unmet needs between two groups, depressive group vs. non-depressive group, by the BDI cutoff score were examined with the t-test. Hierarchical multiple regression models were employed to identify significant predictors of QOL. Independent variables were separated into 3 hierarchical blocks. Socio-demographic characteristics (age at recurrence, education, financial status, marital status) were entered in the first block (Model A) and then clinical characteristics (time since recurrence, performance status, recurrence pattern) were entered in the second block (Model B) because they are more stable characteristics that are less subjected to errors. Five domains of SCNS (psychological, physical and daily living, sexuality, health system, and information domain) were entered in the last block (Model C) to examine the predictive value of unmet needs after controlling for socio-demographic and clinical characteristics. Prior to analyzing the regression models using these predictor variables, tests were conducted to ensure that the inclusion of all the above-mentioned variables did not introduce statistically significant multicollinearity. Data analyses were conducted using the SPSS software version 17.0 (SPSS Inc., Chicago, USA). A p-value less than 0.05 was considered statistically significant.
RESULTS
Patient characteristics
The demographic and clinical characteristics of 52 study participants are displayed in Table 1. The mean age of the study participants was 48.34±8.28 years, 86.5% were married, and 11 (21.2%) were educated under high school level. Most women (82.7%) were unemployed at the time of survey and 71.2% reported their economic status as middle. The mean time since recurrence was 20.26±22.19 months. Most women were amenorrheic (84.6%) and almost fully ambulatory in the performance status (90.4%). In terms of recurrence pattern, 32.7% of women were local-regional and 67.3% were either systemic or both systemic and local. Among the patients with systemic recurrence, 51.4% were bone and soft tissue metastases.
Table 1.
Socio-demographic and clinical characteristics
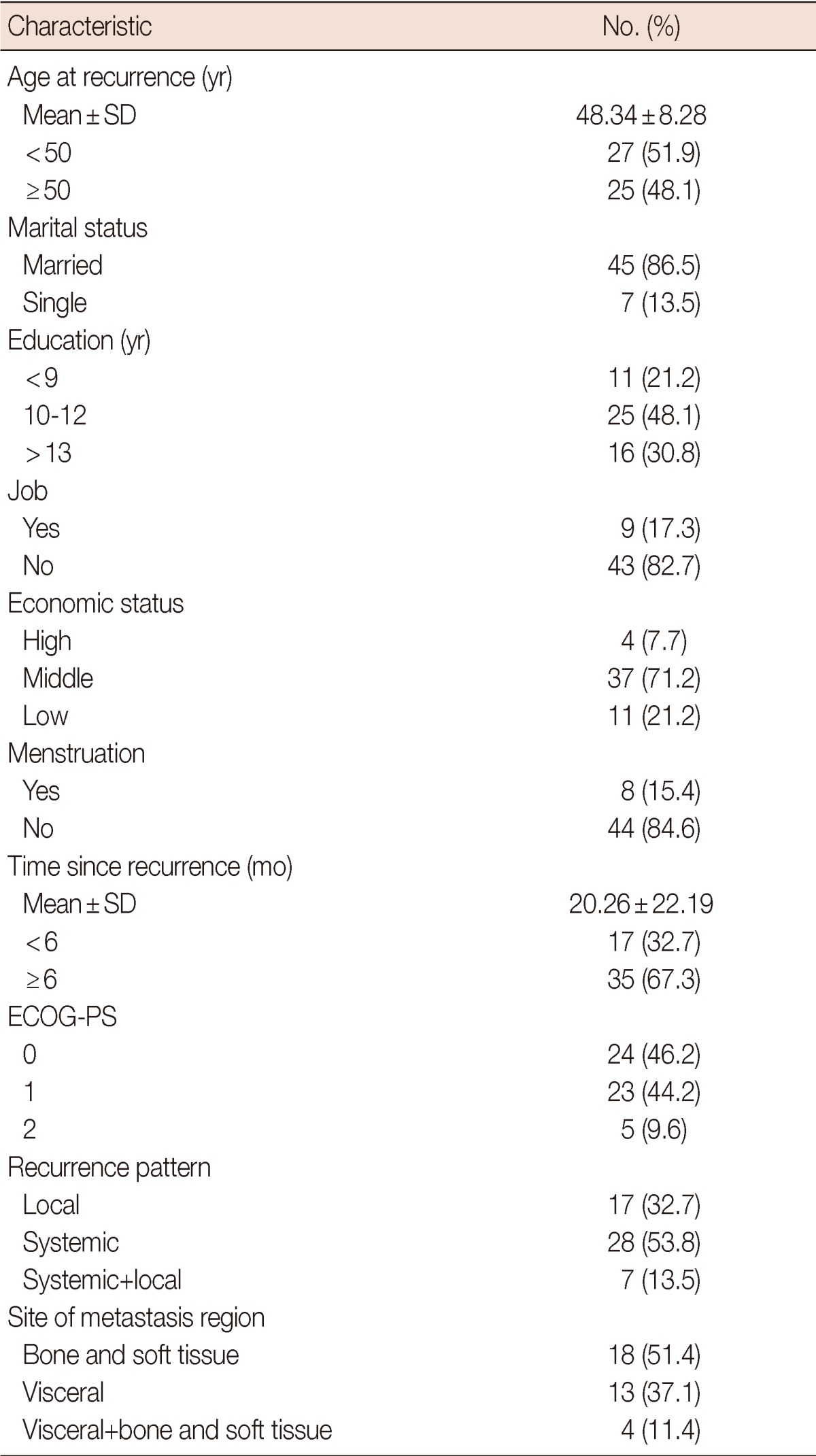
ECOG-PS=the Eastern Cooperative Oncology Group Performance Scale.
Prevalence of unmet needs
The top 20 unmet needs that were rated as moderate to high are shown in Table 2. Among the 20 highest needs items, 13 items were in the health system and information domain, 3 in the psychological domain and 4 were in the patient care and support domain. The most common unmet needs were 'Being informed about cancer which is under control or diminishing' (50.3%) followed by 'To be informed about things you can do to help yourself get well' (47.6%), 'Waiting a long time for clinic appointments' (43.7%), 'To be informed about your test results as soon as possible' (42.5%), and 'To have one member of hospital staff with whom you can talk to about all aspects of your condition, treatment and follow-up' (41.8%).
Table 2.
Top 20 unmet needs by percentage rating with moderate or high need

Unmet needs by patient characteristics
Table 3 shows the mean differences of SCNS subscales by patient characteristics. In the psychological needs domain, patients with a lower level of education were more likely to report significantly higher unmet needs (p=0.003). Economic status was marginally significant (p=0.072). In the physical and daily living needs domain, patients with a lower performance status (p=0.002) were more likely to have higher unmet needs; marital status (p=0.076) was marginally significant. In the sexuality needs domain, no significant factor was found, except economic status (p=0.053) and education (p=0.077) which were marginally significant. In the health system and information needs domain and the patient care and support needs domain, there were no mean differences of SCNS subscales by patient characteristics.
Table 3.
The mean scores of SCNS subscales by patient characteristics

SCNS=the Supportive Cancer Needs Survey; ECOG-PS=the Eastern Cooperative Oncology Group Performance Scale.
Differences of unmet needs between depressive vs. non-depressive recurrent breast patients
The mean scores of unmet needs between the depressive group and the non-depressive group are compared in Table 4. A cutoff score of 21 was used to divide the two groups for this analysis, which was suggested as suitable to distinguish between those having depressive symptoms from those not having such symptoms in Korea, since Korean patients tend to report their symptoms higher than what they actually experience [24].
Table 4.
Unmet needs differences by BDI cutoff score

BDI=Beck Depression Inventory.
Twenty-five percent of the participants were depressive (BDI score ≥21). Patients in the depressive group exhibited a significantly higher level of unmet needs in the psychological domain (p<0.001), physical and daily living domain (p=0.001) and health system and information domain (p=0.002) than those in the non-depressive group (BDI score <21).
Predictors of QOL in a hierarchical multivariate framework
The mean scores of FACT-B are presented in Table 5. The mean total score of FACT-B was 90.44±20.33. Table 6 displays the standardized regression coefficients and p-values for the hierarchical multivariate regression analyses. Firstly, univariate analyses were performed for socio-demographic characteristics including age at first diagnosis, age at recurrence, marital status, education, job, economic status and clinical variables including menstruation, time since first diagnosis, time since recurrence, performance status, chemotherapy, and recurrence pattern (data not shown). We only included variables in the multiple regression models which were determined as significant according to univariate analysis or were reported as strong predictors for QOL of recurrent breast cancer patients in previous studies [2,8,16-18]. Therefore, age at recurrence, education, financial status and marital status among the socio-demographic characteristics were entered in the first block, and time since recurrence, performance status and recurrence pattern among clinical variables were entered in the second block. In model A (R2=0.216), in which socio-demographic variables were entered, higher level of education (>13 years) was a significant predictor for better QOL among women with recurrent breast cancer (p=0.023). However, it did not remain significant once clinical variables were entered in model B (R2=0.363). There was no significant clinical predictor in model B, although performance status was marginally significant (p=0.078). In the final equation (model C, R2=0.635), the psychological needs, physical and daily living needs and sexuality needs were identified as strong predictors of quality of life. Having a higher level of unmet needs in the psychological needs domain (p=0.008) and in the physical and daily living needs domain (p=0.022), and a lower level of unmet needs in the sexuality domain (p=0.040) were significantly associated with poorer quality of life. Older age (≥50 years at recurrence [p=0.054]) was the only variable that was marginally associated with better quality of life among all the socio-demographic and clinical variables in the final model. The final model accounted for 63.5% of the variance.
Table 5.
The mean scores of FACT-B
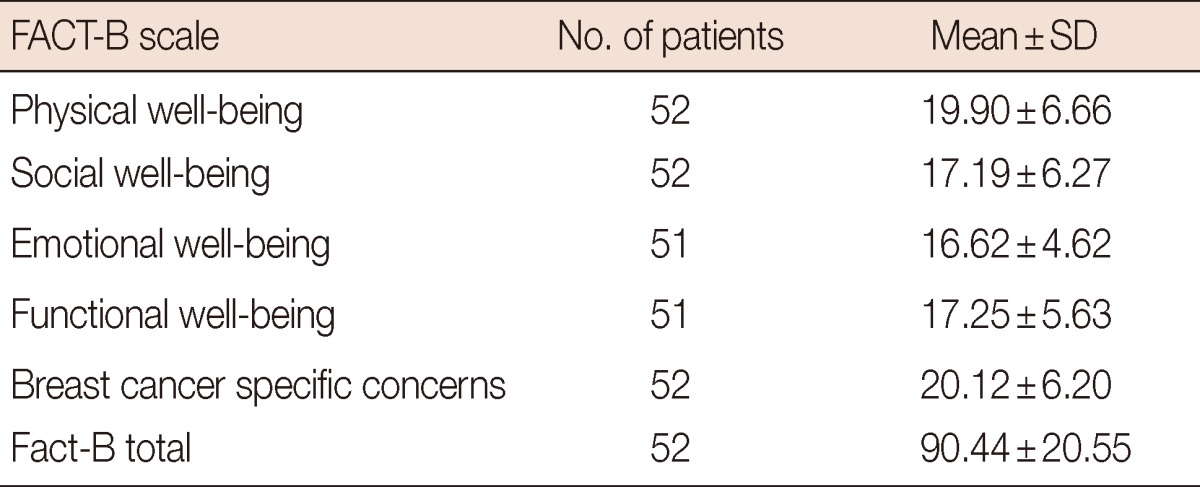
FACT-B=Functional Assessment of Cancer Therapy-Breast.
Table 6.
The hierarchical regression models predicting QOL

QOL=quality of life; ECOG-PS=the Eastern Cooperative Oncology Group Performance Scale.
DISCUSSION
The present findings indicated that unmet needs including the psychological, the physical and daily living, and the sexuality needs were strong predictors for QOL of recurrent breast cancer patients. Most of the common unmet need items belonged to the health system and information needs domain. In addition, depressive patients reported a significantly greater level of unmet needs in the psychological, the physical and daily living domain, and in the health system and information domain.
In terms of unmet needs, the highest frequencies of unmeet needs were from the health system and the information domain, which is consistent with previous studies for survivors of breast cancer [15,19,27]. Among previous Asian studies, our results are similar to the results of study involving a population of Hong Kong Chinese patients [15], which also showed that 9 out of 10 highest unmet needs belonged to the health and information domain. On the contrary, a Japanese study with advanced breast cancer patients showed a much higher prevalence of moderate to high unmet needs from 59.4% to 78.8% [20], compared with that from 29.6% to 50.3% in the present study. Also, patients in the Japanese study considered psychological unmet needs (8 out of 10 highest unmet needs) as their utmost priority, while the health system and information needs were prioritized the most in the present study (8 out of 10 highest unmet needs). This indicates that differences exist even among Asian countries as well as between Caucasian and Asian countries. It is interesting to note that the prevalence of unmet needs in the present study was almost no different from a previous study of early breast cancer patients in Korea [19], except that 2 psychological unmet needs ('Fears about cancer spreading', 'Fears about cancer returning') were ranked as 10th and 11th respectively in the present study. This might suggest that health system and information needs are the most highly perceived needs for both early and recurrent breast cancer patients. Since various patient education programs are regularly provided and booklets or cyber information is so easily accessible these days, new strategies must be developed in terms of the level of detail, the timing of presentation, and the medium in which information is presented [27], in addition to the quantity of information. Satisfaction with care could be significantly improved if preferences of patients regarding provision of information are considered.
The percentage of depression (≥21 on BDI score) observed in our study participants (25%) was higher than that of a previous study involving early breast cancer patients in Korea (20.4%) [28], which is consistent with other research [6,7]. The depressive group expressed a significantly greater level of the psychological, the physical and daily living, and the health system and information needs, which confirms the results of other research which showed that depression was associated with a higher level of unmet needs [27]. Also, recurrent breast cancer patients were still struggling with fears about cancer spreading and recurrence. This might suggest that the threat of another recurrence is an ongoing and significant issue for recurrent breast cancer survivors as well as for primary cancer patients. Further research with randomized samples is needed to confirm the differences of unmet needs and depression between early and recurrent breast cancer patients.
Overall QOL in the present participants measured by FACT-B (90.44±20.55) was much lower than those in other studies with recurrent [29] and primary breast cancer patients [30], which were evaluated by the same measure. This confirms that QOL experienced by recurrent breast cancer patients was worse than that experienced by patients with an initial diagnosis [4,16]. However, this needs a further study because the statistical significance could not be examined among these results.
Interestingly, there was no significant predictor for QOL among the demographic and clinical characteristics in the final regression model, which supports a previous study with metastatic breast cancer [27]. Only older age was marginally associated with better QOL in the present study. This may result from older patients being more emotionally mature and having more resources and support, and are therefore coping better with recurrence. Although significant improvement of QOL at 6 months after recurrence [17] and a significant association between local recurrence and QOL were suggested previously [2,17], the present study was not consistent with such findings. The association between local recurrence and QOL has been somewhat contradictory. In one study, local recurrence was associated with poorer QOL [17], whereas it was associated with better QOL in another study [2]. Patients in our study may have perceived recurrence as equally overwhelming irrespective of their clinical characteristics, and therefore unmet needs rather than clinical differences were considered more important in perceived QOL.
Another interesting result in this study was the association between greater sexuality needs and better QOL. Prior studies noted that Asian women report significantly lower sexuality needs than Caucasian women [12,15,19] and showed significant association between higher education attainment and higher unmet needs scores in the sexuality domain [15]. Taking into account that Asian women are more reluctant to talk about their sexual needs, it is plausible that those who express their sexual needs directly might have better functioning and better QOL than those who do not. Patients who suffer more serious difficulties might consider sexual needs as relatively less important than other needs, which might result in a significant association between greater sexuality needs and better QOL. This needs further examination in a future study.
Even though this study provides important information of unmet needs and QOL among recurrent breast cancer patients, it has some limitations including the cross-sectional design, sample bias, and the small sample size. As we used the cross-sectional design, inferences about causality could not be made based on this study. Furthermore, because the sample was accrued from outpatients, the unmet needs of recurrent breast cancer patients with severe physical impairment might not have been reflected in the study results. Thus, the present findings cannot be generalized to all recurrent breast cancer patients. Further studies should be undertaken to confirm the present findings.
In the present study, the unmet needs of recurrent breast cancer patients were determined as strong predictors for their QOL. This suggests the importance of identifying the specific needs of women with breast cancer in order to improve their QOL. If future studies can confirm the predictive value of unmet needs on QOL among recurrent breast cancer patients, direct assessment of unmet needs may become an effective means to improve QOL and reduce utilization and costs of the health care system.
Footnotes
The authors declare that they have no competing interests.
References
- 1.Gotay CC. The experience of cancer during early and advanced stages: the views of patients and their mates. Soc Sci Med. 1984;18:605–613. doi: 10.1016/0277-9536(84)90076-5. [DOI] [PubMed] [Google Scholar]
- 2.Thornton AA, Madlensky L, Flatt SW, Kaplan RM, Pierce JP. The impact of a second breast cancer diagnosis on health related quality of life. Breast Cancer Res Treat. 2005;92:25–33. doi: 10.1007/s10549-005-1411-7. [DOI] [PubMed] [Google Scholar]
- 3.Jenkins PL, May VE, Hughes LE. Psychological morbidity associated with local recurrence of breast cancer. Int J Psychiatry Med. 1991;21:149–155. doi: 10.2190/UU5G-MDJ3-U55G-33GQ. [DOI] [PubMed] [Google Scholar]
- 4.Siddiqi A, Given CW, Given B, Sikorskii A. Quality of life among patients with primary, metastatic and recurrent cancer. Eur J Cancer Care (Engl) 2009;18:84–96. doi: 10.1111/j.1365-2354.2008.01021.x. [DOI] [PubMed] [Google Scholar]
- 5.Simon AE, Thompson MR, Flashman K, Wardle J. Disease stage and psychosocial outcomes in colorectal cancer. Colorectal Dis. 2009;11:19–25. doi: 10.1111/j.1463-1318.2008.01501.x. [DOI] [PubMed] [Google Scholar]
- 6.Cella DF, Mahon SM, Donovan MI. Cancer recurrence as a traumatic event. Behav Med. 1990;16:15–22. doi: 10.1080/08964289.1990.9934587. [DOI] [PubMed] [Google Scholar]
- 7.Fulton C. The prevalence and detection of psychiatric morbidity in patients with metastatic breast cancer. Eur J Cancer Care (Engl) 1998;7:232–239. doi: 10.1046/j.1365-2354.1998.00107.x. [DOI] [PubMed] [Google Scholar]
- 8.Northouse LL, Dorris G, Charron-Moore C. Factors affecting couples' adjustment to recurrent breast cancer. Soc Sci Med. 1995;41:69–76. doi: 10.1016/0277-9536(94)00302-a. [DOI] [PubMed] [Google Scholar]
- 9.Burgess C, Cornelius V, Love S, Graham J, Richards M, Ramirez A. Depression and anxiety in women with early breast cancer: five year observational cohort study. BMJ. 2005;330:702. doi: 10.1136/bmj.38343.670868.D3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Bonevski B, Sanson-Fisher R, Girgis A, Burton L, Cook P, Boyes A Supportive Care Review Group. Evaluation of an instrument to assess the needs of patients with cancer. Cancer. 2000;88:217–225. doi: 10.1002/(sici)1097-0142(20000101)88:1<217::aid-cncr29>3.0.co;2-y. [DOI] [PubMed] [Google Scholar]
- 11.McElduff P, Boyes A, Zucca A, Girgis A. Supportive Care Needs Survey: a Guide to Administration, Scoring and Analysis. Newcastle: Centre for Health Research and Psycho-oncology; 2004. p. 4. [Google Scholar]
- 12.Akechi T, Okuyama T, Endo C, Sagawa R, Uchida M, Nakaguchi T, et al. Patient's perceived need and psychological distress and/or quality of life in ambulatory breast cancer patients in Japan. Psychooncology. 2011;20:497–505. doi: 10.1002/pon.1757. [DOI] [PubMed] [Google Scholar]
- 13.Shim EJ, Mehnert A, Koyama A, Cho SJ, Inui H, Paik NS, et al. Health-related quality of life in breast cancer: a cross-cultural survey of German, Japanese, and South Korean patients. Breast Cancer Res Treat. 2006;99:341–350. doi: 10.1007/s10549-006-9216-x. [DOI] [PubMed] [Google Scholar]
- 14.Sanson-Fisher R, Girgis A, Boyes A, Bonevski B, Burton L, Cook P Supportive Care Review Group. The unmet supportive care needs of patients with cancer. Cancer. 2000;88:226–237. doi: 10.1002/(sici)1097-0142(20000101)88:1<226::aid-cncr30>3.3.co;2-g. [DOI] [PubMed] [Google Scholar]
- 15.Lam WW, Au AH, Wong JH, Lehmann C, Koch U, Fielding R, et al. Unmet supportive care needs: a cross-cultural comparison between Hong Kong Chinese and German Caucasian women with breast cancer. Breast Cancer Res Treat. 2011;130:531–541. doi: 10.1007/s10549-011-1592-1. [DOI] [PubMed] [Google Scholar]
- 16.Hanson Frost M, Suman VJ, Rummans TA, Dose AM, Taylor M, Novotny P, et al. Physical, psychological and social well-being of women with breast cancer: the influence of disease phase. Psychooncology. 2000;9:221–231. doi: 10.1002/1099-1611(200005/06)9:3<221::aid-pon456>3.0.co;2-t. [DOI] [PubMed] [Google Scholar]
- 17.Bull AA, Meyerowitz BE, Hart S, Mosconi P, Apolone G, Liberati A. Quality of life in women with recurrent breast cancer. Breast Cancer Res Treat. 1999;54:47–57. doi: 10.1023/a:1006172024218. [DOI] [PubMed] [Google Scholar]
- 18.Lee MK, Son BH, Hwang SY, Han W, Yang JH, Lee S, et al. Factors affecting health-related quality of life in women with recurrent breast cancer in Korea. Qual Life Res. 2007;16:559–569. doi: 10.1007/s11136-006-9144-6. [DOI] [PubMed] [Google Scholar]
- 19.Park BW, Hwang SY. Unmet needs of breast cancer patients relative to survival duration. Yonsei Med J. 2012;53:118–125. doi: 10.3349/ymj.2012.53.1.118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Uchida M, Akechi T, Okuyama T, Sagawa R, Nakaguchi T, Endo C, et al. Patients' supportive care needs and psychological distress in advanced breast cancer patients in Japan. Jpn J Clin Oncol. 2011;41:530–536. doi: 10.1093/jjco/hyq230. [DOI] [PubMed] [Google Scholar]
- 21.Sorensen JB, Klee M, Palshof T, Hansen HH. Performance status assessment in cancer patients. An inter-observer variability study. Br J Cancer. 1993;67:773–775. doi: 10.1038/bjc.1993.140. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Hwang SY, Park BW. The perceived care needs of breast cancer patients in Korea. Yonsei Med J. 2006;47:524–533. doi: 10.3349/ymj.2006.47.4.524. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Hahn HM, Yum TH, Shin YW, Kim KH, Yoon DJ, Chung KJ. A standardization study of Beck Depression Inventory in Korea. J Korean Neuropsychiatr Assoc. 1986;25:487–502. [Google Scholar]
- 24.Lee YH, Song JY. A study of the reliability and the validity of the BDI , SDS, and MMPI-D scales. Korean J Clin Psychol. 1991;10:98–113. [Google Scholar]
- 25.Brady MJ, Cella DF, Mo F, Bonomi AE, Tulsky DS, Lloyd SR, et al. Reliability and validity of the functional assessment of cancer therapy-breast quality-of-life instrument. J Clin Oncol. 1997;15:974–986. doi: 10.1200/JCO.1997.15.3.974. [DOI] [PubMed] [Google Scholar]
- 26.Yoo HJ, Ahn SH, Eremenco S, Kim H, Kim WK, Kim SB, et al. Korean translation and validation of the functional assessment of cancer therapy-breast (FACT-B) scale version 4. Qual Life Res. 2005;14:1627–1632. doi: 10.1007/s11136-004-7712-1. [DOI] [PubMed] [Google Scholar]
- 27.Aranda S, Schofield P, Weih L, Yates P, Milne D, Faulkner R, et al. Mapping the quality of life and unmet needs of urban women with metastatic breast cancer. Eur J Cancer Care (Engl) 2005;14:211–222. doi: 10.1111/j.1365-2354.2005.00541.x. [DOI] [PubMed] [Google Scholar]
- 28.Park BW, Hwang SY. Depression and coping in breast cancer patients. J Breast Cancer. 2009;12:199–209. [Google Scholar]
- 29.Northouse LL, Mood D, Kershaw T, Schafenacker A, Mellon S, Walker J, et al. Quality of life of women with recurrent breast cancer and their family members. J Clin Oncol. 2002;20:4050–4064. doi: 10.1200/JCO.2002.02.054. [DOI] [PubMed] [Google Scholar]
- 30.Wenzel LB, Fairclough DL, Brady MJ, Cella D, Garrett KM, Kluhsman BC, et al. Age-related differences in the quality of life of breast carcinoma patients after treatment. Cancer. 1999;86:1768–1774. [PubMed] [Google Scholar]