

Abstract
Aim:
To define the range of phase spread on equilibrium gated radionuclide ventriculography (ERNV) in normal individuals and derive the cut-off limit for the parameters to detect cardiac dyssynchrony.
Materials and Methods:
ERNV was carried out in 30 individuals (age 53±23 years, 25 males and 5 females) who had no history of cardiovascular disease. They all had normal left ventricular ejection fraction (LVEF 55–70%) as determined by echocardiography, were in sinus rhythm, with normal QRS duration (≤120 msec) and normal coronary angiography. First harmonic phase analysis was performed on scintigraphic data acquired in best septal view. Left and right ventricular standard deviation (LVSD and RVSD, respectively) and interventricular mechanical delay (IVMD), the absolute difference of mean phase angles of right and left ventricle, were computed and expressed in milliseconds. Mean + 3 standard deviation (SD) was used to derive the cut-off limits.
Results:
Average LVEF and duration of cardiac cycle in the study group were 62.5%±5.44% and 868.9±114.5 msec, respectively. The observations of LVSD, RVSD and right and left ventricular mean phase angles were shown to be normally distributed by Shapiro–Wilk test. Cut-off limits for LVSD, RVSD and IVMD were calculated to be 80 msec, 85 msec and 75 msec, respectively.
Conclusion:
Fourier phase analysis on ERNV is an effective tool for the evaluation of synchronicity of cardiac contraction. The cut-off limits of parameters of dyssynchrony can be used to separate heart failure patients with cardiac dyssynchrony from those without. ERNV can be used to select patients for cardiac resynchronization therapy.
Keywords: Cardiac dyssynchrony, equilibrium gated radionuclide ventriculography, interventricular mechanical delay, left ventricular ejection fraction, left ventricular standard deviation, right ventricular standard deviation
INTRODUCTION
Equilibrium gated radionuclide ventriculography (ERNV) is a non-invasive, reproducible and minimally operator-dependent study. ERNV has been used widely for the assessment of wall motion abnormalities and left ventricular ejection fraction (LVEF).[1] Fourier phase analysis on ERNV in addition provides valuable and accurate information of synchronicity of LV contraction.[2] Synchronicity of LV contraction is important for maintenance of adequate LVEF. Failing hearts are associated with abnormally coordinated contraction and relaxation. This loss of synchronous contraction is called LV dyssynchrony.[3–5] Since Fourier phase analysis is an effective tool for detecting dyssynchrony, ERNV can differentiate synchronous and dyssynchronous contraction of heart. Hence, we aim to establish the range of phase parameters in normal individuals and derive cut-off limits for parameters to detect cardiac dyssynchrony.
MATERIALS AND METHODS
This prospective study was conducted between April 2009 and April 2011.
Study population
The study group included 30 individuals (age 53±23 years, 25 males and 5 females) with no history of cardiovascular disease. They all had normal LVEF and wall motion (LVEF 55–70% on echocardiography), were in sinus rhythm, with normal QRS duration (≤120 msec) and either normal myocardial perfusion scintigraphy or normal coronary angiography.
Preparations for ERNV
The electrodes used for cardiac gating were secured on the skin in order to ensure an optimal ECG signal. The cardiac rhythm was noted to rule out marked heart rate variability that could interfere with the procedure and interpretation of ERNV results.
In vivo RBC labeling
20 microgram per kilogram body weight stannous pyrophosphate solution was injected intravenously. After 20 minutes, 25 mCi of Tc 99m pertechnate solution was injected intravenously. This allowed in vivo labeling of red blood cells (RBCs). Imaging was performed after a gap of 20 minutes.
Instrumentation
ERNV was performed using dual head GE Infinia Hawkeye 4 gamma camera with low-energy, high-resolution, parallel hole collimator interfaced to a dedicated computer. An appropriate ECG gating device was interfaced with the acquisition computer. The simultaneity of R wave triggered by the gating device and the QRS complex were verified before initiation of the study. A 15% R-R interval beat acceptance window was selected to include acceptable cardiac cycles.
Acquisition parameters
Thirty-two frames per R-R interval were obtained for assessment of ventricular wall motion, assessment of ejection fraction and phase analysis. Images were acquired so that the heart occupied ~50% of the usable field of view. Supine imaging was performed in a minimum of three views to visualize all walls of the left ventricle. The left anterior oblique (LAO) acquisition was obtained at an angle that allowed the best separation of the right and left ventricles (best septal or best separation view). A craniocaudal angulation of 10°–15°, for separation of atria from ventricle, was not given due to technical limitation of the newer gamma camera. Anterior acquisition and lateral acquisition were also obtained. A total of 6–7 million counts were acquired in the best septal view. Anterior and lateral views were acquired for 3 million counts. The data from best septal view were chosen for Fourier phase analysis.
Data processing
Scintigraphic data were processed on Xeleris Functional Imaging Workstation with the help of XT ERNA software. Automatic processing was performed on Laplacian images to define the end diastolic and end systolic frames. First harmonic phase analysis was performed to generate two-dimensional Fourier phase images. The result was a cosine curve characterized by its amplitude and phase angle. The phase angle referred to the timing or the placement of cosine curve within the cardiac cycle, from 0° to 360°. The earliest ventricular phase angle relates to the time of onset of the ventricular contraction, the mean ventricular phase angle reflects the mean time of the onset of the ventricular contraction and the standard deviation of the ventricular phase angle relates to the synchrony of the ventricular contraction.[6] The atria and ventricles are normally 180° out of phase. Phase angles were computed for each pixel and colored phase images with corresponding histograms were generated. Phase angle was converted to milliseconds by the formula: (phase angle/360 °) × RR interval (milliseconds). Mean phase angle and standard deviation (SD) were computed for right and left ventricles. The results were initially expressed in degrees and later converted to milliseconds [Figure 1a and b]. Interventricular mechanical delay (IVMD) was calculated by taking the absolute difference of mean phase angles of right and left ventricle. Mean + 3SD was considered as the cut off since it included 99.7% normally distributed population. The values were rounded to the nearest 5 msec. The parameters of cardiac dyssynchrony on ERNV were left ventricular standard deviation (LVSD), IVMD and right ventricular standard deviation (RVSD).
Figure 1.
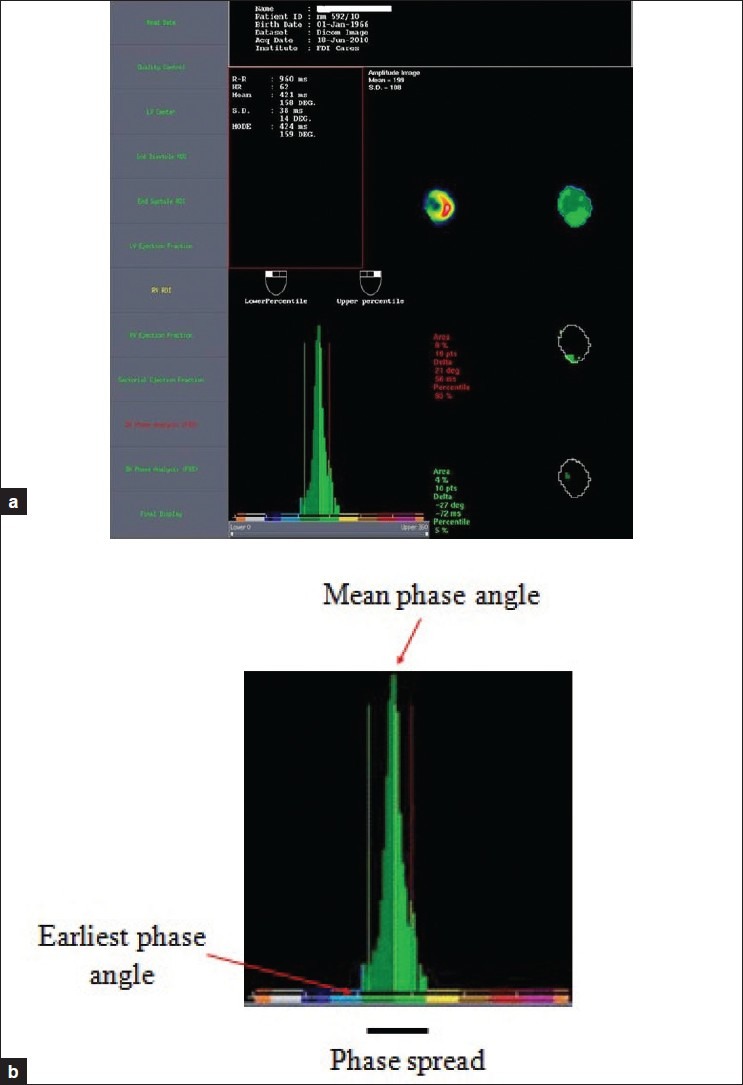
(a) First harmonic phase analysis of left ventricle (LV). Mean phase angle and standard deviation are represented in millisecond and degrees. Phase and amplitude images of LV are shown. The corresponding phase histogram is also seen in the picture. (b) A typical LV phase histogram showing earliest phase angle, mean phase angle and phase spread
Statistical analysis
The statistical analysis was performed on MedCalc 11.5.0 and Epiinfo 3.5.3.0 for the analysis of the data, and Microsoft word and Excel were used to generate graphs and tables. Descriptive statistical analysis was carried out in the present study. Results on continuous measurements were presented as Mean±SD and on categorical measurements as number (%). Shapiro–Wilk test was performed to test if the observations of phase parameters were normally distributed.
RESULTS
The study group [age 53±23 years, 25 (83%) males and 5 (17%) females] included normal individuals, selected according to the criteria mentioned in the section materials and methods. The mean LVEF of the study group was 62.5%±5.44%. The average R-R interval (duration of cardiac cycle) was 868.9±114.5 msec. It was observed that majority (≈83%) of study population belonged to the age group of 40–69 years [Figure 2].
Figure 2.

Age and sex distribution in the study population
Shapiro–Wilk normality test
This test was performed to evaluate the null hypothesis that the observations of LVSD, RVSD and the mean phase angles of left and right ventricles came from a normally distributed population.
The test statistic (W) was assessed at various thresholds of P value:
Threshold (P = 0.01) = 0.8999
Threshold (P = 0.05) = 0.9269
Threshold (P = 0.10) = 0.9390
If “W” was greater than P value, then the null hypothesis was accepted.
At thresholds of P = 0.01, P = 0.05 and P = 0.10, the Shapiro–Wilk statistic (W) was noted to be greater than the P value. Hence, null hypothesis was accepted for LVSD, RVSD, LV and RV mean phase angles. This suggested that the observations were normally distributed [Table 1].
Table 1.
Results of Shapiro–Wilk test on study group for parameters of dyssynchrony
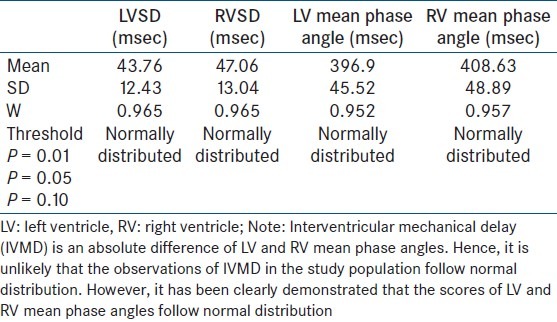
The average mean phase angles for left and right ventricles in normal individuals are 396.9±45.52 msec and 408.63±48.89 msec, respectively [Table 1]. The cut-off value for LVSD (mean + 3SD) is 80 msec. The cut-off value for RVSD (mean + 3SD) is 85 msec. Cut-off value for IVMD (mean + 3SD) is 75 msec [Table 2]. LVSD >80 msec should be considered significant for left intraventricular dyssynchrony. RVSD >85 msec should be considered significant for right intraventricular dyssynchrony. IVMD >75 msec should be considered significant for interventricular dyssynchrony.
Table 2.
Cut-off values for parameters of dyssynchrony

DISCUSSION
There are several imaging modalities for the evaluation of cardiac mechanical synchrony and LV function. Echocardiography (2D and 3D) is popular among all. Phase analysis on ERNV is known for decades and is grossly underutilized for the evaluation of cardiac dyssynchrony. Heart failure patients with LVEF ≤35%, symptomatic (NYHA III/IV) despite optimal pharmacological therapy and QRS duration >120 msec should be selected for cardiac resynchronization therapy (CRT) if significant cardiac mechanical dyssynchrony is detected, to get the best results. Cardiac mechanical dyssynchrony is prevalent in heart failure patients and predicts the response to CRT.[7–9] To separate the heart failure patients with dyssynchrony from those without, it is essential that we define the range of phase spread on ERNV and derive a cut-off limit for the parameters by using the locally available software.
The cut-off values for LVSD, RVSD and IVMD were determined to be >80 msec, >85 msec and >75 msec, respectively. Fauchier et al.,[10] in their study using ERNV, established the cut-off values for LVSD, RVSD and IVMD as >45 msec, >50 msec and >40 msec, respectively. The discrepancy in the cut-off limits between the studies could be explained by considering several factors. First, only 20 normal individuals of European descent were recruited in their study. Second, mean + 2SD was considered for setting the cut-off limit; while this study considered mean + 3SD. 2SD accounts 95.4% of normally distributed population, while 3SD accounts for 99.7%. Third, the software (XT ERNA) used for performing Fourier phase analysis in the present study was different from the one used in Laurent Fauchier's study. Fourth, in the present study, caudal tilt was not given during acquisition of scintigraphic data from the study population. The modern Infinia Hawk Eye 4 gamma camera of GE, unlike single head gamma camera, does not come with this facility. A caudal tilt of the gamma camera prevents overlap of left atrium over left ventricle. An overlap of left atrium over left ventricle might increase the left ventricular phase standard deviation. The cut-off values from the present study can further be validated by multicenter trials in India with the modern gamma camera, using the same XT ERNA based phase analysis of ERNV.
CONCLUSION
ERNV is a known effective, non-invasive and reproducible method of assessment of LVEF. Fourier phase analysis is a robust tool for the evaluation of synchronicity of cardiac contractility. The range of phase spread and cut-off limits defined in normal individuals can be used to distinguish heart failure patients with cardiac dyssynchrony from those without. The normative phase analysis data from the present study will be applicable to all those ERNV procedures performed with modern dual head gamma camera that does not allow a craniocaudal tilt. ERNV is useful for the assessment of LVEF, wall motion abnormalities and cardiac dyssynchrony, especially in those heart failure patients who may be potential candidates for CRT.
Study limitations
The cut-off limits from the present study need further validation from a larger sample size.
ACKNOWLEDGEMENT
Dr. AD Gowrishankar, MSc, MA, Med, PhD, retired Regional Joint Director of Collegiate Education, Government of Karnataka, is gratefully acknowledged.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.van Royen N, Jaffe CC, Krumholz HM, Johnson KM, Lynch PJ, Natale D, et al. Comparison and reproducibility of visual echocardiographic and quantitative radionuclide left ventricular ejection fractions. Am J Cardiol. 1996;77:843–50. doi: 10.1016/s0002-9149(97)89179-5. [DOI] [PubMed] [Google Scholar]
- 2.Fauchier L, Marie O, Casset-Senon D, Babuty D, Cosnay P, Fauchier JP. Interventricular and intraventricular dyssynchrony in idiopathic dilated cardiomyopathy: a prognostic study with Fourier phase analysis of radionuclide angioscintigraphy. J Am Coll Cardiol. 2002;40:2022–30. doi: 10.1016/s0735-1097(02)02569-x. [DOI] [PubMed] [Google Scholar]
- 3.Xiao HB, Brecker SJ, Gibson DG. Effects of abnormal activation on the time course of the left ventricular pressure pulse in dilated cardiomyopathy. Br Heart J. 1992;68:403–7. doi: 10.1136/hrt.68.10.403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Xiao HB, Lee CH, Gibson DG. Effect of left bundle branch block on diastolic function in dilated cardiomyopathy. Br Heart J. 1991;66:443–7. doi: 10.1136/hrt.66.6.443. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Cheng A, Helm RH, Abraham TP. Pathophysiological mechanisms underlying ventricular dyssynchrony. Europace. 2009;11(Suppl 5):510–4. doi: 10.1093/europace/eup272. [DOI] [PubMed] [Google Scholar]
- 6.Botvinick EH. Scintigraphic blood pool and phase image analysis: the optimal tool for the evaluation of resynchronization therapy. J Nucl Cardiol. 2003;10:424–8. doi: 10.1016/s1071-3581(03)00526-9. [DOI] [PubMed] [Google Scholar]
- 7.Emkanjoo Z, Esmaeilzadeh M, Mohammad Hadi N, Alizadeh A, Tayyebi M, Sadr-Ameli MA. Frequency of inter- and intraventricular dyssynchrony in patients with heart failure according to QRS width. Europace. 2007;9:1171–6. doi: 10.1093/europace/eum234. [DOI] [PubMed] [Google Scholar]
- 8.Fauchier L, Marie O, Casset-Senon D, Babuty D, Cosnay P, Fauchier JP. Interventricular and intraventricular dyssynchrony in idiopathic dilated cardiomyopathy: a prognostic study with Fourier phase analysis of radionuclide angioscintigraphy. J Am Coll Cardiol. 2002;40:2022–30. doi: 10.1016/s0735-1097(02)02569-x. [DOI] [PubMed] [Google Scholar]
- 9.Bax JJ, Bleeker GB, Marwick TH, Molhoek SG, Boersma E, Steendijk P, et al. Left Ventricular dyssynchrony predicts response and prognosis after cardiac resynchronization therapy. J Am Coll Cardiol. 2004;44:1834–40. doi: 10.1016/j.jacc.2004.08.016. [DOI] [PubMed] [Google Scholar]
- 10.Fauchier L, Marie O, Casset-Senon D, Babuty D, Cosnay P, Fauchier JP. Reliability of QRS duration and morphology on surface electrocardiogram to identify ventricular dyssynchrony in patients with idiopathic dilated cardiomyopathy. Am J Cardiol. 2003;92:341–4. doi: 10.1016/s0002-9149(03)00644-1. [DOI] [PubMed] [Google Scholar]