

Abstract
Background:
Radiotherapy of head and neck cancers causes acute and chronic xerostomia and acute mucositis. Xerostomia increases risk of radiation caries and affects on oral comfort, fit of prostheses, speech, swallowing, and the growth of caries-producing organisms. Salivary flow rate can be measured by asking patients some questions. There are different types of commercial synthetic saliva such as BIOXTRA, but until now, no one can effectively relieve xerostomia. We tried to design a clinical research on BIOXTRA efficacy for treating xerostomia.
Materials and Methods:
In this research, 58 patients with head and neck cancer (except salivary gland cancers) treated in Seyed-al-Shohada Hospital. The patients received at least 40-50 GY; and after 2 months of compilation treatment, they were evaluated by asking about having xerostomia. Before and after treatment with the BIOXTRA, the PH of the oral cavity, candida albicans, and lactobacillus counts measured and documented in laboratory. We used BIOXTRA for 2 weeks, 3 times daily, and then re-evaluated patients with some questions.
Results:
The counts of candida albicans and lactobacilli statistically significant decreased.
Conclusion:
Xerostomia for most patients improved clinically during the day and night while PH of the oral cavity increased.
Keywords: BIOXTRA, radiotherapy, xerostomia
INTRODUCTION
Treatment end points for patients with malignant disease have historically been reflected by objective tumor response, overall survival and/or disease-free survival. However, over the past three decades, with the introduction of multi-modality treatments and the increasing number of cancer survivors, has come the growing awareness and concern for the psychosocial needs of patients with cancer.[1]
Head and neck cancers are 2.8% of all new cancer cases that almost 1/3rd of patients are women. Head and neck cancers have a fairly good chance to cure.
Because of certain head and neck anatomy, radiotherapy with or without chemotherapy of cancers is one of the main treatment modalities.[2]
There is both acute and long-term sequel of radiation therapy for head and neck cancers, which occurs due to effects on normal tissues. Permanent xerostomia is the most prevalent late side effect of RT for H&N cancers, and is a major cause of reducing quality of life. An alteration in taste can also occur, and decrease in oral intake may also contribute to decrease saliva production. Temporary loss of saliva, which is significant after delivery of 10 Gy to salivary glands while administration of approximately 40 to 50 Gy, causes permanent loss of their functions.[2,3]
Xerostomia is most marked when the amount of salivary mucous membranes moist is reduced by 50%.[4,5]
Decreased saliva causes dry mouth, tingling, decreasing sense of taste, difficulty swallowing dry foods, teeth caries, gum disease, bad breath, oral health costs, discomfort when using dentures, and increasing opportunities infections such as candida albicans.[6]
Patients asking many questions, can help identify and demonstrate reduce salivary gland function. A definitive answer to at least 1 of the following 4 questions can be indicated to reduce salivation.
-
(1)
Do you complain of dry mouth during the day or night?
-
(2)
Do you feel xerostomia in your mouth when you eat?
-
(3)
Do you use liquids for dry food ingestion?
-
(4)
Is it because of dry mouth you avoid talking to those around you?
Other methods include imaging techniques, and collecting saliva can also be used to measure it.[4,5,7]
Autoimmune diseases such as Sugren syndrm, HIV infection, and GVHD after bone marrow transplantation are other causes of xerostomia. Also, decreased saliva and immunoglobulin's abnormalities may be seen in people who have been used silicone breast implants.[8]
Patients with renal failure who are on hemodialysis are also suffering from reduced salivary gland function.[9]
Up to now, no effective treatment for dry mouth has been discovered.
Cholinergic drugs such as Pilocarpin can improve xerostomia, but they have many complications.[10,11]
Patients should be instructed to drink adequate fluids, rinse, and gargle with a weak solution of salt and baking soda several times a day (½ teaspoon of salt and 1 teaspoon of baking soda added to 1 quart of water). This regimen can refresh the mouth, loosen thick, tenacious oral secretions, and alleviate mild mucositis pain.[4–6]
Xerostomia often improves with time, but it is a long lasting and frequently permanent problem that adversely impacts quality of life. Commercially available salivary substitutes or artificial saliva (oral rinses containing hyetellose, hyprolose, or carmellose) relieve the discomfort of xerostomia by temporarily wetting the oral mucosa. Although they can provide temporary relief, especially prior to eating, many patients must take frequent sips of water to remain comfortable. In addition to being inconvenient, this can lead to secondary problems such as nocturia from late night fluid intake in men with prostatic hypertrophy and in men and women with small bladder capacity.[12]
A commercially available oral moisturizer (Optimoist) produces significant benefit for patients with H&N cancers undergoing radiation therapy.
MATERIALS AND METHODS
This study was a clinical randomized controlled trial (from 2008 to 2009), conducted in Radiation Oncology Department of Seyed-al-Shohada Hospital, Isfahan University of Medical Sciences, on some head and neck cancer patients, with no age and sex limitation that received at least 4000 cGY RT with parallel opposed field and daily fraction of 180 cGY.
Ethical approval was obtained from the local research ethics committee in school of medicine before recruitment. The study was performed in accordance with published guidelines and is reported in accordance with the CONSORT statement. Except salivary gland cancer, head and neck cancer patients were eligible for an enrolment. They received radiotherapy and went away at least 2 months from their treatment, but they would be excluded if they had diseases associated with xerostomia (such as autoimmune disease, connective tissue disease, etc.), used drugs which xerostomia is one of their side effects, and had a past history of radiotherapy in head and neck cancer region.
The main objective was to evaluate whether Bioxtra gel would improve radiation-induced xerostomia, lactobacillus colony count, candida albicans in the saliva cultures and oral cavity PH.
55 patients were defined as eligible patients. Written informed consent was recorded from subjects who agreed to participate.
The primary end-point was xerostomia, which was measured at the end of 2 weeks after finishing therapy. Candida albicans, lactobacillus colony count, and oral cavity PH measured as secondary end-points at the end of treatment for increasing power coefficient of xerostomia.
At the first day of treatment, xerostomia and saliva stream evaluated by some questions such as whether patients had complained of xerostomia during days or nights, felt xerostomia while eating, drank water for swallowing dry food and if avoided talking to people because of xerostomia. One absolute positive answer to at least one of these questions presents decreased saliva. Then, we used a special table for scoring in order from 0 to 1. Then, we tried to find the mean score of the patients and analyzed with Chi-square test.
The other options evaluated are basic PH with PH strip, basic lactobacillus colony count and candida albicans of the mouth in special cultures in laboratory. Then, patients were recommended to drink water when they need to and use ice chips to wet their mouth. Chewing gum, using lemon, avoidance of hot or cold and peppery food was also recommended.
Patients received 2 Bioxtra gel for 2 weeks (1 spoon, 3 times a day). They went for assessment of xerostomia, swallowing, and oral cavity examined for infections and teeth condition. After 2 weeks, xerostomia evaluated again by the same questions, and oral cavity PH, lactobacillus colony count and candida albicans checked in laboratory.
Qualitative results such as xerostomia were compared by using Chi-square test and quantitative results such as oral cavity PH, lactobacillus colony count and candida albicans used t-test.
RESULTS
Between 2008 and 2009, 55 head and neck cancer patients were evaluated for xerostomia. The average age of the patients was 54.9 +15.5 years (range: 19-82). 32 (58.2%) patients were males, and 23 (41.8%) were females. There was no significant difference between the mean ages of these 2 groups (P = 0.86).
In the evaluation of xerostomia before treatment with the Bioxtra gel, their most common symptom was xerostomia during the days and nights. The mean xerostomia score was 4.25 + 1.6.
For assessing the difference between male and female patients, Mann-Whitney test was used that indicated no significant difference between two sexes (P = 0.48). Also, in accordance to variance analysis, there was no association between xerostomia and age (P = 0.13).
In comparison with results before treatment, results of xerostomia evaluation after treatment are shown in Figure 1.
Figure 1.
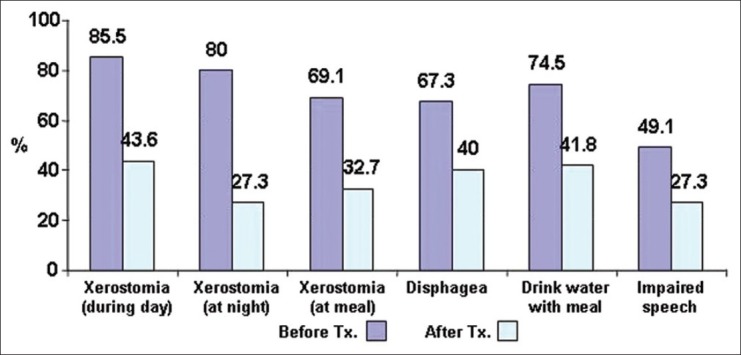
Frequency of xerostomia before and after treatment
In accordance to Vilkakson test on these data, the mean of xerostomia score was significantly lower after treatment (P = 0.004). In accordance to Mac nemar test, xerostomia during the day and night and speech impairment has significant difference, but xerostomia while eating and drinking water during a meal indicate no significant difference (P = 0.004 with SD = 1.67 before treatment and 1.19 after treatment).
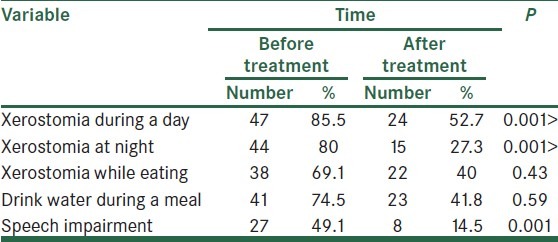
Comparing mean and standard deviation of xerostomia before and after treatment is shown in Table 1.
Table 1.
Comparing mean and standard deviation of xerostomia before end after treatment
To evaluate patients’ satisfaction of xerostomia treatment with Bioxtra gel, willing to continue using Bioxtra gel for the quality of life improvement, its taste satisfaction, and the feeling of xerostomia improvement were assessed. 39 patients (70.9%) were willing to continue taking it, 50 patients (90.9%) were satisfied with its taste, and xerostomia of 32 patients (58.2%) were improved.
The mean PH was 5.42 + 0.66 before treatment and 5.18 + 0.65 after treatment. In accordance to T-paired test, the PH of the mouth before and after the treatment indicates significant difference (P = 0.033).
The mean colony counts of candida albicans was 81515 + 23733 before treatment and 70303 + 27668 after treatment. In accordance to T-paired test, the number of colony counts of candida albicans indicates significant difference (P = 0.044).
The mean colony counts of lactobacillus was 8975 + 23695 before treatment and 84750 ± 25719 after treatment, but in accordance to T-paired test, the number of colony counts of lactobacillus indicates no significant difference (P = 0.23).
DISCUSSION
The present study indicates a significant superiority of Bioxtra gel for xerostomia during the day and a speech, but it doesn’t indicate significant effect in swallowing xerostomia because in this situation, we need more saliva flow, and Bioxtra cannot improve xerostomia with different scores.
If Bioxtra gel used for 2 weeks, resulted significant improvement in xerostomia, Shahdad et al. indicated in a study. The effects of Bioxtra and Bioten are evaluated in this study and showed that Bioxtra significantly improves xerostomia more than Bioten.[10]
Piet Dirix et al. in 2006 demonstrated that the use of Bioxtra gel after 4 weeks in head and neck cancer patients significantly decreased the xerostomia. In this study, mean of xerostomia, according to the VAS, was 59.8; and after the treatment, it became 36.4. As a result, the use of Bioxtra gel significantly improved the radiotherapy complications, especially xerostomia.[9]
In this study, Bioxtra gel increased the PH. Naturally. Decrease in oral cavity PH is one of the complications of xerostomia that causes chemical effects on oral cavity tissues and teeth, proliferation of organisms such as lactobacillus and candida that induced severe teeth caries and other side effects.
In a series of 24 patients, whole unstimulated salivary flow rate improved from 0.12 to 0.24 mL/min after 2 weeks of therapy. Candida colonization decreased in 43%, and swallowing objectively improved in 75% of subjects.[13] According to Dirix P et al. in 2007, 77% of patients improved after treatment with 32% had an excellent response. After treatment with Bioxtra, quality of life significantly increased than placebo and anyone had complications, although further studies of this drug use are considered essential.[14]
Shahdad et al., in double-blind randomized cross trial, evaluated effect of Bioxtra and Bioten on radiation-induced xerostomia. In this study, patients were randomly received Bioten for 2 weeks, they had a week break, and again, they received Bioxtra for 2 weeks or vice versa. After assessment the results, both drugs were effective, but the improvement in xerostomia and speech with Bioxtra was more than with Bioten.[15]
This gel could decrease lactobacillus counts and significantly decreased candida counts.[10]
Although these results can be advised to patients, more trials addressing this issue with this drug and the other kind of drugs need to be undertaken.
Due to high cost and lack of insurance, those drug combinations require long term treatment and have daily application. If the cost is reduced and the drug exposure is available, the patients’ quality of life will be improved.
Considering that there is still no cure for the relief of xerostomia caused by radiotherapy proven, as recommended routine, controlling is performed for xerostomia and compared with other drugs with different mechanisms.
Considering that xerostomia has undesirable effects on patients’ quality of life and available treatment has a temporary effect, using more advanced methods of radiotherapy to prevent or to reduce these complications is recommended.
CONCLUSIONS
The present results show that Bioxtra gel is effective in decreasing radiation-induced xerostomia, and treatment may be considered as the favorable therapy in head and neck cancer patients who received radiotherapy and have xerostomia.
ACKNOWLEDGMENTS
This study was supported by a grant from Isfahan University of Medical Science.
Footnotes
Source of Support: Isfahan University of Medical Science
Conflict of Interest: None declared
REFERENCES
- 1.Tschiesner U, Rogers SN, Harréus U, Berghaus A, Cieza A. Content comparison of quality of life questionnaires used in head and neck cancer based on the international classification of functioning, disability and health: A systematic review. Eur Arch Otorhinolaryngol. 2008;265:627–37. doi: 10.1007/s00405-008-0641-9. [DOI] [PubMed] [Google Scholar]
- 2.Perez CA. Brady's. Principles and practice of radiation oncology. 5th ed. Philadelphia: Lippincott Williams and Wilkins Company; 2008. pp. 2–137. [Google Scholar]
- 3.Jemal A, Murray T, Samuels A, Ghafoor A, Ward E, Thun MJ. Cancer statistics, 2003. CA Cancer J Clin. 2003;53:5–26. doi: 10.3322/canjclin.53.1.5. [DOI] [PubMed] [Google Scholar]
- 4.Ghezzi EM, Lange LA, Ship JA. Determination of variation of stimulated salivary flow rates. J Dent Res. 2000;79:1874–8. doi: 10.1177/00220345000790111001. [DOI] [PubMed] [Google Scholar]
- 5.Navazesh M, Christensen C, Brightman V. Clinical criteria for the diagnosis of salivary gland hypofunction. J Dent Res. 1992;71:1363–9. doi: 10.1177/00220345920710070301. [DOI] [PubMed] [Google Scholar]
- 6.Sreebny LM, Valdini A, Yu A. Xerostomia, part II: Relationship to nonoral symptoms, drugs, and diseases. Oral Surg Oral Med Oral Pathol. 1989;68:419–27. doi: 10.1016/0030-4220(89)90140-0. [DOI] [PubMed] [Google Scholar]
- 7.Fox PC, Busch KA, Baum BJ. Subjective reports of xerostomia and objective measures of salivary gland performance. J Am Dent Assoc. 2000;115:581–4. doi: 10.1016/s0002-8177(87)54012-0. [DOI] [PubMed] [Google Scholar]
- 8.International Dental Federation. Working Group 10 of the Commission on Oral Health, Research and Epidemiology (CORE). Saliva: Its role in health and disease. Int Dent J. 1992;42(4 supplement 2):287–304. [PubMed] [Google Scholar]
- 9.Loesche WJ, Bromberg J, Terpenning MS, Bretz WA, Dominguez BL, Grossman NS, et al. Xerostomia, xerogenic medications and food avoidances in selected geriatric groups. J Am Geriatr Soc. 1995;43:401–7. doi: 10.1111/j.1532-5415.1995.tb05815.x. [DOI] [PubMed] [Google Scholar]
- 10.Niedermeier WH, Kramer R. Salivary secretion and denture retention. J Prosthet Dent. 2002;67:211–6. doi: 10.1016/0022-3913(92)90455-j. [DOI] [PubMed] [Google Scholar]
- 11.Samaranayake LP. Host factors and oral candidosis. In: Samaranayake LP, MacFarlane TW, editors. Oral candidosis. London: Wright; 1990. pp. 66–103. [Google Scholar]
- 12.Braam PM, Roesink JM, Moerland MA, Raaijmakers CP, Schipper M, Terhaard CH. Long-term parotid gland function after radiotherapy. Int J Radiat Oncol Biol Phys. 2005;62:659–64. doi: 10.1016/j.ijrobp.2004.12.015. [DOI] [PubMed] [Google Scholar]
- 13.Rhodus NL, Bereuter J. Clinical evaluation of a commercially available oral moisturizer in relieving signs and symptoms of xerostomia in postirradiation head and neck cancer patients and patients with Sjögren's syndrome. J Otolaryngol. 2000;29:28–34. [PubMed] [Google Scholar]
- 14.Dirix P, Nuyts S, Vander Poorten V, Delaere P, Van den Bogaert W. Efficacy of Bioxtra dry mouth care system in the treatment of radiotherapy induced xerostomia rostomia. [Epub 2007 Jan 18];Support Care Cancer. 2007 15:1429–36. doi: 10.1007/s00520-006-0210-y. Available from: http://www.springerlink.com /content/k8781784w215v440 . [DOI] [PubMed] [Google Scholar]
- 15.Shahdad SA, Taylor C, Barclay SC, Steen IN, Preshaw PM. A double blind, crossover study of Biotene Oralbalance & Bioxtra systems as salivary substitutes in patient with post-raditherapy xerostomia. Eur J Cancer Care (Engl) 2005;14:319–26. doi: 10.1111/j.1365-2354.2005.00587.x. [DOI] [PubMed] [Google Scholar]