

Abstract
Background:
Doppler ultrasonography (DU) and measurement of its indexes, resistive index (RI) and pulsatility index (PI), is used to investigate transplanted kidney hemodynamic status and function. The aim of this study was to determine the correlation between Doppler indexes in the early phase after transplantation with long-term transplanted kidney function.
Materials and Methods:
In this cross-sectional study on 38 newly kidney transplant patients, we performed DU with assessment of its indexes within 48 hours, 1 week, and 6 months after kidney transplantation. Serum creatinine after stability and 6 months after kidney transplantation were assessed. Cyclosporine level was measured 1 week after kidney transplantation and compared with DU indexes.
Results:
About 71% of kidney transplanted patients reached their normal initial creatinine level(cr<1.5 mg/ dl) and 28% of all patients were involved in kidney dysfunction after 6 months (increase in basic creatinine level more than 25%).There was no significant difference between mean RI and PI in patients with normal and disturbed kidney function based on creatinine level in early posttransplantation period but there was linear correlation between mean RI and PI within 48 hours and 1 week with kidney function after 6 months. Also no association between cyclosporine level and RI and PI was shown. There was a direct association between age and the levels of RI and PI 6 months after transplantation.
Conclusion:
This study suggests assessment of RI and PI in early period after transplantation and can be used as predictive parameters for long-term function of transplanted kidney and RI more than 0.80 in early phase after transplantation has an acceptable sensitivity and specificity to predict long-term kidney dysfunction.
Keywords: Creatinine, Doppler indexes, Doppler ultrasonography, transplanted kidney
INTRODUCTION
Kidney transplant (KT) is a choice for patients with end stage renal failure that promotes their quality of life and diminishes morbidity. Although nowadays, transplanted patients’ survival has increased by modification of surgical techniques as well as intake of immunosuppressive drugs, detection of early KT complications plays a key role in transplantation success and patients’ survival.[1] Ultrasound and creatinine measurement are routine investigations of kidney function after transplantation and for detection of any complications. Ultrasound imaging is the main imaging method to detect any changes in shape of the transplanted kidney. This is a very safe method and without ionization and intravenous contrast to assess structure of the transplanted kidney compared with other methods.[2] Doppler ultrasonography is employed to assess the transplanted kidney better and to investigate vascular complications occurring in 1–10% of transplantations[1,3] as well as rare cases of renovascular hypertension and revascularization follow up. Doppler indexes [pulsatility index (PI) and resistive index (RI)] are measured in this method. These indexes are helpful parameters to quantify possible changes in kidney circulation due to other diseases involving the transplanted kidney. Therefore nowadays, Doppler method is vastly adopted to investigate transplanted kidney hemodynamic status and function through these indexes.[4–6] Radermarker et al. reported that RI was the best index to predict transplanted kidney dysfunction.[7] Although some researchers made predictive results of RI under question and not absolute,[8] in some other researches it was utilized as a prognostic marker with regard to the association of PI and RI with long-term function of transplanted kidney.[9] Some previous researches on acute rejection of a transplanted kidney showed that sensitivity and specificity of RI was low,[4] but it was shown in a study that measurement of RI shortly after transplantation can be utilized as a predictor for short-term function of a transplanted kidney.[10] Therefore, with regard to the existing controversy, the present study aims to investigate the correlation between Doppler indexes after transplantation with transplanted kidney function, and to define Doppler indexes cut off in diagnosis of transplanted kidney dysfunction.
MATERIALS AND METHODS
This is a cross-sectional study conducted on 38 end stage renal disease patients with mean age of 41.5 ± 13.8 years (range of 7–68 years) who underwent a kidney transplantation surgery in Alzahra hospital (Isfahan, Iran) from March 2011 to August 2011. All the patients underwent surgical anastomosis by end-to-end method. In this method end of donor kidney vessels connected to end of external iliac artery and vein of recipients. Laboratory studies included measurement of serum creatinine(colorimetry method mg/dl) and cyclosporine leve(monoclonal RIA ng/dl). The level of creatinine was measured daily up to a stable level for each patient and normal initial serum creatinine level was considered below 1.5 mg/dl after creatinine level stability.[11]
Level of cyclosporine was checked twice a week in the related center. Doppler sonography was performed for the patients 48 hours and a week after transplantation. It was performed by one radiologist by SIEMENS G60 (SIEMENS G60s,MODEL:7474922 Made in japan march 2006) device with curved probe of 3.5-5 MHz in patients’ supine position. Doppler indexes from interlobar arteries of upper, middle, and lower pole of transplanted kidney were calculated by equations 1 and 2 and the mean values of these were used.
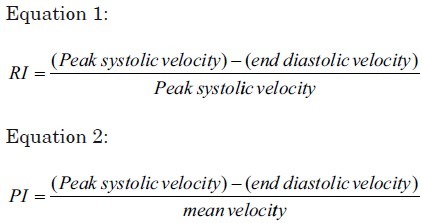
All the patients underwent Doppler ultrasonography 6 months after surgery and Doppler indexes were again calculated by equations 1 and 2. The creatinine level was also measured for them and an increase in basic creatinine level more than 25% was considered as renal dysfunction.[12] Exclusion criteria were acute rejection, perinephric fluid accumulation and moderate to severe hydronephrosis in transplanted kidney, renal artery and vein thrombosis, and significant stenosis of renal artery. Statistical analysis was done by SPSS statistical package software (version 18.0; SPSS_IBM). Independent t-test and Receiver operating characteristic (ROC) curve were employed to investigate the correlation between Doppler index and kidney function, and Doppler indexes cut off in diagnosis of kidney dysfunction, respectively. PI and RI values were based on mean ± SD, and P < 0.05 was considered significant. Pearson correlation test was employed to investigate the effect of recipients’ age on Doppler indexes.
RESULTS
There were 42 patients at the onset of study,3patients died and 1 patient missed, of 38 remnant cases there were 28 male and 10 female subjects attending this study. About 71% (27 patients) of the patients reached their normal initial creatinine level after creatinine level stability of whom 5 patients were involved in kidney dysfunction after 6 months. About 28%(11cases) of the patients never reached basic normal creatinine level of whom 6 patients had disturbed level of serum creatinine after 6 months. [Table 1] Mean RIs in the first 48 hours and a week after transplantation were 0.80 ± 0.092 and0.81±0.109in patients with kidney dysfunction after creatinine level stability, respectively. These values were higher than mean RIs at the same times for those with kidney normal function (0.74 ± 0.095, 0.74 ± 0.090) [Table 2]. Mean PIs in the first 48 hours and a week after transplantation in patients with initial kidney dysfunction was 1.76 ± 0.423, 1.67 ± 0.474, respectively. Mean PIs for those with normal kidney function at the same time were lower than those with kidney dysfunction [Table 2]. Independent t-test showed no significant difference between mean RI and PI in patients with normal and disturbed kidney function based on creatinine level in early posttransplantation period. Mean RIs in patients with 6 months kidney dysfunction (11 patients) in the first 48 hours, a week and 6 months after transplantation were 0.78 ± 0.086, 0.83 ± 0.052 and 0.84 ± 0.092, respectively, which were higher than values measured in patients with 6 months normal renal function (P < 0.05) [Table 3]. Mean PI in patients with transplanted kidney disturbed function after 6 months was significantly higher than the obtained values from those with normal renal function (P < 0.05) Table 3. In ROC curve analysis early 48 hours RI values of transplanted kidneys 0.80 was considered as cut off point for prediction long-term renal dysfunction with 63% sensitivity and 75% specificity [Table 4]. Mean cyclosporine level was 293 ± 68.6 at the end of the first week and Pearson correlation test showed no association between cyclosporine level, and RI and PI simultaneously. There was a direct association between age and the levels of RI and PI 6 months after transplantation [Figures 1 and 2].
Table 1.
Distribution of patients according to renal function based on initial and 6 months serum creatinine

Table 2.
RI and PI Mean values according to renal function in the early phase after transplantation
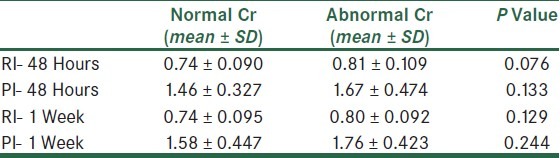
Table 3.
RI and PI Mean value according to renal function, 6 months after transplantation
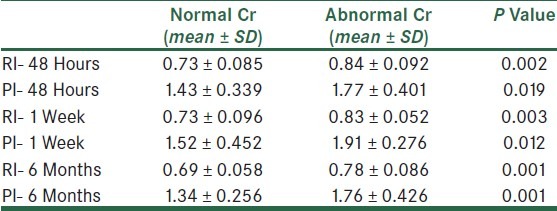
Table 4.
RI and PI cut off according to renal function, 6 months after transplantation
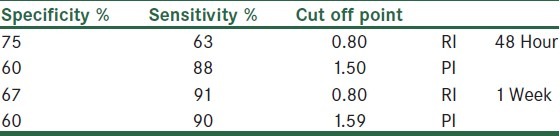
Figure 1.
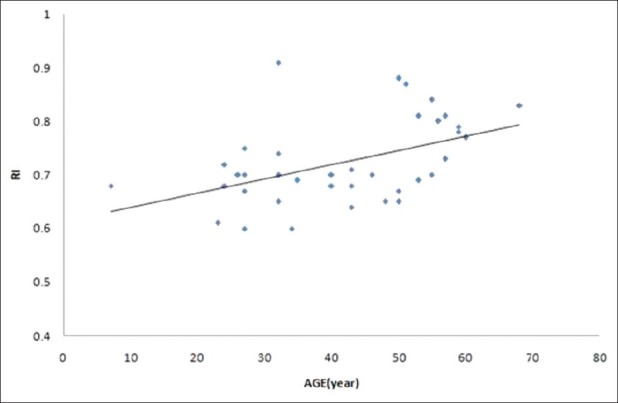
Correlation between age of recipients and 6 months PI
Figure 2.
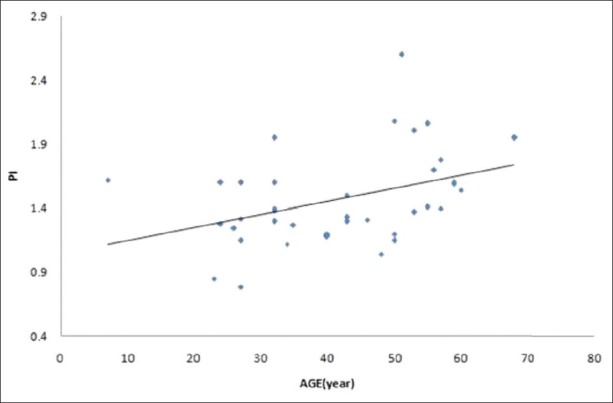
Correlation between age of recipients and 6 months RI
DISCUSSION
Results of this study shows that Doppler ultrasound and consideration of RI = 0.80 as a cut off, in the early phase after kidney transplantation, it could be used as a predictor of long-term kidney function. Sonography is a convenient noninvasive way to check transplanted kidneys in case of short- and long-term complications. In the acute stage, these complications include acute rejection, obstruction of urinary track accompanied with hydronephrosis, acute tubular necrosis (ATN), and renal artery and vein thrombosis for which gray scale and color Doppler sonography are diagnostic methods. RI is a parameter vastly used to assess kidney function.[4] Reduction of diastolic velocity due to an increase in renal resistance in the diseases involving the kidneys leads to RI increase. RI level is also under influence of various extra renal factors;[7] therefore, using RI as a mere element to distinguish various reasons of kidney dysfunction is of limited value.[13] Although RI increase at the very beginning is considered as a specific finding for transplant rejection, various studies have shown that RI increase lacks appropriate specificity.[5] There was no significant association found in RI and PI levels and transplanted kidney function at the early stage after transplantation based on creatinine level in the present study. Trillaud et al. showed that neither RI level nor power Doppler images can help in diagnosis of kidney dysfunction on the first day postsurgery.[14] Balbooaco et al. argued that there was a significant association between serum creatinine level and Doppler indexes on the 12th day postsurgery, but there was no such association on the 20th day.[15] The present study showed a direct association between levels of RI and PI in the first stage postsurgery and transplanted kidney function after 6 months based on serum creatinine level. Kahraman et al. showed that measurement of RI on the first week postsurgery can predict 1 month and 1 year function of transplanted kidney.[10] In a study conducted by McArthur, a significant correlation was reported between RI and PI levels, measured 1 week to 3 months posttransplantation, and transplanted kidney function 1 year after transplantation.[9] Radermarcher et al. in a prospective study showed that among various risk factors including recipient's and donor's age, proteinuria, arterial hypertension, and number of Human leukocyte antigen (HLA) mismatch, RI is the best predictor for transplanted kidney failure and recipients’ death.[7] Similar results were obtained in another study.[16,17]
Some researchers did not support the correlation between Doppler measurements and long-term function of a transplanted kidney.[11,14] In the present research, RI = 0.80 has been considered as cut off in prediction of kidney dysfunction 6 months after transplantation with sensitivity and specificity, presented values in Table 4. With regard to high RI level sensitivity 1 week after transplantation in diagnosis of kidney dysfunction, utilizing RI seems more appropriate to predict kidney dysfunction compared with measurement of RI in the first 48 hours after transplantation, similar results concerning PI values were obtained in the present study [Table 4]. Radermarcher et al. obtained sensitivity of 56% and specificity of 96% in measurement of RI = 0.80 3 months after transplantation.[7] McArthur et al. argued that the patients whose PI>1.49 or RI>0.74were measured between 1 week and 3 months after transplantation are at a higher risk of kidney dysfunction 1 year after transplantation.[9] A noticeable correlation between recipients’ age, and RI and PI 6 months after transplantation was shown in the present study. The main factor influencing RI is the recipients’ vascular compliance, which is affected by atherosclerotic changes related to age.[18] Heine et al. showed that RI is a complex factor, which is associated with cardiovascular risk factors such as vascular subclinical atherosclerotic changes.[8] The association between recipients’ age and Doppler indexes has been proved by other studies.[7,16,19] Despite vasospasm effect of cyclosporine on peripheral vascular of transplant kidney, no association was seen between cyclosporine level, and PI and RI in the present study. There was also no significant association between cyclosporine level in the patients with kidney dysfunction and those with normal kidney function based on creatinine level. A similar finding was reported in some other studies.[18–20] Meanwhile, Dopallo et al. claimed that an increase in cyclosporine level increase RI of the transplanted kidney.[13] Limitations of our study were the number of patients and course of follow up, it seems that evaluation of more cases in longer time will have better results
CONCLUSION
The obtained results in the present study showed that there was a correlation between RI and PI in early period of transplantation, and long-term function of transplanted kidney so that they can be used as predictive parameters for long-term function of transplanted kidney. RI = 0.80 has an acceptable sensitivity and specificity to predict long-term kidney dysfunction in early phase after transplantation. Hence, these patients need more care and follow up. These indexes are affected by recipients’ age within time.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Doppler ultrasound evaluation of renal transplant [homepage on the Internet] 2010. [Last accessed on 2011]. Available from: http://www.appliedradiology.com/Issues/2010/09/Articles/AR_09-10_Piyasena .
- 2.Al-khulaifat S. Evaluation of a transplanted kidney by Doppler ultrasound. Saudi J Kidney Dis Transpl. 2008;15:730–6. [PubMed] [Google Scholar]
- 3.Malfi B, Cogno C, Rabbia C, Messina M, Monga G, Mazzucco G, et al. Comparison between biopsy data and the resistive index obtained by Doppler echography in the evaluation of the transplanted kidney. Minerva Urol Nefrol. 1992;44:261–4. [PubMed] [Google Scholar]
- 4.Boas FE, Desser TS, Kamaya A. Does separating the resistive index into pre-and post glomerular resistance and vascular compliance improve the diagnostic accuracy of renal transplant Doppler ultrasound.? Am J Radiol. 2011;87:196–201. [Google Scholar]
- 5.Tublin ME, Bude RO, Platt JF. The resistive index in renal Doppler sonography: Where do we stand.? Am J Roentgenol. 2003;180:885–92. doi: 10.2214/ajr.180.4.1800885. [DOI] [PubMed] [Google Scholar]
- 6.Platt JF, Rubin JM, Ellis JH. Lupus nephritis: Predictive value of conventional and Doppler US and comparison with Serologic and biopsy parameters. Radiology. 1997;203:82–6. doi: 10.1148/radiology.203.1.9122420. [DOI] [PubMed] [Google Scholar]
- 7.Radermacher J, Mengel M, Ellis S, Stuht S, Hiss M, Schwarz A, et al. The Renal Arterial Resistance Index and Renal Allograft Survival. N Engl J Med. 2003;349:115–24. doi: 10.1056/NEJMoa022602. [DOI] [PubMed] [Google Scholar]
- 8.Heine GH, Gerhart MK, Ulrich C, Kohler H, Girndt M. Rental Doppler resistance indices are associated with systemic atherosclerosis in kidney transplant recioients. Kidney Int. 2005;68:87885. doi: 10.1111/j.1523-1755.2005.00470.x. [DOI] [PubMed] [Google Scholar]
- 9.McArthur C, Geddes CC, Boxter GM. Early measurement of pulsatility and resistive indexes: Correlation with long-term renal transplant function. Radiology. 2011;259:278–85. doi: 10.1148/radiol.10101329. [DOI] [PubMed] [Google Scholar]
- 10.Kahraman S, Genctoy G, Cil B, Yilmaz R, Arici M, Altun B, et al. Perediction of renal allograft function with early Doppler ultrasonography. Transplant Proc. 2004;36:1348–51. doi: 10.1016/j.transproceed.2004.05.030. [DOI] [PubMed] [Google Scholar]
- 11.Breitenseher M, Helbich T, Kainberger F, Hübsch P, Trattnig S, Traindl O, et al. Color Doppler ultrasound of kidney transplants.Does the resistance index facilitate diagnosis of chronic kidney Failure? Ultraschall Med. 1994;15:24–8. doi: 10.1055/s-2007-1004000. [DOI] [PubMed] [Google Scholar]
- 12.Gabriel MD. Handbook of Kidney Transplantation. 5th ed. Lippincott Williams and Wilkins; 2012. [Google Scholar]
- 13.Dipallo FQ, Rivolta R, Elli A, Castagnone D, Abelli P, Zafiropulu S, et al. Effect of cyclosporin A on renal cortical resistances measured by color Doppler flow metry on renal grafts. Nephron. 1993;65:240–4. doi: 10.1159/000187481. [DOI] [PubMed] [Google Scholar]
- 14.Trillaud H, Merville P, LeLinh PT, Palussiere J, Potaux L, Grenier N. Color Doppler Sonography in Early, Renal Transplantation Follow-Jp: ResistiveIndex MeasurementsVersus Power Doppler Sonography. Am J Radiol. 1998;171:1611–5. doi: 10.2214/ajr.171.6.9843297. [DOI] [PubMed] [Google Scholar]
- 15.Bolboaca SD, Lucan MD, Botar-Jid C, et al. European Congress of radiaology. Austria: 2004. Mar 5-9, Daily monitoring patients with renal transplant: A way to better understand to relationship between Doppler indices and renal function. [Google Scholar]
- 16.Saracino A, Santarsia G, Latorraca A, Gaudiano V. Early assessment of renal resistance index after kidney transplant can help predict long-term renal function. Nephrol Dial Transplant. 2006;21:2916–20. doi: 10.1093/ndt/gfl203. [DOI] [PubMed] [Google Scholar]
- 17.Akgul A, Lbis A, Sezar S, Basaran C, Usluogullari A, Ozdemir FN, et al. Early assessment of renal resistance index and long term renal function in renal transplantation recipients. Ren Fail. 2009;31:18–24. doi: 10.1080/08860220802546347. [DOI] [PubMed] [Google Scholar]
- 18.Krumme B, Grotz W, Kirste G, Schollmeyer P, Rump LC. Determinants of Intrarenal Doppler Indices in Stable Renal Allografts. J Am Soc Nephrol. 1997;8:813–6. doi: 10.1681/ASN.V85813. [DOI] [PubMed] [Google Scholar]
- 19.Nouri-Majelan N, Nafici R. Duplex sonographic, measurements in allografted kidneys: A cross-sectional study. Transplant Proc. 2007;39:1103–7. doi: 10.1016/j.transproceed.2007.03.039. [DOI] [PubMed] [Google Scholar]
- 20.Ardalan MR, Tarzamani MK, Mortaazavi M, Bahloli A. Relation between resistive index and serum creatinine level in first month after renal transplantation. Transplant proc. 2003;35:2628–9. doi: 10.1016/j.transproceed.2003.09.054. [DOI] [PubMed] [Google Scholar]