

Situs inversus is a rare congenital condition in which the position of major visceral organs is reversed.1–5 Management of an acute abdomen in such cases becomes difficult on account of the altered anatomy and the high risk of congenital heart conditions.
Case report
A 20-year-old lady presented to the emergency room with complaints of pain in the right lower chest and right upper abdomen, after being kicked in the chest by a horse few hours back. Her abdominal pain soon became generalized and she also complained of increased chest pain during inspiration. She gave no history of vomiting. On initial examination, she had tachycardia (98 beats per minute) and her blood pressure was 100/80 mmHg. Her respiratory rate was 20 per minute and decreased breath sounds were present on the right side. A bruise could be seen over her right lower chest and upper abdomen. Her abdomen was tense, tender and distended with absent bowel sounds. A provisional diagnosis of chest injury with liver injury following blunt trauma abdomen was made and resuscitation was started. Two large bore intravenous lines were secured and patient was given Ringer lactate solution. A Foley's catheter was introduced to assess the response to resuscitation.
A chest X-ray revealed the heart to be normal in position (apex on the left side) along fractures of the ninth and 10th ribs on the right side. There was no evidence of haemo-pneumothorax or any other bony injury on the X-ray (Figure 1). An ultrasound of the abdomen revealed moderate amount of free fluid in the abdomen with an injured spleen present in the right hypochondrium. Computerized tomography (CT) scan of the abdomen revealed a shattered spleen on the right side with a normal liver and gall bladder on the left side (Figure 2). The rest of the abdominal viscera appeared to be normal.
Figure 1.
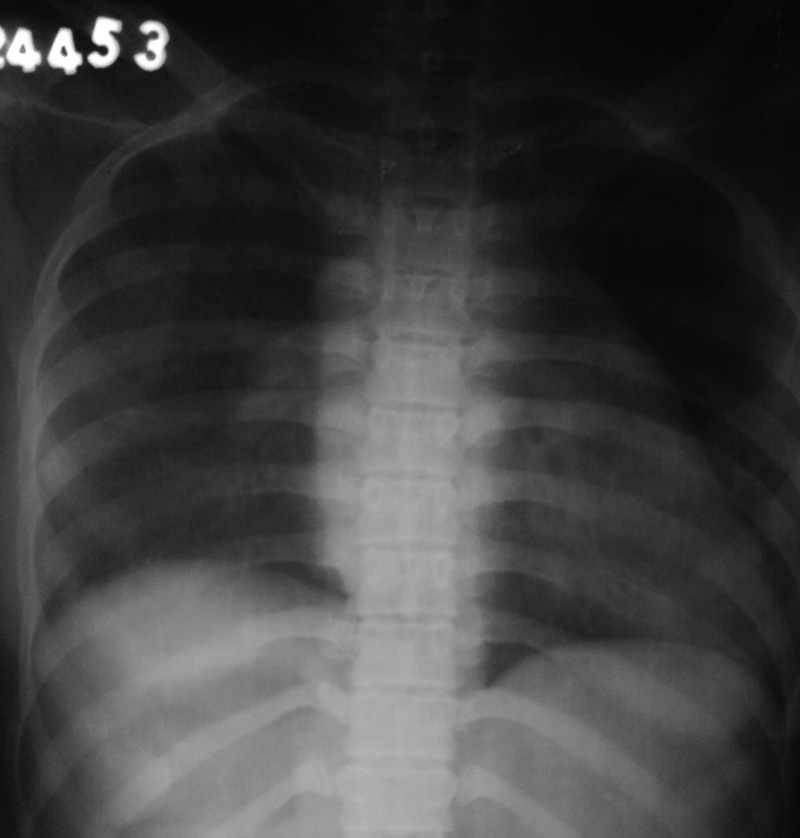
X-ray chest showing levocardia (cardiac apex on the left side of the thorax)
Figure 2.
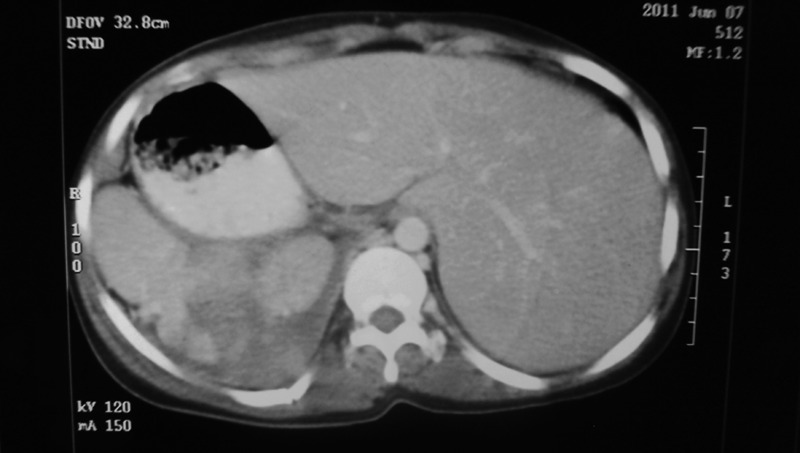
Computerized tomography scan showing a shattered spleen on the right side of the abdomen with liver on the left side
In view of the altered haemodynamic status of the patient, a decision was taken to carry out an emergency exploratory laparotomy. During laparotomy, 1.5 L of blood was evacuated from the peritoneal cavity and a shattered spleen was seen in the right hypochondrium with active bleeding. The splenic pedicle was intact and an emergency splenectomy was carried out. The liver and the other viscera were reversed in position but normal. The postoperative period was uneventful and the patient was discharged on the sixth postoperative day. Prior to discharge, the patient was immunized against Pneumococcus, Meningiococcus and Haemophilus influenzae.
Discussion
Situs inversus is a rare entity with an incidence of less than one in 10,000 people.2–4 Situs solitus is the normal position, and situs inversus is the mirror image of situs solitus. The cardiac situs is determined by the atrial location and in situs inversus, the right atrium is on the left, and the morphological left atrium is on the right. In addition to this, the position of major thoracic and abdominal viscera is also reversed. The liver and gall bladder are located to the left and the stomach and the spleen to the right. The classification of situs is independent of the cardiac apical position. The terms levocardia and dextrocardia only indicate the direction of the cardiac apex.2–6 Situs inversus with dextrocardia is also termed situs inversus totalis because the cardiac position as well as the atrial chambers and abdominal viscera are a mirror image of the normal anatomy.3–7
Situs inversus is generally an autosomal recessive genetic condition, although it can be X-linked. There is a 5–10% prevalence of congenital heart disease in individuals with situs inversus totalis, most commonly transposition of the great vessels.8 The incidence of congenital heart disease is higher in patients of situs inversus with levocardia (90%).2–3,8
In the absence of congenital heart defects, a person can lead a normal life without any complications related to the medical condition. Presence of situs inversus in patients leads to difficulty in diagnosis and management because of the altered anatomy. Anaesthetic complications may be increased in these patients on account of the high incidence of congenital heart lesions present in these patients.1–2,9
Although few cases of acute appendicitis and acute cholecystitis in patients with situs inversus have been reported,5–6,9–10 we could only find one case of splenic rupture following blunt trauma to the abdomen in our extensive search of the literature. Srivastava et al.2 reported a case of an 18-year-old man with situs inversus, who sustained a splenic injury following a fall from height and was managed by an emergency splenectomy. Our case had incomplete situs inversus without any congenital heart lesions and the condition was diagnosed by a contrast-enhanced CT scan performed for acute abdomen. Splenectomy was done on account of the high grade of splenic injury (Grade V) and the patient recovery was uneventful.
DECLARATIONS
Competing interests
None declared
Funding
No funding obtained
Ethical approval
Written informed consent to publish the article was obtained from the patient or next of kin.
Guarantor
RK
Contributorship
RK: Assisting surgeon and helped in preparation of manuscript. RC: Operating surgeon. LK, MS, PU: Assisting surgeons. SS, PG, AG: Helped in patient management and preparation of manuscript.
Acknowledgements
None
Reviewer
Antonella Ardolino
References
- 1.Lee SE, Kim HY, Jung SE Situs anomalies and gastrointestinal abnormalities. J Pediatr Surg 2006;41:1237–42 [DOI] [PubMed] [Google Scholar]
- 2.Srivastva V, Kumar P, Dosar S A case of splenic rupture in patient of situs inversus. Indian J Surg 2010;72(Suppl 1):326–7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Francisco RC, Casanova M Zulu Patient with situs inversus stabbed in the right flank. Internet J Surg 2009;20(1): [Google Scholar]
- 4.Holzmann D, Ott PM, Felix H Diagnostic approach to primary ciliary dyskinesia: a review. Eur J Pediatr 2000;159:95–8 [DOI] [PubMed] [Google Scholar]
- 5.Tiwari A, MacMull S, Fox S, Jacob SA Left sided abdominal pain in a patient with situs inversus. Clin Anat 2006;19:154–5 [DOI] [PubMed] [Google Scholar]
- 6.Kumar S, Fusai G Laparoscopic cholecystectomy in situs inversus totalis with left-sided gall bladder. Ann R Coll Surg Engl 2007;89:W16–18 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Gindes L, Hegesh J, Barkai G, Jacobson JM, Achiron R Isolated levocardia: prenatal diagnosis, clinical importance, and literature review. J Ultrasound Med 2007;26:361–5 [DOI] [PubMed] [Google Scholar]
- 8.Casey B Genetics of human situs abnormalities. Am J Med Genet 2001;101:356–8 [PubMed] [Google Scholar]
- 9.Lee SE, Kim HY, Jung SE, et al. Situs anomalies and gastrointestinal abnormalities. J Pediatr Surg 2006;41:1237–42 [DOI] [PubMed] [Google Scholar]
- 10.Karagülle E, Türk E, Yildirim E, Moray G A rare cause of left lower quadrant abdominal pain: acute appendicitis with situs inversus totalis. Ulus Travma Acil Cerrahi Derg 2010;16:268–70 [PubMed] [Google Scholar]