

Abstract
Goals & Background
Serum alanine aminotransferase (ALT) activity has been reported to be greater in the afternoon than the early morning, but data are scarce. We examined diurnal variation of ALT in a national population-based sample.
Study
Participants in the 1999–2008 U.S. National Health and Nutrition Examination Survey were randomly assigned to morning (AM) (n=4,474 adolescents, 11,235 adults) or afternoon/evening (PM) (n=4,887 adolescents, 11,735 adults) examinations. We examined ALT distributions graphically and compared both geometric mean ALT and the prevalence of elevated ALT, defined as >31 IU/L for adolescent boys, >24 IU/L for adolescent girls, >43 IU/L for adult men and >30 IU/L for adult women, between AM and PM examination groups.
Results
The examination groups were similar with the exception in the AM group of a longer fasting time and slightly higher prevalence of diabetes among adolescents and viral hepatitis B among adult women. ALT distributions were similar between examination sessions among the four groups. Among adolescents and men, neither mean ALT nor prevalence of abnormal ALT differed by examination group. Among women, mean ALT was statistically significantly, but minimally higher in the PM (19.6 IU/L) than the AM group (19.1 IU/L; p=0.009). Among one subgroup, women with chronic viral hepatitis, there was a higher prevalence of abnormal ALT in the PM (p=0.018 in unadjusted analysis). Adjusting for liver injury risk factors had little effect on the difference in mean ALT.
Conclusions
In general, clinically significant diurnal variation in ALT activity was not found in the U.S. population.
Keywords: liver enzymes, Circadian rhythm, National Health and Nutrition Examination Survey, epidemiology
INTRODUCTION
Serum alanine aminotransferase (ALT) activity is an important marker for liver disease. Significant diurnal variation in ALT activity may exist, with ALT concentrations of up to 45% higher in the afternoon than in the early morning, according to a recent review.1, 2 The existence of diurnal variation of ALT activity would have important clinical implications for screening, diagnosis, and monitoring of liver disease. However, data on diurnal variation of ALT are scarce. One study of ALT activity in chronic liver disease, in which 12 patients with cirrhosis of various etiologies underwent hourly blood sampling for 24 hours, found higher liver enzymes during the day than at night and a peak time in the afternoon.3 However, older studies found modest or no evidence for diurnal variation in ALT activity.4–8 To examine whether there are meaningful differences in ALT activities during the day, we investigated ALT activity among U.S. adolescents and adults in a national population-based sample that was randomly assigned to examination in the morning or in the afternoon or evening.
MATERIALS AND METHODS
The National Health and Nutrition Examination Survey (NHANES) is conducted in the United States by the National Center for Health Statistics (NCHS) of the Centers for Disease Control and Prevention (CDC) and since 1999 has been a continuous annual survey.9 It consists of cross-sectional interview, examination, and laboratory data collected from a complex multistage, stratified, clustered probability sample representative of the civilian, non-institutionalized population with oversampling of adolescents aged 12–19 years, persons age 60 years and older, African Americans, and Mexican Americans. Participants were randomly assigned to examination in the morning or to examination in the afternoon or evening. Participants randomized to a non-morning examination had the option of choosing the afternoon or evening examination. A small number of participants were assigned to a morning examination, but reported in the afternoon or evening. Because of confidentiality reasons, they could not be identified from the public use data and thus could not be excluded. The survey was approved by the CDC Institutional Review Board and all participants provided written informed consent to participate. The current analysis utilized data collected from 1999 through 2008.
Serum ALT activity was measured on participants 12 years and older. Of 47,346 persons sampled, 35,090 (74%) attended an examination at a mobile examination center. We excluded participants with missing data on serum ALT activity (n=2,759), resulting in an analysis sample of 9,361 adolescents aged 12–19 years and 22,970 adults aged 20 years and older. Because diurnal variation in ALT activity has been reported in chronic liver disease patients, secondary analyses were conducted among subgroups at high risk for liver injury: 1) 533 adults with viral hepatitis (positive serum hepatitis B surface antigen or positive serum hepatitis C antibody), 2) 7,079 obese adults (BMI ≥ 30 kg/m2 and waist circumference > 102 cm in men or > 88 cm in women); and 3) 1,997 obese adolescents (BMI ≥ 95th percentile of the 2000 CDC sex-specific BMI-for-age growth charts).10, 11 There were 446 adults with hepatitis C, 83 with hepatitis B, and 4 with both B and C. The number of adolescents with viral hepatitis (n=11) was insufficient for subgroup analysis.
A serum sample was collected and processed within one hour, frozen, and shipped weekly to testing laboratories. From 1999–2001 serum ALT activity was assayed by using a Hitachi model 917 multichannel analyzer (Roche Diagnostics, Indianapolis, IN) at the Coulston Foundation, Alamogordo, NM and from 2002–2008 by using a Beckman Synchron (LX20 and DxC800) (Beckman Coulter Inc., Fullerton, CA) at Collaborative Laboratory Services, L.L.C., Ottumwa, IA.12–18 ALT activity distributions did not differ between the Coulston Foundation Laboratory and Collaborative Laboratory Services.19 We considered ALT to be abnormal if higher than the 95th percentile among U.S. adolescents or adults not at high risk for liver injury (negative for viral hepatitis B and C, BMI < 85th percentile of the 2000 CDC sex-specific BMI-for-age growth charts10, 11 for adolescents or < 25 kg/m2 for adults, no doctor-diagnosed diabetes and hemoglobin A1C < 6.5%, and among adults, alcohol consumption ≤ 2 drinks per day among men and ≤ 1 drink per day among women and waist circumference ≤ 102 cm among men and ≤ 88 cm among women). These cut-offs were 31 IU/L for adolescent boys, 24 IU/L for adolescent girls, 43 IU/L for adult men and 30 IU/L for adult women.
Factors known or thought to be related to elevated ALT were included as covariates in multivariate analyses: age (years), BMI (kg/m2), doctor-diagnosed diabetes, elevated hemoglobin A1C (≥6.5%), serum total cholesterol concentration (mg/dL), and ethnicity (non-Hispanic white, non-Hispanic black, Mexican American, other). Other ethnicity included non-Mexican American Hispanics and other subgroups with insufficient numbers to study separately. Additional factors adjusted for among adults were waist circumference (cm), cigarette smoking (never, former, <1 pack/day, or ≥1 pack/day), viral hepatitis B (positive serum surface antigen) or C (positive serum antibody), and alcohol consumption. Participants were asked about frequency and quantity of alcohol drinking over the past 12 months from which drinks per day were calculated (drinks/day; 0, <1, 1–2, >2). Hepatitis B surface antigen was measured by using a solid-phase “sandwich” enzyme immunoassay (AUSZYME Monoclonal test, Abbott Diagnostics, Chicago, IL).21 Specimens were screened for HCV by the Ortho HCV enzyme-linked immunosorbent assay (ELISA), version 3.0 (Ortho-Clinical Diagnostics, Raritan, NJ) and positives tested with recombinant immunoblot assay (RIBA) (Chiron RIBA HCV Strip Immunoblot Assay, version 3.0, Chiron Corporation, Emeryville, CA) at the CDC.22–25 HCV RNA status was not available for all survey years, so was not used in this analysis. Caffeine consumption (mg/day), calculated for a subgroup of adults who underwent a dietary recall interview in 2001 to 2008 (n=18,010), was coded as deciles. The length of fast prior to venipuncture (hours) was also evaluated.
Statistical analysis
The median (interquartile range) time of blood draw for the morning, afternoon, and evening examinations, respectively, was 9:13 (8:48–9:54), 14:09 (13:42–14:47), and 18:12 (17:46–18:50). The time of blood draw for both afternoon and evening examinations fell within the peak time period that has been reported for ALT.3 Afternoon and evening examinations were, therefore, combined for this analysis and are referred to as “PM examinations” (69% of PM examinations took place in the afternoon). There was no difference between afternoon and evening examination groups with regard to mean ALT among adolescent boys (p=0.87), adolescent girls (p=0.20), adult men (p=0.42) or adult women (p=0.43). Likewise, prevalence of elevated ALT did not differ between afternoon and evening examination sessions among adolescent boys (p=0.78), adolescent girls (p=0.31), adult men (p=0.59) or adult women (p=0.41).
Because of sex differences in ALT activity, most analyses were conducted separately for males and females. Participant characteristics were compared by AM or PM examination session using a t-test for continuous characteristics and a Chi squared test for categorical characteristics. The distribution of ALT among AM and PM subgroups was examined graphically by plotting weighted percentiles. ALT was analyzed as both a natural log transformed (due to the skewed distribution) continuous variable, and back transformed to generate the geometric mean, and as a binary variable (normal, elevated). The geometric mean ALT and the prevalence of elevated ALT were first compared between AM and PM samples. To further examine the relation of ALT concentration with examination session while controlling for the effects of other factors related to abnormal ALT activity, multivariate regression analysis was used. Geometric mean ALT was compared using linear regression analysis (SUDAAN, PROC REGRESS, SUDAAN User’s Manual, Release 10.0, 2008; Research Triangle Institute, Research Triangle Park, NC) to calculate adjusted (least squares) mean estimates and 95% confidence intervals. The prevalence of elevated ALT was compared using logistic regression analysis (SUDAAN, PROC RLOGIST) to calculate adjusted odds ratio estimates and 95% confidence intervals. Multivariate analyses excluded persons with missing values for any factor included in the model. A p-value of <0.05 indicated statistical significance. All analyses utilized sample weights that accounted for unequal selection probabilities and non-response. All variance calculations took into consideration the design effects of the survey using Taylor series linearization.26 Analyses were conducted using SUDAAN software (SUDAAN User’s Manual, Release 10.0, 2008; Research Triangle Institute, Research Triangle Park, NC).
RESULTS
A total of 4,474 adolescents and 11,235 adults underwent examination in the AM and 4,887 adolescents and 11,735 adults in the PM. In keeping with random assignment to time of day of examination, persons examined in the AM and PM differed in very few characteristics (Table 1). Among adolescents, there was a trend toward a higher prevalence of doctor-diagnosed diabetes and/or elevated hemoglobin A1C in the AM group compared with the PM group, but the conditions were uncommon in both groups. Among adults, women in the AM group were more likely to have hepatitis B compared with those in the PM group, however, the prevalence was very low (<1%) among both groups. There were small differences in smoking status between men examined in the AM and PM. Serum total cholesterol was non-clinically significantly lower among both men and women in the AM group.
Table 1.
| a. Comparison of AM and PM samples of adolescents in the National Health and Nutrition Examination Survey, 1999–2008 | ||||||
|---|---|---|---|---|---|---|
| Boys |
Girls |
|||||
| Characteristic | AM (N=2,335) |
PM (N=2,417) |
p- value* |
AM (N=2,139) |
PM (N=2,470) |
p- value* |
| Age (years; mean (SD)) | 15.6 (2.3) | 15.4 (2.3) | 0.18 | 15.6 (2.2) | 15.4 (2.2) | 0.15 |
| Race-ethnicity (%) | 0.35 | 0.84 | ||||
| Non-Hispanic white | 60.9 | 61.7 | 62.1 | 60.3 | ||
| Non-Hispanic black | 15.4 | 13.6 | 14.7 | 14.9 | ||
| Mexican American | 11.2 | 11.9 | 11.4 | 11.5 | ||
| Other | 12.5 | 12.7 | 11.8 | 13.3 | ||
| Viral hepatitis (%) | ||||||
| B | 0.13 | 0 | 0.18 | 0.021 | 0.020 | 0.96 |
| C | 0.0086 | 0.013 | 0.77 | 0.043 | 0.065 | 0.77 |
| B or C | 0.14 | 0.013 | 0.20 | 0.065 | 0.085 | 0.79 |
| BMI (kg/m2; mean (SD)) | 23.2 (5.5) | 23.4 (5.5) | 0.40 | 23.5 (5.7) | 23.7 (5.7) | 0.38 |
| Waist circumference (cm; mean (SD)) | 81.4 (14.9) | 82.0 (14.7) | 0.43 | 80.6 (13.8) | 81.0 (13.5) | 0.60 |
| Doctor-diagnosed diabetes (%) | 1.1 | 0.29 | 0.058 | 0.65 | 0.18 | 0.064 |
| Hemoglobin A1C≥6.5% (%) | 1.0 | 0.33 | 0.051 | 0.50 | 0.10 | 0.046 |
| Abnormal glucose status (%)† | 1.3 | 0.42 | 0.054 | 0.72 | 0.25 | 0.075 |
| Serum total cholesterol (mg/dL; mean (SD)) | 158 (32) | 159 (31) | 0.33 | 164 (30) | 165 (31) | 0.44 |
| Fasting time (hours; mean (SD)) | 11.8 (3.7) | 7.3 (6.0) | <0.001 | 12.2 (4.4) | 7.2 (6.0) | <0.001 |
| b. Comparison of AM and PM samples of adults in the National Health and Nutrition Examination Survey, 1999–2008 | ||||||
|---|---|---|---|---|---|---|
| Men |
Women |
|||||
| Characteristic | AM (N=5,427) |
PM (N=5,614) |
p- value* |
AM (N=5,808) |
PM (N=6,121) |
p- value* |
| Age (years; mean (SD)) | 45.7 (16.3) | 45.6 (16.4) | 0.63 | 47.5 (17.2) | 46.9 (17.2) | 0.19 |
| Race-ethnicity (%) | 0.95 | 0.064 | ||||
| Non-Hispanic white | 71.8 | 72.0 | 71.4 | 71.1 | ||
| Non-Hispanic black | 9.6 | 9.8 | 11.8 | 10.8 | ||
| Mexican American | 8.5 | 8.3 | 6.8 | 7.2 | ||
| Other | 10.0 | 9.9 | 9.9 | 10.9 | ||
| Viral hepatitis (%) | ||||||
| B | 0.45 | 0.48 | 0.85 | 0.35 | 0.07 | 0.002 |
| C | 2.4 | 2.3 | 0.79 | 1.4 | 1.3 | 0.68 |
| B or C | 2.8 | 2.8 | 0.87 | 1.7 | 1.3 | 0.17 |
| Alcohol consumption (drinks/day; %) | 0.87 | 0.30 | ||||
| 0 | 23.5 | 24.2 | 35.9 | 34.6 | ||
| <1 | 52.9 | 52.1 | 56.4 | 58.3 | ||
| 1–2 | 13.3 | 13.6 | 6.0 | 5.6 | ||
| >2 | 10.3 | 10.1 | 1.7 | 1.5 | ||
| BMI (kg/m2; mean (SD)) | 28.2 (5.8) | 28.2 (5.6) | 0.95 | 28.3 (6.9) | 28.4 (7.2) | 0.48 |
| Waist circumference (cm; mean (SD)) | 100 (15.1) | 100 (14.7) | 0.95 | 93.8 (15.7) | 94.0 (16.1) | 0.68 |
| Doctor-diagnosed diabetes (%) | 7.4 | 7.5 | 0.85 | 7.4 | 7.3 | 0.90 |
| Hemoglobin A1C ≥6.5% (%) | 7.0 | 7.0 | 0.94 | 5.8 | 6.2 | 0.49 |
| Abnormal glucose status (%)† | 9.5 | 9.8 | 0.55 | 8.9 | 8.9 | 0.90 |
| Serum total cholesterol (mg/dL; mean (SD)) | 198 (42) | 200 (44) | 0.031 | 202 (42) | 203 (40) | 0.046 |
| Smoking (%) | 0.044 | 0.13 | ||||
| Never | 42.9 | 43.7 | 56.8 | 58.9 | ||
| Former | 29.8 | 28.8 | 22.8 | 20.2 | ||
| <1 pack/day | 14.1 | 15.5 | 12.7 | 12.8 | ||
| ≥1 pack/day | 13.2 | 12.0 | 7.7 | 8.1 | ||
| Fasting time (hours; mean (SD)) | 11.9 (4.1) | 6.9 (5.4) | <0.001 | 12.0 (3.9) | 6.7 (5.5) | <0.001 |
| Caffeine intake (mg /day; mean (SD))‡ | 218 (262) | 216 (254) | 0.77 | 165 (195) | 159 (209) | 0.31 |
SD, standard deviation
From chi-squared test for categorical variables or t-test for continuous variables.
Doctor-diagnosed diabetes or hemoglobin A1C≥6.5%.
Subgroup with dietary interview in NHANES 2001–08 (n=18,010).
One factor on which examination groups differed significantly was length of fast prior to blood draw (Table 1). Participants were asked to fast overnight if examined in the morning, but not if examined in the afternoon or evening. Consequently, the median (interquartile range) length of fast was 12.1 hours (10.7–13.7) among the AM sample and 6.3 hours (2.5–8.1) among the PM sample. However, length of fast was unrelated to ALT elevation. Mean (standard deviation (SD)) fasting time (expressed in hours) did not differ between participants with normal and abnormal ALT activity among any of the four groups: 9.5 (5.5) vs. 9.4 (5.5) (p=0.71) for adolescent boys, 9.5 (6.0) vs. 9.3 (5.2) (p=0.66) for adolescent girls, 9.3 (5.5) vs. 9.4 (5.1) (p=0.71) for adult men and 9.3 (5.5) vs. 9.1 (5.3) (p=0.38) for adult women. Fasting time remained unassociated with ALT among all demographic subgroups in univariate and multivariate models adjusted for factors included in Table 1 (data not shown).
ALT Comparisons Among Adolescents
With the exception of the upper extreme of the range, ALT activity distributions were similar between AM and PM examination sessions among adolescents (Figures 1–2). There were no differences in mean ALT or prevalence of elevated ALT between examination sessions among adolescents in unadjusted analyses (Table 2) or multivariate-adjusted analyses (data not shown). Similarly, ALT was unrelated to examination session among 1,997 obese adolescents (Table 2).
Figure 1.
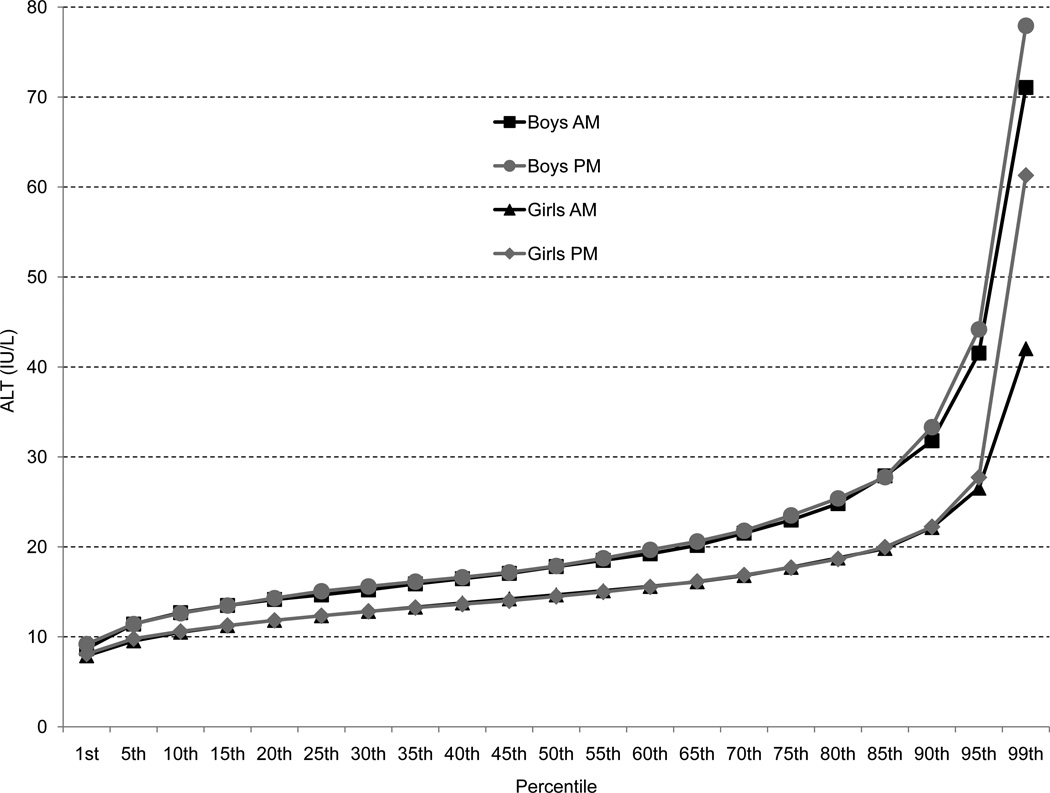
Distribution of serum alanine aminotransferase (ALT) activity among boys and girls according to examination in the AM or PM
Figure 2.
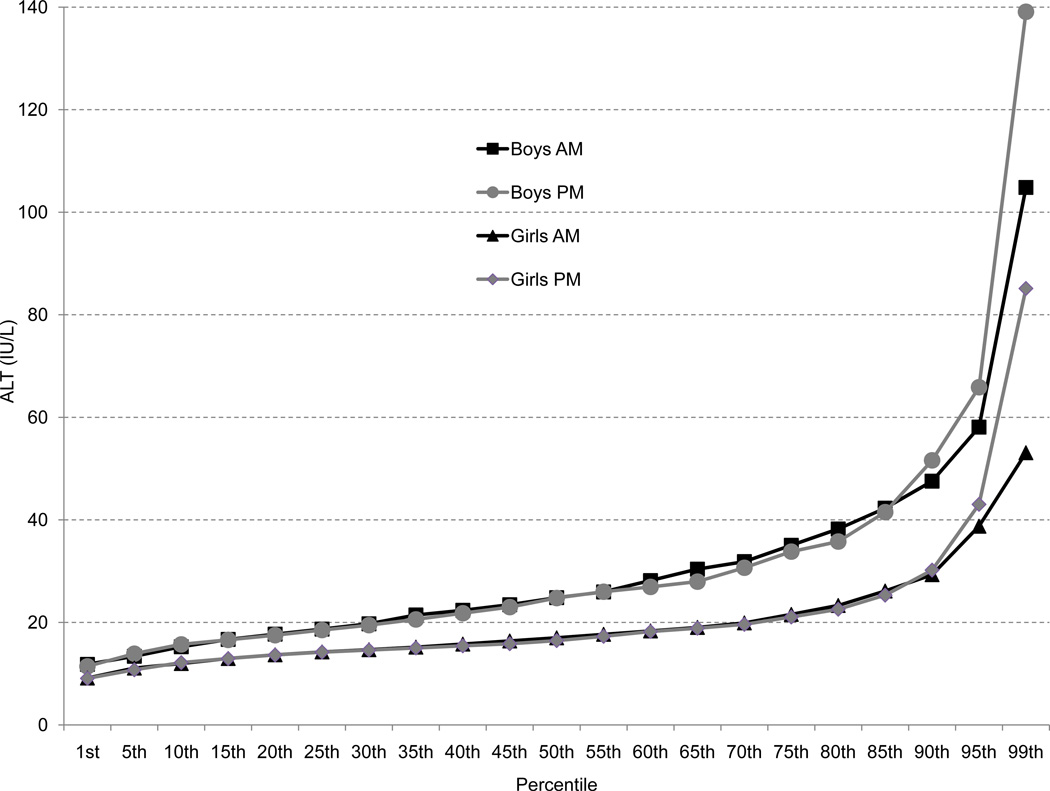
Distribution of serum alanine aminotransferase (ALT) activity among the subgroup of obese boys and girls according to examination in the AM or PM
Table 2.
Geometric mean* and prevalence of elevated serum alanine aminotransferase (ALT) activity† among AM and PM samples of all adolescents and adults and those at high risk for liver injury
| Mean ALT |
Elevated ALT |
||||||
|---|---|---|---|---|---|---|---|
| N | Geometric mean ± SE |
Difference ± SE |
p-value‡ | Prevalence (%) (95% CI) |
Difference ± SE |
p-value‡ | |
| Adolescents | |||||||
| All | |||||||
| Boys | |||||||
| AM | 2,335 | 19.6 ± 0.23 | 0.43 ± 0.33 | 0.19 | 10.8 (9.0 – 12.6) | 0.58 ± 1.3 | 0.65 |
| PM | 2,417 | 20.0 ± 0.25 | 11.3 (9.4 – 13.3) | ||||
| Girls | |||||||
| AM | 2,139 | 15.6 ± 0.14 | 0.14 ± 0.18 | 0.44 | 7.3 (5.7 – 9.0) | 0.50 ± 1.1 | 0.66 |
| PM | 2,470 | 15.8 ± 0.14 | 7.8 (6.4 – 9.3) | ||||
| Obese subgroup§ | |||||||
| Boys | |||||||
| AM | 471 | 26.9 ± 0.74 | 0.05 ± 1.2 | 0.96 | 32.5 (27.3 – 37.7) | 3.4 ± 4.5 | 0.45 |
| PM | 544 | 26.8 ± 0.86 | 29.1 (22.9 – 35.3) | ||||
| Girls | |||||||
| AM | 454 | 18.6 ± 0.34 | 0.09 ± 0.59 | 0.88 | 17.9 (12.3 – 23.4) | 0.77 ± 3.7 | 0.84 |
| PM | 528 | 18.7 ± 0.47 | 17.1 (12.6 – 21.6) | ||||
| Adults | |||||||
| All | |||||||
| Men | |||||||
| AM | 5,427 | 27.0 ± 0.19 | 0.11 ± 0.29 | 0.70 | 13.5 (12.4 – 14.7) | 0.91 ± 0.80 | 0.26 |
| PM | 5,614 | 26.9 ± 0.23 | 12.6 (11.4 – 13.8) | ||||
| Women | |||||||
| AM | 5,808 | 19.1 ± 0.13 | 0.47 ± 0.18 | 0.009 | 10.6 (9.5 – 11.8) | 1.5 ± 0.70 | 0.031 |
| PM | 6,121 | 19.6 ± 0.12 | 12.2 (11.3 – 13.0) | ||||
| Subgroup with viral hepatitis | |||||||
| Men | |||||||
| AM | 172 | 48.1 ± 3.4 | 3.6 ± 4.2 | 0.39 | 51.7 (43.1 – 60.3) | 2.6 ± 6.3 | 0.68 |
| PM | 166 | 44.5 ± 2.6 | 49.1 (39.4 – 58.8) | ||||
| Women | |||||||
| AM | 95 | 24.9 ± 2.1 | 9.3 ± 3.5 | 0.012 | 29.4 (12.6 – 46.1) | 28.7 ± 11.8 | 0.018 |
| PM | 100 | 34.2 ± 2.1 | 58.0 (46.4 – 69.7) | ||||
| Obese subgroup∥ | |||||||
| Men | |||||||
| AM | 1,401 | 32.0 ± 0.46 | 0.90 ± 0.68 | 0.19 | 23.4 (20.9 – 25.8) | 5.4 ± 1.8 | 0.004 |
| PM | 1,499 | 31.1 ± 0.49 | 17.9 (15.1 – 20.8) | ||||
| Women | |||||||
| AM | 2,031 | 20.8 ± 0.23 | 1.0 ± 0.38 | 0.008 | 14.8 (12.7 – 16.8) | 3.0 ± 1.5 | 0.052 |
| PM | 2,148 | 21.8 ± 0.28 | 17.8 (15.7 – 19.8) | ||||
SE, standard error; CI, confidence interval
Exponential of mean of log ALT.
>31 IU/L in adolescent boys, >24 IU/L in adolescent girls, >43 IU/L in adult men or >30 IU/L in adult women.
From a t-test.
BMI ≥95th percentile of 2000 CDC sex-specific BMI-for-age growth charts.
BMI ≥30 kg/m2 and waist circumference >102 cm for men or >88 cm for women.
ALT Comparisons Among Adults
The distribution of ALT activity was similar between AM and PM examination groups among adult men (Figure 3). There were no differences in mean ALT or prevalence of elevated ALT between examination sessions among men in unadjusted analyses (Table 2) or multivariate-adjusted analyses (data not shown). Likewise, among men at high risk for liver injury due to viral hepatitis B or C or to both overall and central adiposity, ALT was not higher with a PM examination (Table 2).
Figure 3.
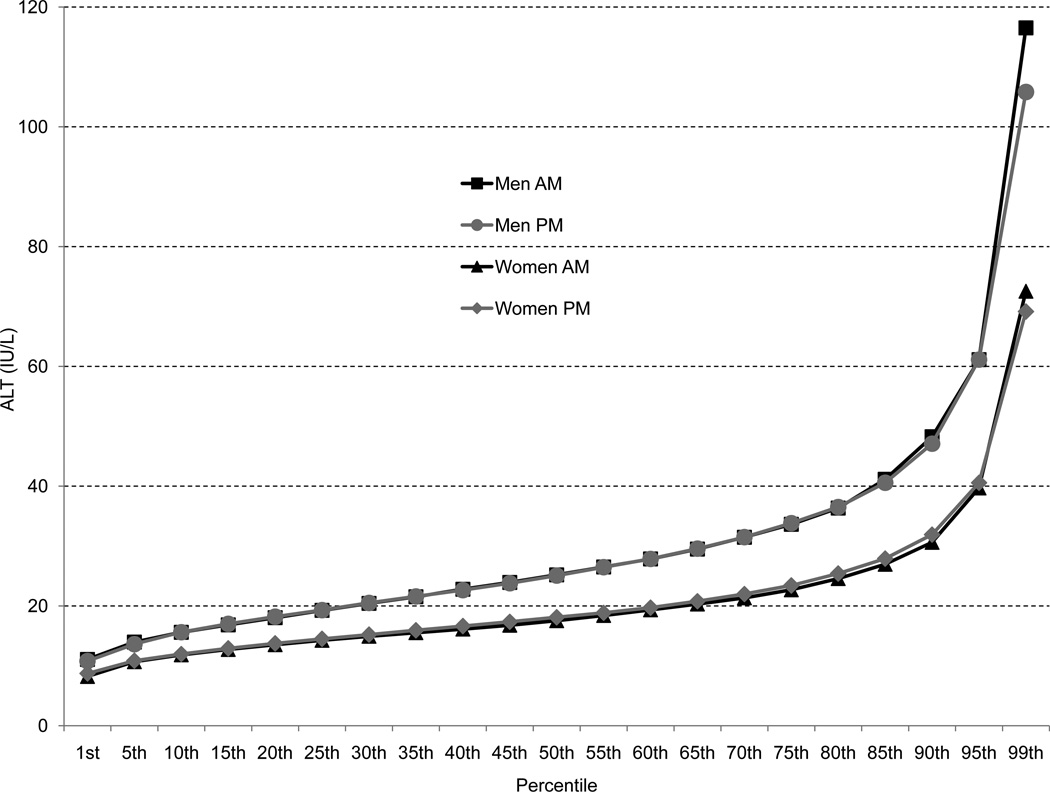
Distribution of serum alanine aminotransferase (ALT) activity among men and women according to examination in the AM or PM
Among adult women, the distribution of ALT activity was similar between AM and PM examination sessions (Figure 3). In contrast to adolescents and men, both mean ALT and prevalence of elevated ALT were slightly higher among women in the PM examination group compare with the AM group in unadjusted analyses (Table 2). In multivariate-adjusted analyses, women in the PM group had a higher mean ALT (p=0.022) and were 20% more likely to have an elevated ALT (p=0.034). Among women positive for viral hepatitis B or C, the relationship with examination session was more pronounced (Table 2). In multivariate analyses, mean ALT remained higher in the PM group (p=0.004), and the odds ratio for higher ALT activity in the PM was 5.7 (p<0.001). With the sexes combined, this difference in elevated ALT activity among participants with viral hepatitis diminished considerably, as is shown in Figure 4 and by the reduced, non-statistically significant odds ratio of 1.5 (p=0.16). Among women with viral hepatitis who had data on caffeine consumption, adding it to multivariate-adjusted models had little effect on the relationship of higher ALT with PM examination (data not shown). Women with both overall and central adiposity had statistically significantly, but minimally higher mean ALT, but not prevalence of elevated ALT, when examined in the PM in both unadjusted (Table 2) and multivariate-adjusted analyses.
Figure 4.
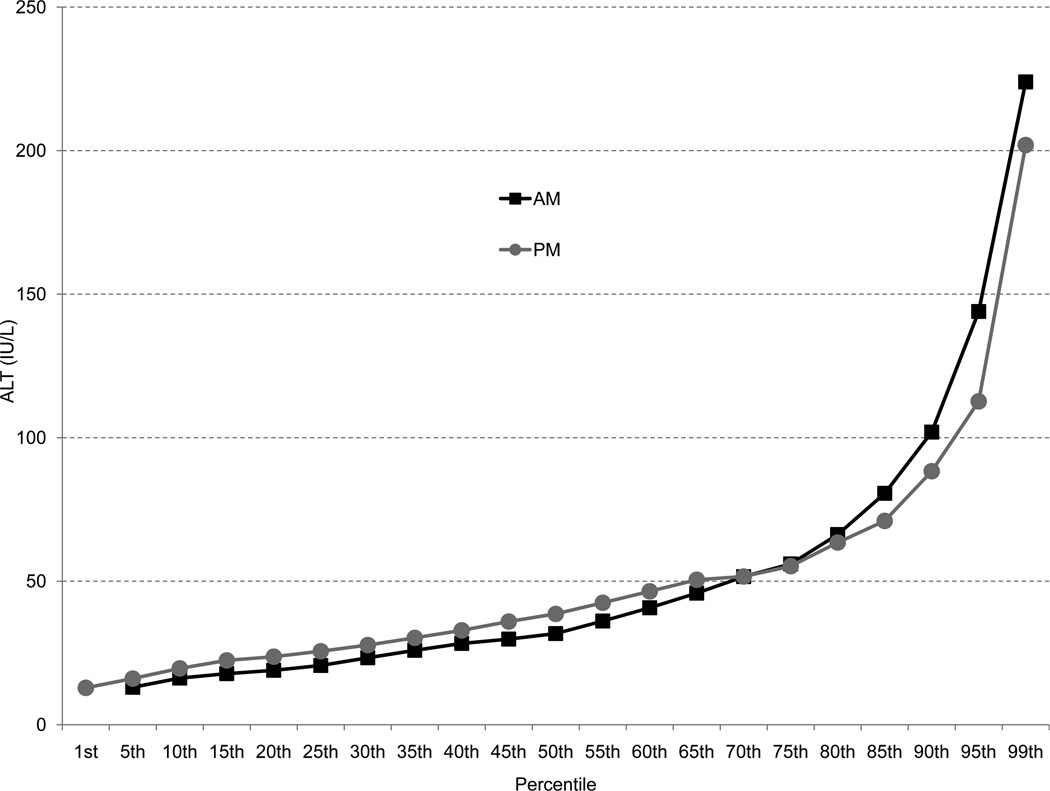
Distribution of serum alanine aminotransferase (ALT) activity among the subgroup of adults (men and women combined) with viral hepatitis according to examination in the AM or PM.
Because there is no universally agreed upon definition of abnormal ALT, we also conducted the analysis among adults using the often cited lower cut-offs for abnormal ALT derived using Italian blood donors of >30 IU/L for men and >19 IU/L for women.27 Lower cut-offs resulted in much higher prevalence of elevated ALT, but the relationships with examination session were similar to those of the main analysis for the entire sample and for subgroups with viral hepatitis or obesity (see Table, Supplemental Digital Content).
DISCUSSION
A number of factors, other than liver injury, may affect ALT activity, including time of day.28 Few data exist on diurnal variation in ALT levels and studies that have been done did not investigate men and women separately or included only men. ALT activity may be up to 45% higher in the afternoon than in the early morning according to a recent review, which may have been based on a brief report of a study among 12 patients with cirrhosis.1–3 Among presumably healthy persons, low amplitude variation was found in one study,8 while several small, but well-designed studies from the 1970s,4–6 and a more recent study7 found no such variation. The current large, national, population-based study does not provide support for clinically significant diurnal variation in ALT activity in the U.S. population. The one exception was a higher prevalence of elevated ALT activity among women attending the PM examination who had serological markers of chronic viral hepatitis. Although this anomalous result may deserve further investigation, the data collected in the current study do not permit further explanation for this finding. In any case, when men and women with viral hepatitis were analyzed together, little difference was found in the prevalence of elevated ALT activity.
Participants examined in the AM and PM were similar with regard to factors related to liver injury, except that women in the AM group were more likely to have viral hepatitis B. However, the prevalence of hepatitis B was low (<1%) among both examination groups. Furthermore, the anticipated effect if any would be a higher ALT activity among the AM sample, whereas women in the PM sample had slightly higher ALT levels in our analysis. One factor on which examination groups differed was fasting time. However, the length of fast was unrelated to ALT activity among adolescents and adults in both unadjusted and multivariate-adjusted analyses. Thus, there should be little concern about an influence of length of time since last food consumption on ALT activity.
A particular aspect of the design of NHANES, and a motivation for this study, is the random assignment to AM and PM examinations. While it is possible that participants differed by assignment in some unmeasured factors that could influence ALT activity, that was no more likely to occur in this study than in a randomized clinical trial. The small number of participants who were assigned to a morning examination, but reported in the afternoon or evening, and could not be identified and excluded due to confidentiality concerns was a limitation of the design. There could be some concern that the evening examinations could have lower ALT than the afternoon examinations. The majority of PM examinations occurred in the afternoon, and there was no statistically significant difference in ALT activity between afternoon and evening examinations, in keeping with the observations of a 24-hour study among 12 patients with cirrhosis.3 Day-to-day biological variation of ALT is known to occur;29, 30 therefore, reliance on a single ALT measurement was another limitation of the study. Inevitably, when ALT was categorized as normal or elevated, some participants were included in the elevated ALT group who would not have been had repeat ALT measurements been available. However, results were consistent with those for ALT analyzed as a continuous variable. More important was the inability to compare ALT activity at other times of the day. It is possible that more significant differences might have been found with earlier or later venipuncture. The limitation of a single ALT measurement is balanced by the benefits of a large, national, population-based sample, particularly the avoidance of ascertainment bias that can occur in clinical studies of selected patients and the ability to generalize the results to the U.S. population. Also, morning and afternoon, when the large majority of the examinations were conducted, are the times when patients typically have blood drawn. Nevertheless, future studies should measure ALT levels on the same persons throughout the day. A final limitation was the use of serology, rather than virology, to define HCV because HCV RNA was not available for all survey years (unavailable for 2003–2004), therefore, chronic HCV infection cannot be definitely excluded. However, false negative HCV antibody is uncommon.
As regards clinical implications of variation of ALT activity, there should be no concern that time of day of venipuncture would influence results among adolescents or men or asymptomatic women screened for liver injury. However, pending further studies, for women with known liver disease, the differences in ALT activity could be important if treatment and other decisions regarding care depended on detection of an abnormal ALT. In that case, it might be best to monitor ALT activity from samples collected at approximately the same time of day.
Supplementary Material
ACKNOWLEDGMENTS
The authors thank Vicki Burt and Jeffery Hughes of the National Center for Health Statistics for providing summary statistics on time of phlebotomy and Zhongyu Fang for her assistance with programming.
Source of Funding: This work was supported by a contract from the National Institute of Diabetes and Digestive and Kidney Diseases (HHSN267200700001G and HHSN276201200161U).
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Conflicts of Interest: The authors have no conflicts of interest.
Contributor Information
Constance E. Ruhl, Social & Scientific Systems, Inc., 8757 Georgia Avenue, 12th floor, Silver Spring, MD 20910, 301-628-3272 (phone), 301-628-3201 (fax), cruhl@s-3.com
James E. Everhart, National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health, Department of Health and Human Services, 2 Democracy Plaza, Room 655, 6707 Democracy Boulevard MSC 5450, Bethesda, MD 20892-5450, everhartj@extra.niddk.nih.gov
REFERENCES
- 1.Kim WR, Flamm SL, Di Bisceglie AM, et al. Serum activity of alanine aminotransferase (ALT) as an indicator of health and disease. Hepatology. 2008;47:1363–1370. doi: 10.1002/hep.22109. [DOI] [PubMed] [Google Scholar]
- 2.Dufour DR, editor. Laboratory Guidelines for Screening, Diagnosis and Monitoring of Hepatic Injury. Laboratory Medicine Practice Guidelines: National Academy of Clinical Biochemistry. 2000;20:1–60. [Google Scholar]
- 3.Cordoba J, O'Riordan K, Dupuis J, et al. Diurnal variation of serum alanine transaminase activity in chronic liver disease. Hepatology. 1998;28:1724–1725. doi: 10.1002/hep.510280640. [DOI] [PubMed] [Google Scholar]
- 4.Statland BE, Winkel P, Bokelund H. Factors contributing to intra-individual variation of serum constituents. 1. Within-day variation of serum constituents in healthy subjects. Clin Chem. 1973;19:1374–1379. [PubMed] [Google Scholar]
- 5.Morrison B, Shenkin A, McLelland A, et al. Intra-individual variation in commonly analyzed serum constituents. Clin Chem. 1979;25:1799–1805. [PubMed] [Google Scholar]
- 6.Panek E, Steinmetz J. The effect of sex, deviation from ideal weight and sampling time on blood constituents in presumably healthy subjects. Clin Chim Acta. 1979;92:343–351. doi: 10.1016/0009-8981(79)90212-2. [DOI] [PubMed] [Google Scholar]
- 7.Kanabrocki EL, Sothern RB, Scheving LE, et al. Reference values for circadian rhythms of 98 variables in clinically healthy men in the fifth decade of life. Chronobiol Int. 1990;7:445–461. doi: 10.3109/07420529009059156. [DOI] [PubMed] [Google Scholar]
- 8.Rivera-Coll A, Fuentes-Arderiu X, Diez-Noguera A. Circadian rhythms of serum concentrations of 12 enzymes of clinical interest. Chronobiol Int. 1993;10:190–200. doi: 10.3109/07420529309073887. [DOI] [PubMed] [Google Scholar]
- 9.NCHS. [Accessed on July 25, 2012];National Health and Nutrition Examination Survey (NHANES) Available at: http://www.cdc.gov/nchs/nhanes.htm.
- 10.Krebs NF, Himes JH, Jacobson D, et al. Assessment of child and adolescent overweight and obesity. Pediatrics. 2007;120(Suppl 4):S193–S228. doi: 10.1542/peds.2007-2329D. [DOI] [PubMed] [Google Scholar]
- 11.Kuczmarski RJ, Ogden CL, Guo SS, et al. 2000 CDC Growth Charts for the United States: methods and development. Vital Health Stat. 2002;11:1–190. [PubMed] [Google Scholar]
- 12.NCHS. [Accessed on July 25, 2012];NHANES 1999–2000 Laboratory Procedure Manual - Lab 18 Biochemistry Profile. Available from: http://www.cdc.gov/nchs/data/nhanes/nhanes_99_00/lab18_met_biochemistry_profile.pdf.
- 13.NCHS. [Accessed on July 25, 2012];NHANES 2001–2002 Laboratory Procedure Manual - Lab 18 Biochemistry Profile. Available from: http://www.cdc.gov/nchs/data/nhanes/nhanes_01_02/l18_b_met_biochemistry_profile.pdf.
- 14.NCHS. [Accessed on July 25, 2012];NHANES 2001-2002 Laboratory Procedure Manual - Lab 40 ALT. Available from: http://www.cdc.gov/nchs/data/nhanes/nhanes_01_02/l40_b_met_alanine_amino_transferase.pdf.
- 15.NCHS. [Accessed on July 25, 2012];NHANES 2003–2004 Laboratory Procedure Manual - Lab 40 ALT. Available from: http://www.cdc.gov/nchs/data/nhanes/nhanes_03_04/l40_c_met_alanine_amino_transferase.pdf.
- 16.NCHS. [Accessed on July 25, 2012];NHANES 2005–2006 Laboratory Procedure Manual - Lab 40 ALT. Available from: http://www.cdc.gov/nchs/data/nhanes/nhanes_05_06/biopro_d_met_alt.pdf.
- 17.NCHS. [Accessed on July 25, 2012];NHANES 2007–2008 Laboratory Procedure Manual - Alanine aminotransferase (ALT) - Beckman Synchron LX20. Available from: http://www.cdc.gov/nchs/data/nhanes/nhanes_07_08/ALT_BIOPRO_E_met_%20LX20.pdf.
- 18.NCHS. [Accessed on July 25, 2012];NHANES 2007–2008 Laboratory Procedure Manual - Alanine aminotransferase (ALT) - Beckman UniCel DxC800 Synchron. Available from: http://www.cdc.gov/nchs/data/nhanes/nhanes_07_08/ALT_biopro_e_met_DXC800.pdf.
- 19.NCHS. [Accessed on July 25, 2012];NHANES 2001–2002 Public Release Data File Laboratory 40 - Standard Biochemistry Profile, Follicle Stimulating Hormone, and Luteinizing Hormone. Available from: http://www.cdc.gov/nchs/data/nhanes/nhanes_01_02/l40_b_doc.pdf.
- 20.Executive summary: Standards of medical care in diabetes--2010. Diabetes Care. 2010;33(Suppl 1):S4–S10. doi: 10.2337/dc10-S004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.NCHS. [Accessed on July 25, 2012];NHANES 1999 –2000 Laboratory Procedure Manual - Hepatitis B Surface Antigen (HBsAg) Available from: http://www.cdc.gov/nchs/data/nhanes/nhanes_99_00/lab02_met_hep_b_antigen.pdf.
- 22.NCHS. [Accessed on July 25, 2012];NHANES 1999 –2000 Laboratory Procedure Manual - Hepatitis C Antibody / Hepatitis C Confirmatory. Available from: http://www.cdc.gov/nchs/data/nhanes/nhanes_99_00/lab02_met_hepatitis_c_%20eia_riba.pdf.
- 23.NCHS. [Accessed on July 25, 2012];NHANES 2001–2002 Laboratory Procedure Manual - Hepatitis C Antibody / Hepatitis C Confirmatory Test. Available from: http://www.cdc.gov/nchs/data/nhanes/nhanes_01_02/l02_b_met_hepatitis_c_eia_riba.pdf.
- 24.NCHS. [Accessed on July 25, 2012];NHANES 2005 –2006 Laboratory Procedure Manual - Hepatitis C Antibody / Hepatitis C Confirmatory Test. Available from: http://www.cdc.gov/nchs/data/nhanes/nhanes_05_06/hepc_d_met_hep_c_riba.pdf.
- 25.NCHS. [Accessed on July 25, 2012];NHANES 2007–2008 Laboratory Procedure Manual - Hepatitis C Antibody / Hepatitis C Confirmatory Test. Available from: http://www.cdc.gov/nchs/data/nhanes/nhanes_07_08/hepc_e_met_hep_c_RIBA.pdf.
- 26.Breslow NE, Day NE. Statistical methods in cancer research: the design and analysis of cohort studies: Lyon, France: International Agency for Research on Cancer. 1987:48–79. [PubMed] [Google Scholar]
- 27.Prati D, Taioli E, Zanella A, et al. Updated definitions of healthy ranges for serum alanine aminotransferase levels. Ann Intern Med. 2002;137:1–10. doi: 10.7326/0003-4819-137-1-200207020-00006. [DOI] [PubMed] [Google Scholar]
- 28.Dufour DR, Lott JA, Nolte FS, et al. Diagnosis and monitoring of hepatic injury. I. Performance characteristics of laboratory tests. Clin Chem. 2000;46:2027–2049. [PubMed] [Google Scholar]
- 29.Fraser CG. Biological variation in clinical chemistry. An update: collated data, 1988–1991. Arch Pathol Lab Med. 1992;116:916–923. [PubMed] [Google Scholar]
- 30.Lazo M, Selvin E, Clark JM. Brief communication: clinical implications of short-term variability in liver function test results. Ann Intern Med. 2008;148:348–352. doi: 10.7326/0003-4819-148-5-200803040-00005. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.