

Abstract
Bipolar dislocation of the clavicle at acromioclavicular and sternoclavicular joint is an uncommon traumatic injury. The conservative treatments adopted in the past is associated with redislocation dysfunction and deformity. A 41 years old lady with bipolar dislocation of right shoulder is treated surgically by open reduction and internal fixation by oblique T-plate at sternoclavicular joint and Kirschner wire stabilization at acromioclavicular joint. The patient showed satisfactory recovery with full range of motion of the right shoulder and normal muscular strength. The case reported in view of rarity and at 2 years followup.
Keywords: Bipolar dislocation, floating clavicle, internal fixation
INTRODUCTION
Bipolar dislocation of clavicle, was first reported by Poral in 1831.1 Scapinallium (2004)2 though collected 26 published cases yet it is considered a rare entity.
Although relatively minor trauma was also reported as the cause of bipolar dislocation, floating clavicle most principally results from major trauma which produces deforming force on the lateral aspect of shoulder or a severe pressure on the shoulder together with the torsion of the trunk.2
Nonsurgical treatment, adopted in the past, was highly recommended out of its easiness and low cost. However, redislocation, deformity, and dysfunction after conservative treatment are more and more emphasized. Open reduction and internal fixation (ORIF) gradually became the first choice of treatment for floating clavicle because it ensured better stability and earlier recovery.
We report a case with bipolar dislocation of clavicle, which was successfully treated by open reduction and internal fixation by oblique T-plate and Kirschner wires with 2 years followup demonstrating good outcome.
CASE REPORT
The patient was informed that the case would be presented for publication and she agreed.
A 41-year-old lady met with a car accident in June 2009 and was admitted to the hospital with the chief complaint of chest and back pain and restrictions of movements of right shoulder. During the accident, the patient was knocked down by a car when she was riding a motorcycle and trying to cross a street. She hit the ground with her right shoulder which suffered internal rotation and abduction. There was no history of coma, nausea, vomiting, respiratory distress, and shortness of breath.
Physical examination showed slight swelling and tenderness on the right shoulder. Sternoclavicular joint deformity [Figure 1] was also spotted. Piano key sign and thoracic squeeze sign were both positive. Active abduction and flexion were limited to 60°, while there was limitation of extension and adduction. Passive abduction was restricted to 90°. There was bruising at the back.
Figure 1.

Preoperative photograph of the patient, showing deformity at the right sternoclavicular joint with prominent medial end of the clavicle
Radiographic examination showed dislocation of right acromioclavicular joint and sternoclavicular joint, multiple rib fractures, and minor right pleural effusion [Figure 2a]. 3D CT reconstruction [Figure 2b] of the injured clavicle demonstrated posterior dislocation of the lateral end of the clavicle and anterosuperior dislocation of the sternoclavicular joint.
Figure 2.
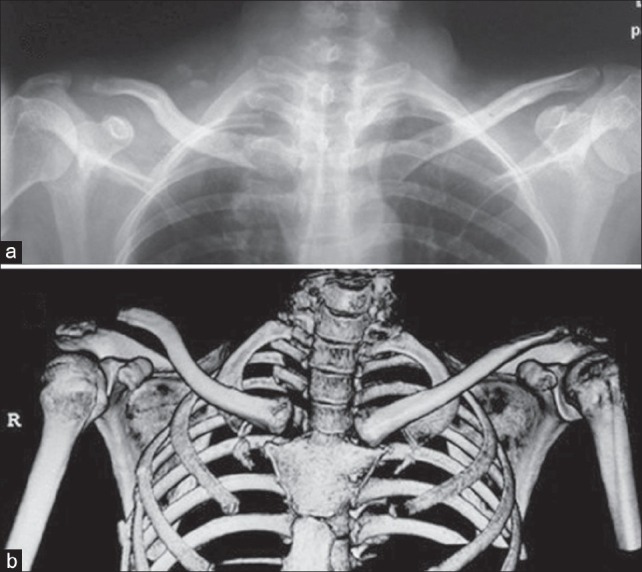
Preoperative (a) X-ray and (b) 3D CT reconstruction showing anterosuperior dislocation of the sternoclavicular joint and superioposterior dislocation of acromioclavicular joint
Open reduction and internal fixation was performed under general anesthesia through a 10-cm curved incision from acromian and a 5-cm horizontal incision on the right sternoclavicular joint. After exposure, superioposterior dislocation was at the acromio claviculer joint, while the medial end of the clavicle was found subluxed anteriorly and upward. Moreover, coracoclavicular ligament avulsion was also spotted. The sternoclavicular joint was fixed first. To relocate the clavicle, we firstly removed the adherent dense fibrous connective tissue in the joint space. Next, with a satisfied reduction of the clavicle, in the sternoclavicular joint, an oblique T-type steel plate was transfixed by four screws, while at the same time another lag screw was inserted from the superior surface of clavicle toward sternum [Figure 3a]. The acromioclavicular joint was fixed with two Kirschner wires (3.0mm). The wires were inserted from the lateral end of acromion, parallel to the articulation [Figure 3b]. Repair of the articular capsule and surrounding ligaments was then done.
Figure 3.
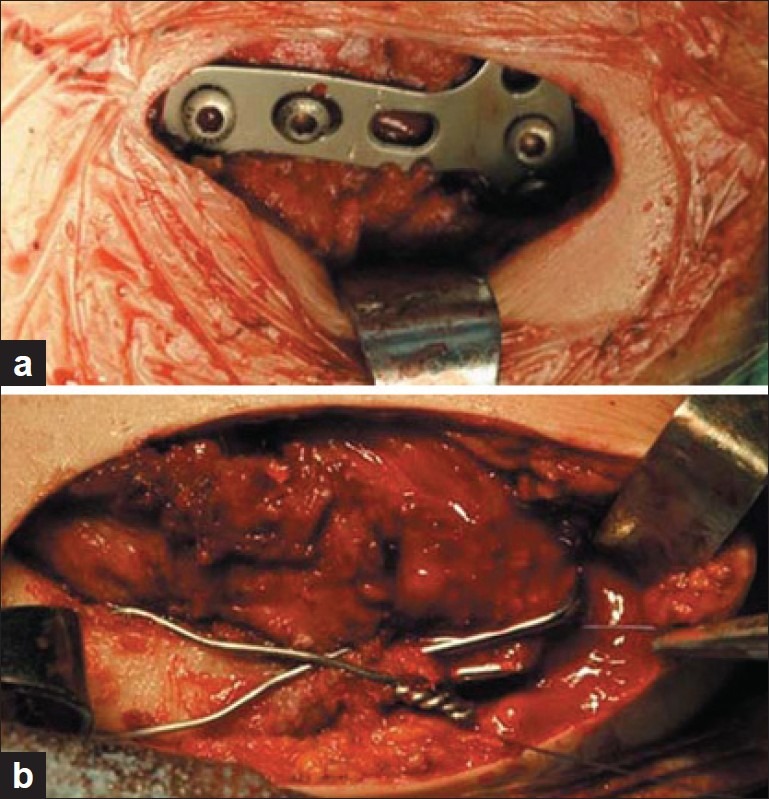
Intraoperative photograph showing the fixation of (a) sternoclavicular and (b) acromioclavicular joints with oblique T-plate and Kirschner wires, respectively
After wound closure, the patient was asked to wear an abduction device for a month. Passive motion exercises began after 1 week while the active ones began 2 weeks later. Removal of both Kirschner wires and plate was performed under general anesthesia 6 months after surgery. X-ray conducted 1 week [Figure 4a], 6 months [Figure 4b], 1 year [Figure 4c] and 2 years [Figure 4d] after the operation showed stable fixation and good relationship of both acromioclavicular and sternoclavicular joints. At 2 year followup, the patient had an abduction of approximately 150°, forward flexion of 160°, backward extension of 60°, and normal rotation [Figure 5a–c]. Besides, the power of the shoulder girdle muscles recovered and no instability of the dislocated joints was noted.
Figure 4.

X-ray followup (a) 1 week, (b) 6 months, (c) 1 year, and (d) 2 years after surgery shows normal alignment and good relationship of both joints
Figure 5.

Rehabilitation of joint abduction (a) flexion, (b) extension, and (c) rotation is satisfactory 2 years after surgery
DISCUSSION
In contrast to low-energy trauma like falling,3,4 bike riding,5 undoubtedly, a high-impact collision is considered the most common reason for bipolar clavicle dislocation.2,6–9 Two hypotheses have been suggested as the mechanism of the synchronous dislocation of both the joints. One theory suggests that elastic potential energy, originating from trauma related initial clavicle transformation, is released after the elimination of outer force, causing the synchronous dislocation of both acromioclavicular and sternoclavicular joints as well as the injury of ligaments.7 The other theory indicates that a backward violence firstly tears the articular capsule together with the acromioclavicular and coracoclavicular ligaments, causing a superioposterior dislocation of the lateral end of clavicle, and then elevates and pivots the medial end of clavicle from the first rib, causing the former to be dislocated anteriorly and upward.2,4,10
The conservative treatments including sling immobilization and plaster application appeared to be the preference by the most satisfactory outcome was reported in some of the cases, the residual pain, dysfunction and deformity resulting from various means of external fixation.2,5,7,11 Beckman6 tried for the first time to consolidate the articular capsule by suturing between periosteum and the surrounding soft tissue, but without an effective outcome. However, with the promising result brought about by the use of the Kirschner wires, reported by Echo6 and Benabdallah,7 more and more surgeons became interested in open surgical treatment which was characterized by simultaneous treatment at the two related joints.2,11 The following studies also proved that strong fixation not only ensures earlier rehabilitative training but also prevents deformity secondary to redislocation.8,9 Nevertheless, it could also cause unpredictable intra and postoperative complications. So, thorough considerations of surgery indications become critical. In general, surgery should be adopted in comparatively younger patients or patients with high requirement of their sport ability, as it guarantees better stability.
The use of Kirschner wires in sternoclavicular joint remains controversial, concerning their relatively inadequate stabilization which may contribute to higher risks of redislocation or subluxation as well as deformity. More seriously, the migration and rupture of Kirschner wires, which are not rare, could lead to severe complications such as hemorrhage threatening patient's life when part of it migrates into mediastinum, heart, or lung.12–14 Therefore, more reliable internal fixation is required in the case of sternoclavicular joint dislocation. Schemitsch et al.,9 had used Balser plate instead of Kirschner wires to fix the dislocation of sternoclavicular joint and achieved success, proving that the selection of implant material is the key to the therapy of bipolar dislocation. But in our opinion, T-plate is superior to other inter-fixation materials due to the following three reasons: Firstly, though is in a smaller size, it is stronger; secondly, it has high plasticity; and finally, it resembles skeleton owing to its elasticity modulus.
Our patient was young with high requirement of sport ability, we synchronously conducted bilateral internal fixation. On one hand, we used steel plate along with screws to deal with sternoclavicular joint first. On the other end, we fixed acromioclavicular joint with Kirschner wires joined and a figureof-eight tension band. Two years followup showed that the patient had satisfactory outcome with no signs of redislocation, good mobility, and no pain.
Footnotes
Source of Support: Nil
Conflict of Interest: None.
REFERENCES
- 1.Porral MA. Observation d’une double luxation de la clavicule droite. J Univ Hebd Med Chir Prat. 1831;2:78–82. [Google Scholar]
- 2.Scapinelli R. Bipolar dislocation of the clavicle: 3D CT imaging and delayed surgical correction of a case. Arch Orthop Trauma Surg. 2004;124:421. doi: 10.1007/s00402-004-0669-2. [DOI] [PubMed] [Google Scholar]
- 3.Eni-Olotu DO, Hobbs NJ. Floating clavicle–Similutaneous dislocation of both ends of clavicle. Injury. 1997;28:319–20. doi: 10.1016/s0020-1383(97)00009-0. [DOI] [PubMed] [Google Scholar]
- 4.Jain AS. Traumatic floating clavicle. A case report. J Bone Joint Surg Br. 1984;66:560–1. doi: 10.1302/0301-620X.66B4.6746693. [DOI] [PubMed] [Google Scholar]
- 5.Echo BS, Donati RB, Powell CE. Bipolar clavicular dislocation treated surgically. A case report. J Bone Joint Surg Am. 1998;70:1251–3. [PubMed] [Google Scholar]
- 6.Beckman T. A case of simultaneous luxation of both ends of the clavicle. Acta Chir Scand. 1924;56:156–63. [Google Scholar]
- 7.Benabdallah O. Bipolar luxation of the clavicle. Apropos of a case. Rev Chir Orthop Reparatrice Appar Mot. 1991;77:262–6. [PubMed] [Google Scholar]
- 8.Dieme C, Bousso A, Sane A, Sané JC, Niane M, Ndiaye A, et al. Bipolar dislocation of the clavicle or floating clavicle. A report of 3 cases. Chir Main. 2007;26:113–6. doi: 10.1016/j.main.2007.02.004. [DOI] [PubMed] [Google Scholar]
- 9.Schemitsch LA, Schemitsch EH, McKee MD. Bipolar clavicle injury: Posterior dislocation of the acromioclavicular joint with anterior dislocation of the sternoclavicular joint: A report of two cases. J Shoulder Elbow Surg. 2011;20:e18–22. doi: 10.1016/j.jse.2010.08.016. [DOI] [PubMed] [Google Scholar]
- 10.Cook F, Horowitz M. Bipolar clavicular dislocation. Report of a case. J Bone Joint Surg Am. 1987;69:145–7. [PubMed] [Google Scholar]
- 11.Sanders JO, Lyons FA, Rockwood CA. Management of dislocations of both ends of the clavicle. J Bone Joint Surg Am. 1990;72:399–402. [PubMed] [Google Scholar]
- 12.Nakayama M, Gika M, Fukuda H, Yamahata T, Aoki K, Shiba S, et al. Migration of a Kirschner wire from the clavicle into the intrathoracic trachea. Ann Thoracic Surg. 2009;88:653–4. doi: 10.1016/j.athoracsur.2008.12.093. [DOI] [PubMed] [Google Scholar]
- 13.Venissac N, Alifano M, Dahan M, Mouroux J. Intrathoracic migration of Kirschner pins. Ann Thoracic Surg. 2000;69:1953–5. doi: 10.1016/s0003-4975(00)01198-x. [DOI] [PubMed] [Google Scholar]
- 14.Wu YH, Lai CH, Luo CY, Tseng YL. Tracheoinnominate artery fistula caused by migration of a Kirschner wire. Eur J Cardio-Thoracic Surg. 2009;36:214–6. doi: 10.1016/j.ejcts.2009.03.043. [DOI] [PubMed] [Google Scholar]